
Abstract
BACKGROUND AND PURPOSE: Intracranial vessel wall MR imaging is an emerging technique for intracranial vasculopathy assessment. Our aim was to investigate intracranial vessel wall MR imaging use by the American Society of Neuroradiology (ASNR) members at their home institutions, including indications and barriers to implementation.
MATERIALS AND METHODS: The ASNR Vessel Wall Imaging Study Group survey on vessel wall MR imaging use, frequency, applications, MR imaging systems and field strength used, protocol development approaches, vendor engagement, reasons for not using vessel wall MR imaging, ordering-provider interest, and impact on clinical care, was distributed to the ASNR membership between April 2 and August 30, 2019.
RESULTS: There were 532 responses; 79 were excluded due to nonresponse and 42 due to redundant institutional responses, leaving 411 responses. Fifty-two percent indicated that their institution performs vessel wall MR imaging, with 71.5% performed at least 1–2 times/month, most frequently on 3T MR imaging, and 87.7% using 3D sequences. Protocols most commonly included were T1-weighted pre- and postcontrast and TOF-MRA; 60.6% had limited contributions from vendors or were still in protocol development. Vasculopathy differentiation (94.4%), cryptogenic stroke (41.3%), aneurysm (38.0%), and atherosclerosis (37.6%) evaluation were the most common indications. For those not performing vessel wall MR imaging, interpretation (53.1%) or technical (46.4%) expertise, knowledge of applications (50.5%), or limitations of clinician (56.7%) or radiologist (49.0%) interest were the most common reasons. If technical/expertise obstacles were overcome, 56.4% of those not performing vessel wall MR imaging indicated that they would perform it. Ordering providers most frequently inquiring about vessel wall MR imaging were from stroke neurology (56.5%) and neurosurgery (25.1%), while 34.3% indicated that no providers had inquired.
CONCLUSIONS: More than 50% of neuroradiology groups use vessel wall MR imaging for intracranial vasculopathy characterization and differentiation, emphasizing the need for additional technical and educational support, especially as clinical vessel wall MR imaging implementation continues to grow.
ABBREVIATIONS:
- ASNR
- American Society of Neuroradiology
- IP
- Internet Protocol
- MR-VWI
- vessel wall MR imaging
Intracranial vessel wall MR imaging (MR-VWI) is capable of detecting,1,2 differentiating,3⇓-5 and characterizing intracranial vasculopathies6⇓-⇓⇓10 and may be able to help predict patient outcomes.11,12 Because this technique has been adopted by a growing number of institutions worldwide, the American Society of Neuroradiology (ASNR) Vessel Wall Imaging Study Group was developed to disseminate vessel wall imaging techniques, educate the general neuroradiology community on its implementation and interpretation, and influence vendors to improve vessel wall imaging techniques.13 Numerous barriers to the implementation of MR-VWI may exist at many institutions, including technology, expertise, knowledge, workflow limitations, and/or vendor relation limitations. The goal of the current survey study was to poll the membership of the ASNR to determine whether institutions were performing MR-VWI, and if not, what barriers exist to its implementation and use. For institutions already performing MR-VWI, our goal was to evaluate applications of the technique, which sequences were being used, how the techniques were developed, levels of clinician interest, and vendor collaborations for technique development. To our knowledge, this is the first study to evaluate institutional use of MR-VWI across a United States–based neuroradiologic society. The survey can help inform the ASNR Vessel Wall Imaging Study Group on the needs of the neuroradiologic community on how to best educate and facilitate the performance of MR-VWI, as well as guide vendors on technical needs for broader MR-VWI use.
MATERIALS AND METHODS
The survey was discussed at ASNR Vessel Wall Imaging Study Group meetings and developed through input by multiple Study Group members. Through an iterative review process, the final survey was developed on the SurveyMonkey.com platform. The survey was built with logic, and if a respondent indicated that they did not perform MR-VWI, he or she skipped to the last 4 questions of the MR-VWI portion of the survey, focused on barriers to MR-VWI performance and ordering-provider interest (the questions in the survey are provided in the Online Supplemental Data). Respondents who indicated that their institution did perform MR-VWI were expected to answer each MR-VWI question of the survey. After institutional review board review, the survey received institutional review board exemption. The anonymous survey was first sent to the ASNR Vessel Wall Imaging Study Group and was opened to the group from March 30 through April 17, 2018. After approval from the ASNR Executive Committee, the survey was then sent to the ASNR membership on April 2, 2019. A second reminder was sent to the membership on August 14, 2019. Responses were gathered between April 2 and August 30, 2019, after which the survey was closed. Individuals could respond to the survey only once.
After collection of survey responses, response quality was assessed, with exclusion of surveys in which the respondent spent <20 seconds on the survey and responded to ≤1 question. Internet Protocol (IP) addresses of the respondents were reviewed to determine the institution of origin for the response. For institutions with multiple responses, partially completed responses were excluded. If there was >1 complete response for an institution, the study investigators reviewed the institutional responses to assess accuracy on the basis of their knowledge of the protocol and clinical performance based on publications, presentations, and/or personal knowledge of the specific institution at the time of the survey. If this issue was not unresolved, discussion with MR-VWI leaders at the particular institution was performed for clarification on their approach at the time. Redundant institutional responses were removed to reduce bias arising from multiple responses from individual institutions that would result in overestimation of the approaches of larger institutions. IP addresses without institutional associations were not excluded. IP addresses were also used to determine the region from which the response came. Responses were grouped into continent, country, and, for US responses, region of the country, divided on the basis of US Census definitions.14 Institutions were categorized as academic, private practice, hybrid, or federal.
RESULTS
Respondents
The survey was distributed to 5552 ASNR members, and 1854 individuals opened the e-mails. There were a total of 46 respondents from the ASNR Vessel Wall Imaging Study Group and 486 respondents from the ASNR membership, for a total of 532 responses. The response rate was 9.6%. Respondents, on average, spent 11 minutes on the survey, and there was an 86% completion rate. We subsequently excluded survey responses for which <20 seconds was spent on the survey and the respondent answered 1 or no questions (n = 79), leaving 453 complete responses. We subsequently excluded redundant institutional responses (n = 42), leading to 411 included responses.
Of the 411 included responses, 81.3% were from North America, 7.5% from Europe, 5.8% from Asia, 3.6% from South America, 1.0% from Australia, and 0.7% from Africa. Among countries, the United States had the most included responses with 314, followed by Canada (n = 16), Brazil (n = 12), and South Korea (n = 5) (see Table 1 for a complete list of country response and included counts). For the 314 US responses, 30.3% were from the South, 24.5% from the Midwest, 24.5% from the East, and 20.7% from the West. Of the 114 responses with institutional IP addresses, 52.6% were academic, 38.6% private practice, 5.3% federal, and 3.5% hybrid institutions.
Countries of origin of total and included respondents
MR-VWI Use
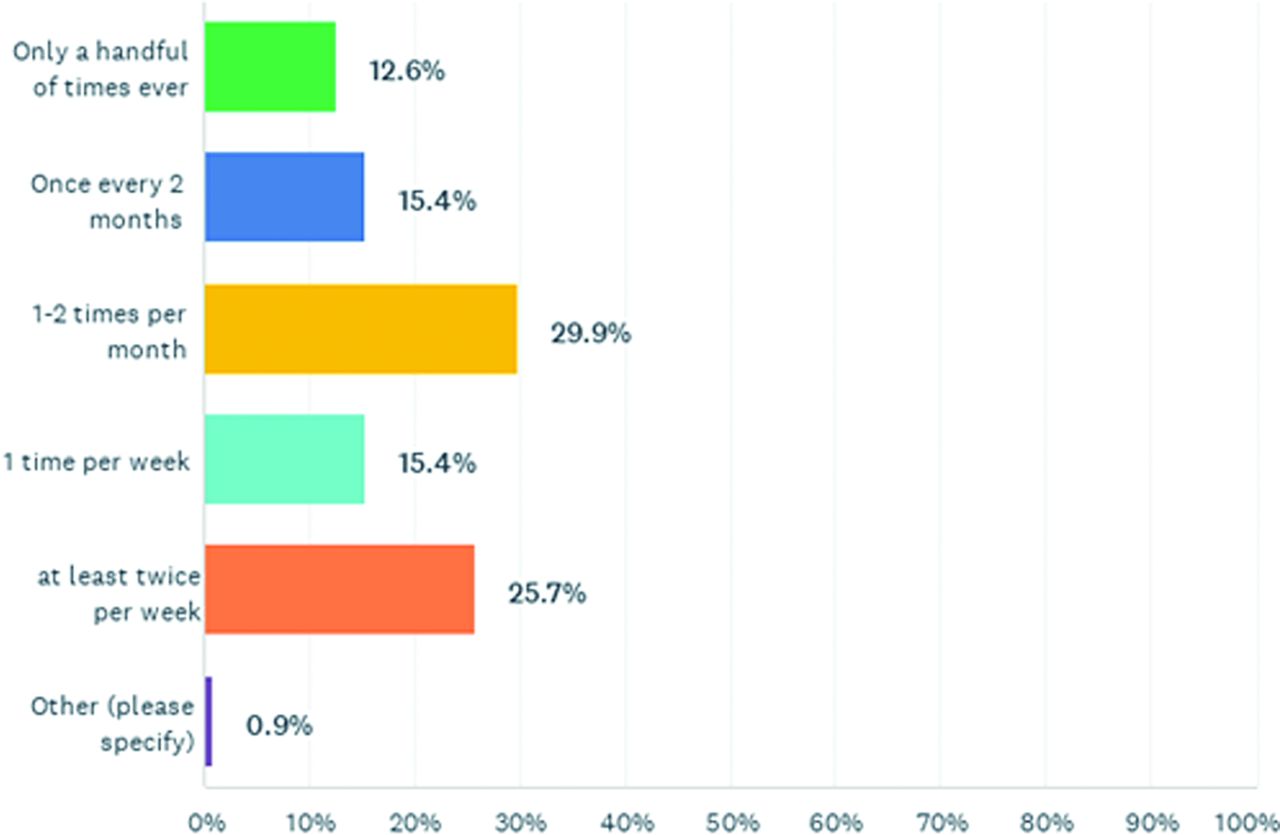
Of included respondents, 52.1% (214/411) indicated that their institution performed MR-VWI. Among those that used MR-VWI, the most common frequency was 1–2 times per month, representing 29.9% (64/214) of respondents, followed by 25.7% (55/214) indicating that they performed MR-VWI at least twice per week, while 15.4% (33/214) indicated that they performed MR-VWI once per week. Overall, 71.5% indicated MR-VWI was performed at least 1–2 times per month (Fig 1).

How often do you perform intracranial vessel wall MR imaging? Respondents = 214.
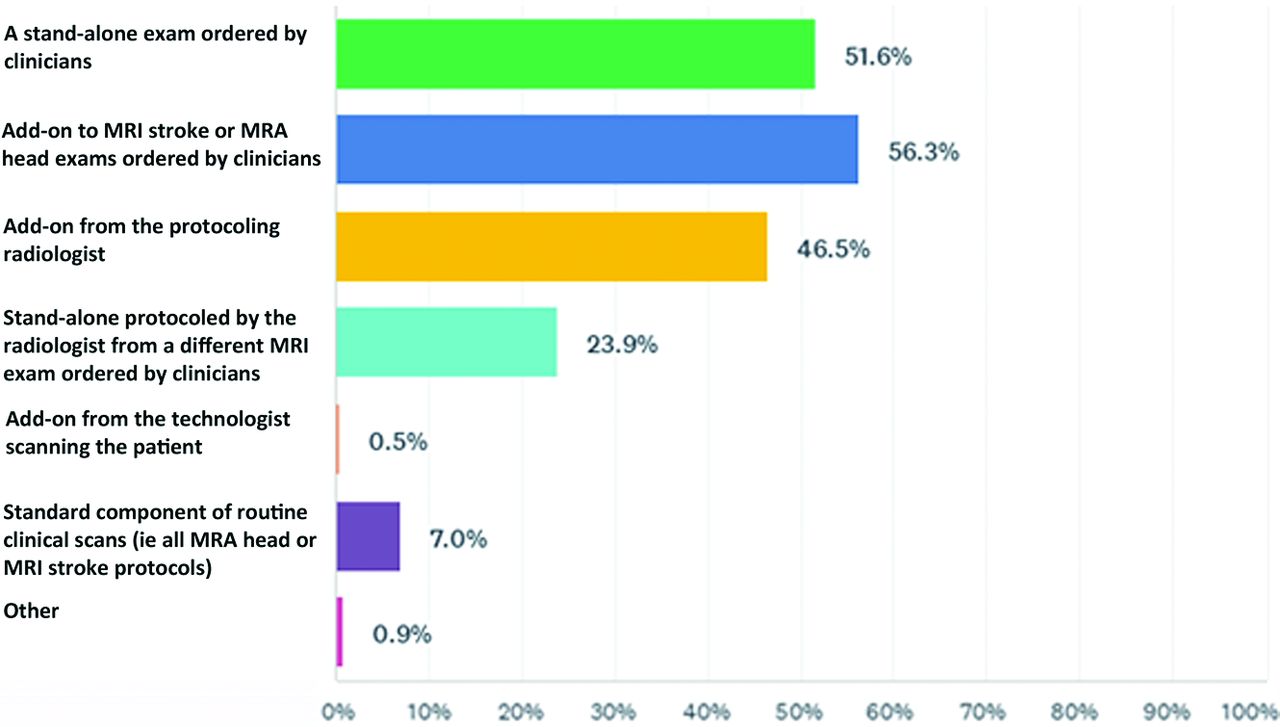
Of respondents, 56.3% (120/213) indicated that MR-VWI was performed as an add-on to the MR imaging stroke protocol ordered by clinicians, 51.6% (110/213) indicated that MR-VWI was performed as a stand-alone examination ordered by clinicians, and 46.5% (99/213) of respondents stated that at their institution, MR-VWI was added on the basis of the protocoling radiologist’s decision. See Fig 2 for full details.

Is intracranial vessel wall MR imaging being clinically performed as? (choose all that apply) Respondents = 213.
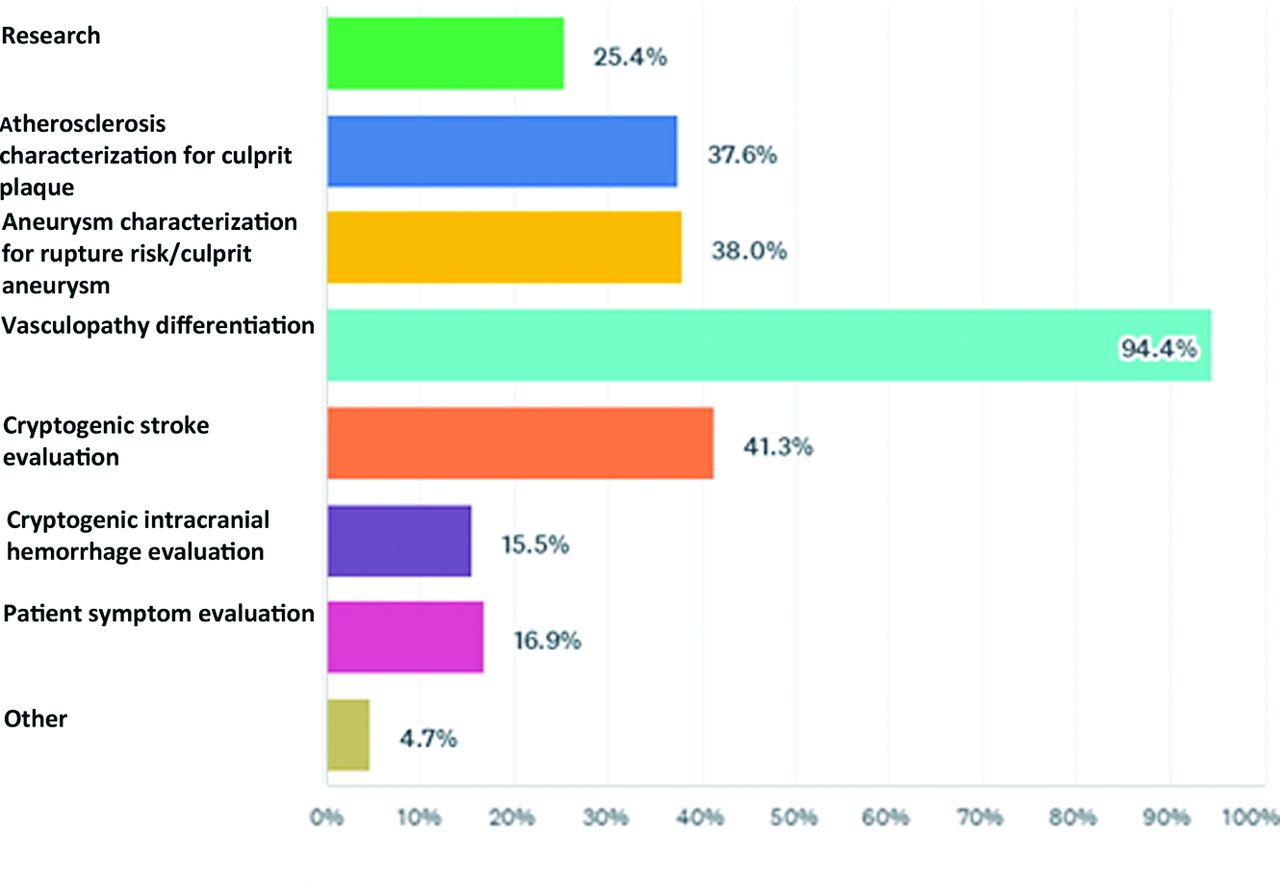
Intracranial vasculopathy differentiation was the most common clinical indication for MR-VWI, indicated by 94.4% (201/213) of respondents. This was followed by cryptogenic stroke evaluation (41.3%; 88/213), aneurysm characterization for rupture risk or culprit aneurysm (38.0%; 81/213), and atherosclerosis characterization for culprit plaque (37.6%; 80/213). Full responses are shown in Fig 3.

For what primary purpose does your institution perform intracranial vessel wall imaging? (choose all that apply) Respondents = 213.
In the United States, 47.3% of respondents indicated that their institution performed MR-VWI. Regionally, Eastern respondents indicated the highest frequency of use (58.4%), followed by the West (55.4%), South (45.8%), and Midwest (31.2%). For respondents outside the United States, 67% indicated that their institution performed MR-VWI. These included 80.6% European, 62.5% Asian and South American, and 66% African; none of the Australian respondents indicated MR-VWI use. In addition, 75% of Canadian and 50% of Jamaican respondents performed MR-VWI.
Among institution types, 61.7% of academic institutions’ responses indicated that they performed MR-VWI, compared with 52.3% of private practice, 66% of federal institutions, and 100% of hybrid practices. These were among 114 responses with institutional IP addresses.
Vendor Involvement
Two hundred fifty-seven total responses indicated that MR-VWI was performed on 3T MR imaging systems, compared with 80 responses indicating use of 1.5T MR imaging systems and 3 indicating the use of 7T systems. MR-VWI was most frequently performed on 3T Siemens MR imaging systems (59.9%; 127/212), followed by 3T GE Healthcare MR imaging systems (34.0%; 72/212) and 3T Philips Healthcare MR imaging systems (26.9%; 57/212). See the Online Supplemental Data for further details. Of responses, 71.2% indicated that they performed MR-VWI on only 3T MR imaging systems; 7.1%, on 1.5T systems only; and 21.7%, on both 3T and 1.5T systems at their respective institutions.
Of respondents, 42.0% indicated that their institution had a research agreement with the vendor, 36.8% indicated they did not, and 21.2% were not sure. For those with a vendor research agreement, 31.9% sought help from the vendor for development of their MR-VWI protocol, and 38.8% did not, while 29.4% were not sure. For those that developed a protocol in collaboration with the vendor that was satisfactory to their clinical needs, 49.2% did so with Siemens; 30.5%, with GE Healthcare; and 28.0%, with Philips Healthcare (Online Supplemental Data). Of respondents, 38.0% indicated limited contributions from the vendors in the development of their clinical protocols, 28.2% indicated initial difficulties when working with the vendor with an eventual solution reached, and 22.5% are still looking for a collaborative solution with their MR imaging vendor; 16.2% indicated an excellent experience working with the vendor on developing an MR-VWI protocol (Online Supplemental Data). In the free-text response, 12 respondents indicated unhappiness with their vendor engagement on protocol development. For those that responded that they did not seek vendor support for protocol building, 40.3% indicated limited vendor contributions, while for those that indicated that they had limited vendor contribution, 48% indicated that they did not seek help from the vendor and 20.4% did, while 31.5% were not sure.
MR-VWI Protocol
Of respondents, 51.2% indicated that they exclusively used 3D MR-VWI protocols and 12.3% used only 2D protocols; 36.5% performed combined 2D/3D protocols; 60.6% pursued their approach to protocols on the basis of published literature, conference lectures, and/or guidance from the ASNR Vessel Wall Imaging Study Group; 29.6% designed their protocols on the basis of the limitations of their MR imaging equipment; 30.5% focused on workflow time constraints to guide protocol approach; 59.2% developed their protocol in-house; 38.9% obtained the protocol from the vendor; and 19.9% received the protocol from another institution (Online Supplemental Data).
Institutions most frequently used postcontrast T1-weighted MR-VWI sequences (89.1%), T1-weighted MR-VWI (88.6%), and T2-weighted (39.3%) sequences, respectively. For MRA techniques, TOF-MRA (76.3%) and contrast-enhanced MRA (36.5%) were used (Online Supplemental data).
Obstacles to Use of MR-VWI
One hundred ninety-seven respondents (47.9%) indicated that their institution was not performing MR-VWI. Of those respondents, 56.7% indicated that the reason was due to lack of ordering-provider interest, while 53.1% indicated that it was due to limited radiologist expertise in interpretation, 50.5% due to limited personal knowledge of applications and value, 49.0% due to lack of radiologists’ time or interest in providing input for protocol development, and 46.4% due to lack of vendor or technical support for protocol development. See Fig 4 for full details.
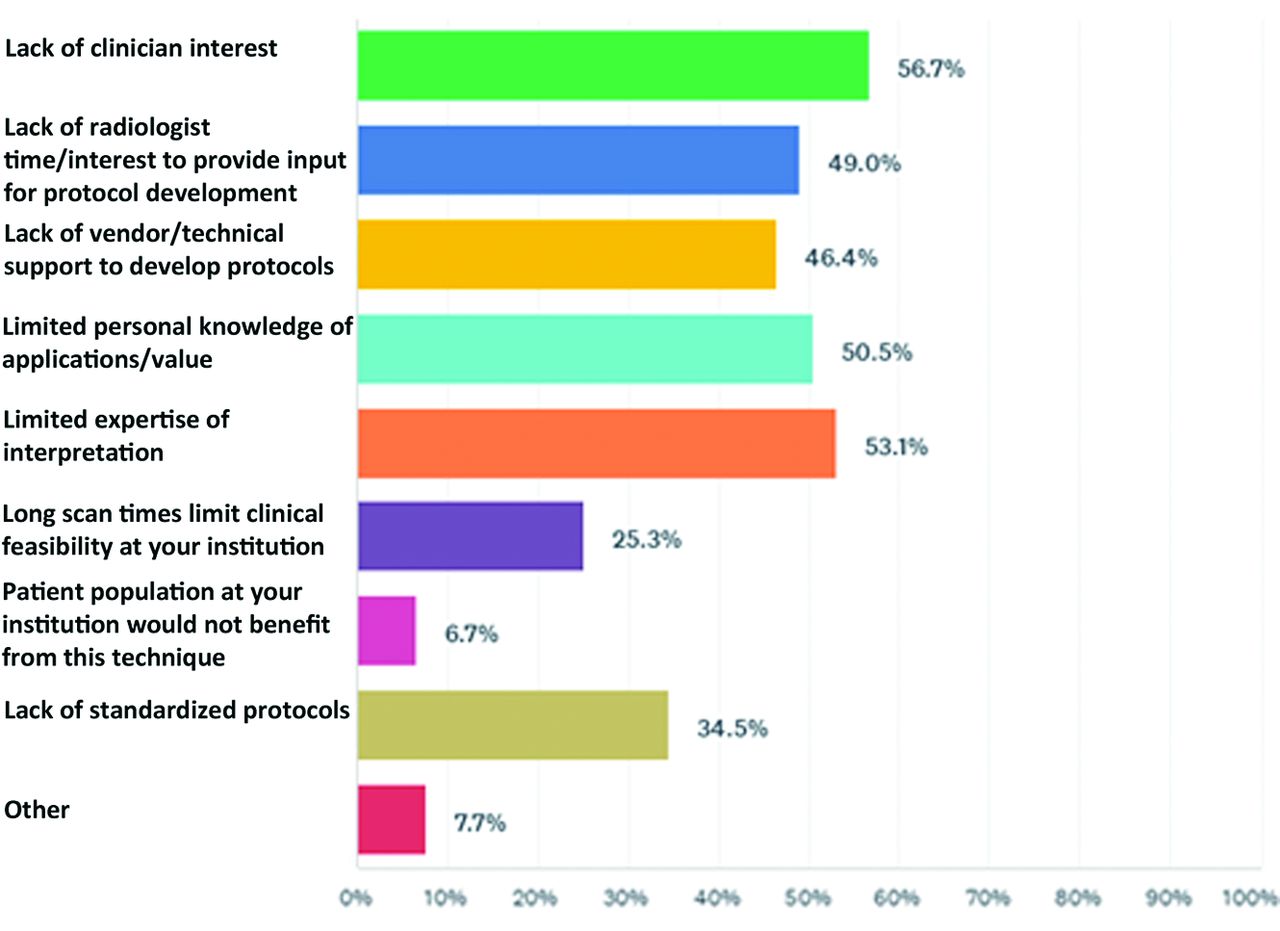
If your institution does not perform intracranial vessel wall MR imaging (only respond to this question if you do not use intracranial vessel wall imaging), what barriers does your institution face for implementation? (choose all that apply) Respondents = 194.
For those facing technical or expertise obstacles for performance of MR-VWI, 56.4% indicated that they would use the technique if these obstacles were overcome; 6.4% indicated that they still would not (Online Supplemental data); and 37.3% were unsure.
Ordering Provider Interest in MR-VWI
Respondents indicated that the following ordering-provider specialties approached radiology departments with interest in MR-VWI performance (respondents could indicate >1 specialty): stroke neurology (56.5%), neurosurgery (25.1%), and rheumatology (14.2%); 34.3% indicated that no ordering providers had expressed interest in MR-VWI (Fig 5).

Have your clinicians approached the radiologists in your group in regard to performing intracranial vessel wall imaging? If so, which clinician groups? (choose all that apply) Respondents = 359.
For respondents indicating that neurology was the only clinical service that ordered examinations, the most common reason was for vasculopathy differentiation (71.1%), followed by cryptogenic stroke (33.0%). For respondents who received requests from neurology and neurosurgery, vasculopathy differentiation remained the most common (83.3%), followed by aneurysm (60.0%) and atherosclerosis (41.7%) characterization for vulnerability. For those who received requests from neurology, neurosurgery, and rheumatology, vasculopathy differentiation was most common (80.8%), followed by aneurysm characterization (57.7%) and cryptogenic stroke (50.0%). See Table 2 for further details.
Institutional indications for MR-VWI performance relative to ordering provider interest
MR-VWI Impact on Patient Management
Of respondents, 40.6% believed that MR-VWI had led to an impact on patient management at their institution, 37.5% believed it had not impacted patient care, and 21.9% were unsure.
DISCUSSION
MR-VWI is a technique that has gained use across >50% of radiology departments that took part in this survey. The technique has shown value in vasculopathy characterization6,7,9,10 and differentiation,3⇓-5 prediction of outcomes,11,12 and association with patient symptoms.6,15 To our knowledge, the current survey study is the first assessing use, approaches, vendor relations, and indications for performance of MR-VWI. Of ASNR member respondents, 52.1% indicated that they were performing MR-VWI for intracranial vasculopathy differentiation, cryptogenic stroke etiology evaluation, and atherosclerosis with aneurysm characterization for vulnerability being the most common indication. Almost 72% of respondents indicated that MR-VWI was performed at their institution at least 1–2 times per month, with 41.1% performing the technique at least once per week. Respondents most frequently indicated a successful interaction with Siemens in protocol development; however, <45% indicated development of a protocol with more than limited contributions from the vendor, and 16% indicated an excellent experience. However, these responses are because almost half of those that indicated limited vendor contribution never sought vendor help for protocol development, indicating the need for increased radiologist-to-vendor outreach and engagement. The most common approach to protocols was the use of 3D sequences, indicated by >87% of respondents with protocols developed in-house. The most common protocol constructions were based on recommendations or approaches outlined by the ASNR Vessel Wall Imaging Study Group, published literature, or lectures at national meetings. The most common barriers to MR-VWI implementation were lack of ordering-provider interest, lack of expertise in interpretation, limited personal knowledge of MR-VWI value or applications, lack of time or interest by the radiologist in providing protocol input, and lack of vendor or technical support for protocol development.
Protocols most commonly included T1-weighted, T1-weighted postcontrast, T2-weighted MR-VWI sequences, and TOF-MRA and contrast-enhanced MRA for luminal imaging, respectively. T1-weighted pre- and postcontrast high-resolution sequences are central to MR-VWI performance because assessment of enhancement contributes to vasculopathy differentiation,3,5 determination of culprit status of atherosclerosis9,16 and aneurysms,15 association with increased aneurysm vulnerability scores,8 symptoms,6 risk of growth,7 associations with recurrent stroke,12,17 association with subsequent vasospasm development,11 and identifying appropriate biopsy targets.18 T2-weighted MR-VWI is less frequently used, likely in many groups, due to time constraints; however, T2-weighted sequences have shown additional value in differentiating vasculopathies.4 While luminal stenosis measurements are more accurate on MR-VWI compared with TOF-MRA,2,19 TOF-MRA is frequently included in MR-VWI protocols because it provides easier identification of stenoses, luminal irregularities, and aneurysms. Contrast-enhanced MRA is also frequently used because it provides more accurate depiction of slow or turbulent flow than TOF-MRA.
The reluctance to implement MR-VWI with little experience or training is well-founded, considering the high frequency of interpretive pitfalls encountered with these examinations.20 A majority of those not performing MR-VWI (56.4%) indicated that if technical or expertise barriers were overcome, their institution would perform MR-VWI. Therefore, both vendor involvement with users and user willingness to reach out to vendors are fundamental to the implementation of MR-VWI in clinical practice. This requirement was highlighted in the survey by most respondents indicating limited or no contribution from the vendors in the development of successful clinical protocols, yet nearly half of the respondents that indicated limited vendor contribution never sought help from their vendors. Increased societal engagement with vendors is also necessary to share expert opinions on technical and clinical approaches and the value and applications of MR-VWI and to help optimize technique development and implementation. In addition, there are various technical parameters to be manipulated in the MR-VWI sequences, including spatial resolution, the timing between injection and postcontrast sequence acquisition, and specific sequence preparation to decrease slow-flow artifacts. The sheer number of options and variables contributes to general uncertainty in how to construct the optimal MR-VWI sequence.
This survey conveys the high level of interest from ordering providers and neuroradiologists in MR-VWI and its potential in the diagnosis and characterization of intracranial vascular diseases. Considering that many respondents indicated a lack of knowledge of MR-VWI applications and imaging interpretation and limited technical expertise, MR-VWI could be even further incorporated into clinical practice with improved education from national and international societies, journals, and study groups. This education can be accomplished through an increased representation of MR-VWI at national and international radiology conferences, through conference sessions on MR-VWI, MR-VWI cases of the day at conferences and on societal webpages, case presentations from experts on social media, peer-reviewed educational publications in radiology and nonradiology clinical journals and webinars, and engagement through institutional multidisciplinary conferences. Through improved knowledge by radiologists of appropriate applications of MR-VWI and correct examination interpretation, ordering providers will better understand the potential diagnostic impact of the technique.
Improved and automated reconstruction, segmentation, quantitation, and disease identification algorithms can also facilitate adoption of MR-VWI. Tools that are agnostic about vendor platforms and techniques could improve generalization and use. Software solutions that make MR-VWI interpretation more standardized, efficient, reproducible, and definitive would facilitate development of standard interpretation approaches and contribute to the development of improved imaging guidelines. These tools could also facilitate the development of automated, quantitative metrics that could help differentiate vasculopathies and stratify patient risk of vasculopathy complications, including stroke and subarachnoid hemorrhage, as well as tracking treatment responses. Because these tools would reduce the burden on radiologists’ expertise and technical homogeneity, neuroradiology and ordering-provider teams would more readily rely on MR-VWI and its output.
Stroke neurologists were the most common ordering provider with interest in MR-VWI. Considering nearly one-third of respondents indicated that no ordering providers had inquired about MR-VWI at their institution, further education of relevant providers on the value of MR-VWI through their societies via educational sessions at annual meetings, webinars, targeted publications, and education through institutional multidisciplinary conferences can even further increase interest in the technique and lead to increased institutional adoption.
The current survey has a number of limitations. First, it was a voluntary survey of a national society with a relatively low response rate; thus, selection bias based on those more motivated to respond to the survey due to interest may be present. In addition, neuroradiologists or radiologists who interpret neuroradiology studies but are not members of ASNR would not have had an opportunity to respond. This process leads to a limited sampling of the total population of neuroradiologists. Second, this survey was performed in 2019, and due to the rapid evolution of MR imaging technology and the relatively quick adoption of MR-VWI, the responses of some respondents may have changed during the past 2 years. Third, the survey was anonymous; thus, we did not request names or institutions of respondents. While we did use IP addresses of respondents to mitigate redundant institutional responses, this was not available for all institutions, so it is still possible that >1 response could have come from some institutions, potentially presenting bias toward larger institutions.
CONCLUSIONS
Intracranial vessel wall MR imaging is a technique that is used by >50% of institutions as indicated by this survey of the American Society of Neuroradiology membership, primarily for intracranial vasculopathy differentiation, cryptogenic stroke, and atherosclerosis and aneurysm risk assessment. Approximately half of respondents reported limited expertise in interpretation, half reported limited knowledge of applications, and half reported technical limitations in protocol development as barriers to implementation. In addition, one-third expressed no provider interest in intracranial vessel wall MR imaging. These survey results highlight the need for further education of neuroradiologists and relevant ordering providers by national and international societies and the ASNR Vessel Wall Imaging Study Group and increased engagement with vendors to overcome technical limitations in protocol implementation, especially as the increasing adoption of vessel wall MR imaging across practices continues.
Footnotes
This work was supported by the US Department of Health and Human Services, the National Institutes of Health, and the National Institute of Neurological Disorders and Stroke, R01NS092207 01A1.
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received February 21, 2022.
- Accepted after revision April 22, 2022.
- © 2022 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Deep Learning-Based Reconstruction of 3D T1 SPACE Vessel Wall Imaging Provides Improved Image Quality with Reduced Scan Times: A Preliminary Study
- Comprehensive imaging analysis of intracranial atherosclerosis
- Implementation of a Clinical Vessel Wall MR Imaging Program at an Academic Medical Center
- Survey of the American Society of Neuroradiology Membership on the Use and Value of Extracranial Carotid Vessel Wall MRI