
Abstract
BACKGROUND AND PURPOSE: Extracranial vessel wall MRI (EC-VWI) contributes to vasculopathy characterization. This survey study investigated EC-VWI adoption by American Society of Neuroradiology (ASNR) members and indications and barriers to implementation.
MATERIALS AND METHODS: The ASNR Vessel Wall Imaging Study Group survey on EC-VWI use, frequency, applications, MR imaging systems and field strength used, protocol development approaches, vendor engagement, reasons for not using EC-VWI, ordering provider interest, and impact on clinical care was distributed to the ASNR membership between April 2, 2019, to August 30, 2019.
RESULTS: There were 532 responses; 79 were excluded due to minimal, incomplete response and 42 due to redundant institutional responses, leaving 411 responses. Twenty-six percent indicated that their institution performed EC-VWI, with 66.3% performing it ≤1–2 times per month, most frequently on 3T MR imaging, with most using combined 3D and 2D protocols. Protocols most commonly included pre- and postcontrast T1-weighted imaging, TOF-MRA, and contrast-enhanced MRA. Inflammatory vasculopathy (63.3%), plaque vulnerability assessments (61.1%), intraplaque hemorrhage (61.1%), and dissection-detection/characterization (51.1%) were the most frequent applications. For those not performing EC-VWI, the reasons were a lack of ordering provider interest (63.9%), lack of radiologist time/interest (47.5%) or technical support (41.4%) for protocol development, and limited interpretation experience (44.9%) and knowledge of clinical applications (43.7%). Reasons given by 46.9% were that no providers approached radiology with interest in EC-VWI. If barriers were overcome, 51.1% of those not performing EC-VWI indicated they would perform it, and 40.6% were unsure; 48.6% did not think that EC-VWI had impacted patient management at their institution.
CONCLUSIONS: Only 26% of neuroradiology groups performed EC-VWI, most commonly due to limited clinician interest. Improved provider and radiologist education, protocols, processing techniques, technical support, and validation trials could increase adoption.
ABBREVIATIONS:
- EC-VWI
- extracranial vessel wall MRI
- IP
- internet protocol
- ASNR
- American Society of Neuroradiology
Ischemic stroke is one of the leading causes of morbidity and mortality worldwide,1 and extracranial carotid atherosclerotic disease is a major contributor.2 Extracranial carotid vessel wall MRI (EC-VWI) has improved the understanding of plaque pathophysiology during the past 35 years and has the potential to change the focus of plaque analysis from luminal stenosis to plaque composition for clinical decision-making.3 The American Society of Neuroradiology (ASNR) Vessel Wall Imaging Study Group was developed to disseminate vessel wall imaging techniques, to educate the general neuroradiology community on their implementation and interpretation, and to influence vendors to improve vessel wall imaging techniques.3 While EC-VWI has been adopted at many institutions to assess extracranial vascular disease, primarily atherosclerosis, arterial dissections, and inflammatory vasculopathies, barriers may still exist for its implementation for others, including technology, knowledge or expertise limitations, or vendor relations or workflow challenges. The ASNR membership represents the primary group of clinicians likely to benefit from the advances in EC-VWI in their clinical practice. Hence, the current survey study aimed to poll the ASNR membership on whether their institutions were performing EC-VWI, and if not, what barriers exist to its implementation and use. For institutions performing EC-VWI, we aimed to evaluate applications of the technique, which sequences were being used, how the techniques were developed, levels of clinician interest, and vendor collaboration for the development of the technique. To our knowledge, this is the first survey of the ASNR membership on EC-VWI use.
MATERIALS AND METHODS
This study is the extracranial portion of a survey administered, for which the intracranial portion had previously been published.4 The survey was discussed at ASNR Vessel Wall Imaging Study Group meetings and developed through input by multiple Study Group members. Through an iterative review process, the final survey was developed on the SurveyMonkey (https://www.surveymonkey.com/) platform. The survey was built with logic, and if a respondent indicated that he or she did not perform EC-VWI, the individual skipped to the last 4 questions of the EC-VWI portion of the survey, focused on barriers to EC-VWI performance and interest of the ordering provider (the questions in the survey are provided in the Online Supplement Data). Respondents who indicated that their institution did perform EC-VWI were expected to answer each EC-VWI question in the survey. After University of Washington institutional review board review, the survey received institutional review board exemption. The anonymous survey was first sent to the ASNR Vessel Wall Imaging Study Group and was opened to the group from March 30, 2018, through April 17, 2018, for revisions and approval. After approval from the ASNR Executive Committee, the survey was then sent to the ASNR membership on April 2, 2019. A second reminder was sent to the membership on August 14, 2019. Responses were gathered between April 2, 2019, and August 30, 2019, after which the survey was closed. Individuals could respond to the survey only once.
After the collection of survey responses, response quality was assessed, with exclusion of surveys in which the respondent spent <20 seconds on the survey and responded to ≤1 question. Internet Protocol (IP) addresses of the respondents were reviewed to determine the institution of origin for the response. For institutions with multiple responses, partially completed responses were excluded. If there was >1 complete response for an institution, the study investigators reviewed the institutional responses to assess accuracy on the basis of their knowledge of protocol and clinical performance based on publications, presentations, and/or personal knowledge of the specific institution at the time of the survey to determine the single institutional response to include. If this issue was yet unresolved, discussion with EC-VWI leaders at the particular institution was performed for clarification on their approach at the time of the survey, and the survey response that most closely approximated this was kept. IP addresses without institutional associations were not excluded. IP addresses were also used to determine the region from which the response came. Responses were grouped into continent, country, and, for US responses, region of the country, divided on the basis of US Census definitions.5 For question 31 regarding obstacles to performing EC-VWI, responses were tabulated individually but also grouped into educational responses and technical responses. Any response that included no clinician interest, limited personal knowledge of applications/value, limited expertise of interpretation, no benefit for the patient population, or lack of evidence supporting the benefit were placed in the education category. Any response that included no radiologist time/interest for protocol development, no vendor/technical support for protocol development, long scan times limiting clinical feasibility, or lack of standardized protocols were placed in the technical category.
RESULTS
Respondents
The survey was distributed to 5552 ASNR members through 2 e-mails from the ASNR separated by 3 weeks, and 1854 individuals opened the e-mails. A total of 46 respondents were from the ASNR Vessel Wall Imaging Study Group, and 486 respondents were from the ASNR membership, for a total of 532 responses. The response rate was 9.6%. Respondents, on average, spent 11 minutes on the survey, and there was an 86% completion rate. We subsequently excluded survey responses for which <20 seconds was spent on the survey and the respondent answered 1 or no questions (n = 79), leaving 453 complete responses. Redundant institutional responses were then removed (n = 42), leaving 411 included responses.
Of the included responses, 81.3% were from North America, 7.5% from Europe, 5.8% from Asia, 3.6% from South America, 1.0% from Australia, and 0.7% from Africa. For countries, the United States had the most included responses, with 314, followed by Canada (n = 16), Brazil (n = 12), and South Korea (n = 5). For the 314 US responses, 30.3% were from the South; 24.5%, from the Midwest; 24.5%, from the East; and 20.7%, from the West. Of the 114 responses with institutional IP addresses, 52.6% were academic, 38.6% private practice, 5.3% federal, and 3.5% hybrid institutions.
EC-VWI Utilization
Most reported VWI performance either 1 to 2 times per month (29%) or once every couple of months (24%), though responses ranged from only a handful of times ever performed (13%) to at least twice per week (17%) (Fig 1). EC-VWI was most frequently performed as an add-on ordered by ordering providers (60.2%, 53/88), stand-alone ordered by providers (46.6%, 41/88), or an add-on from radiologists (46.6%, 41/88) (Fig 2). In the free text option, 3 respondents indicated that the technique was performed only for research.

Question: If your institution performs carotid vessel wall MR imaging, on average how often? There were 89 respondents with 89 responses.

Question: Is carotid vessel wall MR imaging clinically being performed as (answer all that apply)? There were 88 respondents with 161 responses.
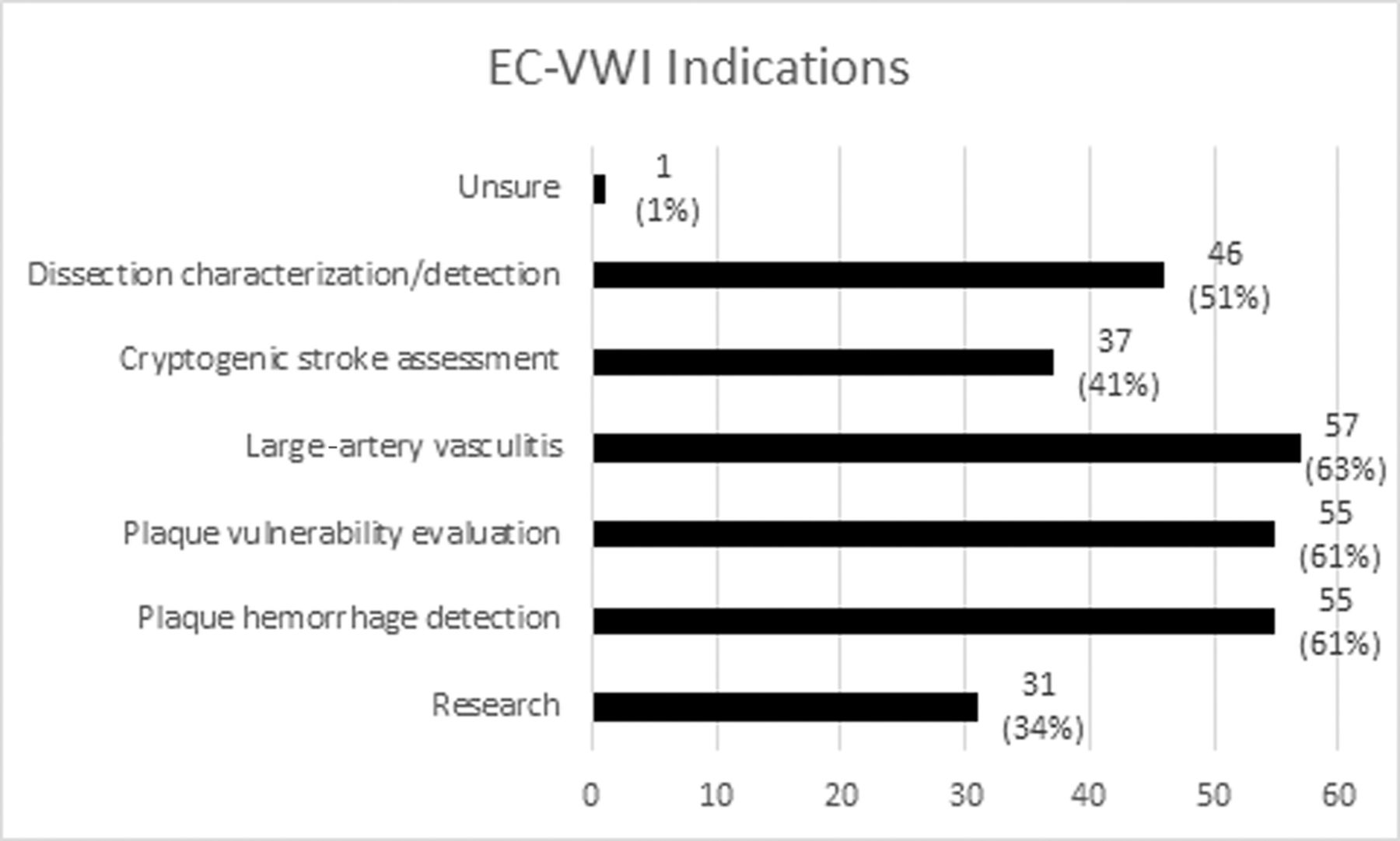
Respondents indicated that EC-VWI was most frequently performed for evaluation of large-artery vasculitis (63.3%, 57/90), atherosclerotic intraplaque hemorrhage assessment (61.1%, 55/90), plaque-vulnerability assessment (61.1%, 55/90), and dissection characterization/detection (51.1%, 46/90) (Fig 3).

Question: For what primary purpose does your institution perform carotid vessel wall imaging (Choose all that apply)? There were 90 respondents with 282 responses.
Of respondents from the United States, 21.7% (68/314) indicated that their institution performed EC-VWI. Among Eastern US respondents, 25% (19/76) indicated that their groups performed EC-VWI, compared with 25% (24/96) of Southern, 23.1% (15/65) of Western, and 13% (10/77) of Midwestern respondents. For those respondents from outside the United States, 50% of South American (8/16), 48.4% (15/31) of European, 43.8% (7/16) of Canadian, and 33.3% of Asian (8/24) and African (1/3) respondents indicated performance of EC-VWI. No Australian (0/4), Mexican (0/1), or Jamaican (0/2) respondents indicated EC-VWI use at their respective institutions.
In terms of practice type, 21.7% (10/46) of respondents from private radiology practices, 36.7% (22/60) of respondents from academic institutions, 50% (2/4) of respondents from federal institutions, and 25% (1/4) from hybrid institutions indicated that they performed EC-VWI. This was from 114 responses for which institutional information was available.
Vendor Environment
One hundred twelve total responses indicated that institutions performed EC-VWI on 3T MR imaging systems, while 50 responses indicated that it was performed on 1.5T systems. EC-VWI was most frequently performed on 3T Siemens MR imaging systems (58%, 53/92), followed by 3T GE Healthcare systems (33%, 30/92) and 3T Philips Healthcare systems (30%, 28/92). Please refer to the Online Supplemental Data for full details. Sixty percent indicated that they performed EC-VWI only on 3T field strength, 34% indicated use of both 3T and 1.5T field strengths, while 5% only used 1.5T.
Forty-six percent indicated that their institution had a research agreement with their MR imaging vendors, 39% indicated they did not, while 16% were unsure. For those with a vendor research agreement, 45% sought vendor support for protocol development, 39% did not, while 16% were unsure. For those that were able to develop a protocol with vendor support, 54% did so with Siemens; 40%, with Philips Healthcare; and 33%, with GE Healthcare (Online Supplemental Data). Thirty-three percent indicated initial difficulties, 30% indicated limited vendor contribution, 26% were still looking for a solution, and 20% had an excellent experience (Online Supplemental Data). For those who responded that they did not seek vendor support for protocol development, 31% indicated limited vendor contribution, while 10% were still looking for a solution. Conversely, for those who indicated limited vendor contribution, 47% did not seek a contribution from the vendor, while 21% did and 32% were unsure.
EC-VWI Protocol
Of respondents, 24.7% indicated that they performed 2D imaging only; 24.7% indicated the use of only 3D imaging, while 50.6% performed a combined 2D and 3D protocol. On the basis of guidance from the literature, expert lectures, and/or the ASNR Vessel Wall Imaging Study Group, 63.1% pursued their imaging approach; 38.1% factored technical limitations of MR imaging equipment into their protocol development; 26.2% considered time constraints; and 3.5% indicated in the free text response that the protocol design was based on personal experience. In addition, 68.6% indicated that the protocol was developed in-house, 33.7% received the protocol from the vendor, 16.3% received their protocol from another institution, and 11.6% were unsure (Online Supplemental Data).
Institutions most frequently used T1-weighted pre- (88.2%) and postcontrast (83.5%), T2-weighted (49.4%), and 3D gradient recalled-echo (including MPRAGE and echo-spoiled gradient echo) (44.7%) sequences. For MRA techniques, TOF-MRA (61.2%) and contrast-enhanced (57.6%) techniques were typically used (Online Supplemental Data).
Obstacles to EC-VWI Use
Three-hundred four respondents (74%) indicated that their institution did not perform EC-VWI. Among those respondents, 63.9% indicated that the reason for not performing EC-VWI was a lack of clinician/ordering-provider interest; 47.5%, due to lack of time/interest by the radiologist to provide input on protocol development; 44.9%, due to limited expertise of interpretation; 43.7%, from limited personal knowledge of applications and value; and 41.4%, due to limited vendor and technical support for protocol development (see Fig 4 for full details). Of the 63.9% not performing EC-VWI, 17.4% did not provide an explanation for Question 31; 21% provided 1 reason; 13.5%, 2 reasons; 15.5%, 3 reasons; 12.8%, 4 reasons; 10.5%, 5 reasons; 5.3%, 6 reasons; and 2% provided 7 and 8 reasons for not performing EC-VWI, respectively. Educational obstacles were given for 72.04% of responses, while 37.5% of responses included technical challenges. Please see the Online Supplemental Data for distribution and patterns of individual responses.

Question: If your institution is not performing carotid vessel wall imaging (respond to this question only if you are not using carotid VWI), what barriers does your institution face for implementation (choose all that apply)? There were 263 respondents with 800 responses.
For those not performing EC-VWI, 51.1% indicated that their institution would perform these scans if technical and expertise obstacles were overcome, 8.3% indicated they would not, and 40.6% were unsure.
Provider Interest in EC-VWI
The ordering providers most frequently approaching radiology departments in regard to EC-VWI were stroke neurology (37.2%), followed by neurosurgery (12.5%) and vascular surgery (11.3%). Of respondents, 46.9% indicated that no clinical services had approached radiology, and 13.1% were unsure (Online Supplemental Data).
EC-VWI Impact on Patient Management
Of respondents, 23.7% indicated that they thought EC-VWI had impacted patient management, 48.6% did not think EC-VWI influenced patient management, and 27.7% were unsure. Of those performing EC-VWI, 8.4% responded that they believed the technique had not impacted patient clinical management, 12.1% were unsure, and 79.5% believed that the technique had an impact on patient management.
DISCUSSION
This detailed survey of EC-VWI use among ASNR members yielded several important findings in regard to performance, indications, and barriers to implementation across many practices. Overall, only about one-quarter of practices offer EC-VWI, and one-third of those perform it on a frequent basis. The utilization rate may even be overinflated compared with general practice, considering a disproportionate response rate from the ASNR VWI Study Group and academic centers. Considering that the most frequent clinical application use indicated by respondents was inflammatory vasculopathy assessment, its adoption for the most studied and most common vascular disease process, carotid plaque risk assessment, is likely even lower than indicated. There was substantial variability of use among different regions of the United States and among countries, ranging from little-to-no reported use to use in about half of practices in some areas such as South American and European institutions. EC-VWI was more commonly performed in academic institutions than in private practices. There were many barriers to implementation: Chiefly, the primary barrier was a lack of clinician interest, but several technical or radiologist-related factors such as lack of interest, time, or expertise were also prevalent. These results reveal opportunities to substantially enhance implementation across practice types and geographic regions and ultimately optimize patient care.
EC-VWI is an established technique technically and scientifically, with substantial imaging-histologic correlation from carotid endarterectomy specimens—that is, important features of carotid plaque including intraplaque hemorrhage, lipid-rich necrotic core, fibrous cap disruption, positive remodeling, and neovascularity can be accurately assessed.3,6 There are data indicating the utility of EC-VWI for atherosclerotic stroke-risk stratification,3,6 identification of the source of cryptogenic stroke,7⇓-9 and prediction of future stroke events,10,11 in addition to assessment of less common entities, including blunt cerebrovascular injury12,13 and inflammatory vasculopathy.14,15
We found that despite these data, widespread adoption is lacking. Identification of the major reasons in the current study may help pinpoint strategies for improved implementation. Several issues of radiologists could be addressed by additional education about the utility of EC-VWI, which could spark interest and increased education related to interpretive skills. Specifically, this education could be accomplished in many forms, including formal Continuing Medical Education courses, practical how-to review articles, and one-on-one peer-to-peer mentorship. ASNR and the ASNR Vessel Wall Imaging Study Group would be well-positioned to take leading roles in this effort. Additional focus on the technical and interpretive aspects in neuroradiology fellowship programs could also assist dissemination across practices.
Although we cannot determine the reasons for lack of interest among some clinicians with certainty, enhanced education of clinicians about the value of EC-VWI through increased presence in clinical journals and national meetings may be beneficial because some clinicians are unaware of, or unconvinced by, the current literature. The perception that EC-VWI does not change management in many patients may partially reflect clinician knowledge and/or philosophy. Randomized controlled surgical trials using EC-VWI for patient selection could provide additional support for the technique.
We found that about half of the practices surveyed that do not currently use EC-VWI would be interested in offering and performing this examination if barriers were reduced, presenting a substantial opportunity that can be accomplished via several methods. In addition to the educational and collaborative opportunities listed above, these include development of easy-to-use and readily accessible EC-VWI protocols by both vendors and radiologists, improved classification schemes, and improved processing. This survey also detailed the typical pulse sequences, field strengths used, and protocolling practices (clinician order versus radiologist add-on), which may be important considerations to facilitate wider adoption. Another potential technical obstacle that was not addressed in this survey is the use of specialized carotid coils for EC-VWI, which many groups may not have or may not be willing to acquire. Development of EC-VWI protocols that can be implemented with standard neurovascular coils would help lower this technical barrier and potentially increase adoption.
Development of commercially available image-processing techniques could also help lower the barrier to EC-VWI adoption. Automated techniques that could align imaging to standard projections,16 segment pathologic lesions, quantify vulnerable features,17 and stratify risk on the basis of these features would ease the interpretation burden on radiologists. In addition, lesion detection and stenosis quantification tools18 could also help augment workflow efficiency. Software tools could also help improve standardized interpretation and reporting approaches, providing improved quality and consistency of reporting and creating better value to ordering clinical services for patient management. These measures could lead to increased adoption, reliance, and acceptance of EC-VWI by radiology departments and ordering providers alike.
A previous multinational survey with 223 multidisciplinary respondents, including radiologists, neurologists, vascular surgeons, and technologists, focused on multitechnique imaging and management of carotid atherosclerotic disease and found that only 8% of respondents indicated that MR imaging was the first-line of imaging for symptomatic carotid atherosclerotic disease, and it was only 4% in asymptomatic carotid atherosclerosis.19 The use of MR imaging in our survey was higher, possibly due to the varied applications targeted beyond carotid atherosclerosis and possibly due to the cohort because our survey included more responses from the United States (76% versus 13%, respectively). The current survey focused more on EC-VWI applications, protocols, field strengths, and barriers to performance, while the previous survey focused more on first-line imaging and treatment.
The current survey has several limitations. First, it was a voluntary survey of a national society with a relatively low response rate, which could contribute to selection bias toward those more motivated to respond to the survey due to interest or performance of EC-VWI. This bias is exemplified by the disproportionate response rate from the ASNR VWI Study Group, who are all ASNR members. Radiologists who are not current members of the ASNR or were not members at the time of survey administration would not have had an opportunity to respond to the survey. There was variability in total responses regionally, especially internationally, also limiting geographic comparisons of responses. These issues would lead to a limited sampling of the total neuroradiologist population. Second, this survey was performed in 2019, presenting the potential for changes in practice; however, EC-VWI is a relatively mature technique, and considering the intervening COVID pandemic, practice patterns and adoption likely have not changed appreciably. Third, the survey was anonymous because we did not request names or institutions of respondents. While we used IP addresses of responses to mitigate redundant institutional responses, this feature was not available for all responses, and it is possible that >1 response could have come from some institutions. Third, the survey asked about only MR imaging techniques; however, CTA and sonography can be used for plaque characterization, vasculitis, and dissection evaluation, each with their specific applications. This survey does not comprehensively assess other imaging modalities for cervical vascular imaging. A previous study, however, indicated that in clinical practice, radiologists rarely report on plaque characteristics on CTA neck studies, only stenosis measurements.20
CONCLUSIONS
EC-VWI is an imaging technique that is used by approximately one-quarter of institutions as indicated by this survey of the ASNR membership, and for those performing the technique, two-thirds used it infrequently. When used, it is performed for a variety of indications. The most frequent reason for institutions not performing this technique was a lack of interest by clinicians, though technical support and radiologist-related reasons were also prevalent. More than half who were not performing EC-VWI indicated that if barriers were overcome, their institution would perform it, and another 40% were unsure. Improved technical support, processing techniques, user-friendly protocols, and education for ordering clinicians and radiologists as well as prospective randomized controlled trials validating the importance of the technique may enhance widespread adoption.
Footnotes
The views expressed in this article are those of the author and do not reflect the official policy of the Department of Army/Navy/Air Force, Department of Defense, or U.S. Government.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
References
- Received June 22, 2022.
- Accepted after revision October 10, 2022.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.