
Abstract
SUMMARY: Benign enhancing foramen magnum lesions have been previously described as T2-hyperintense small, enhancing lesions located posterior to the intradural vertebral artery. We present the first case with pathologic correlation. These lesions are fibrotic nodules adhering to the spinal accessory nerve. While they can enlarge with time on subsequent examinations, on the basis of the imaging characteristics and location, they do not necessitate surgical resection.
ABBREVIATIONS:
- BEFML
- benign enhancing foramen magnum lesions
- HSL
- high-signal lesions
- SAN
- spinal accessory nerve
The patient was a 45-year-old woman without significant medical history who presented with a 1-year history of bilateral eye pain. The initial MR imaging performed at an outside institution showed 2 small, enhancing intradural extramedullary lesions at the foramen magnum, posterior to the intradural vertebral arteries in the subarachnoid space. The leading differential at that time was peripheral nerve sheath tumor. She presented to our institution for further evaluation of the foramen magnum lesions and underwent a lumbar puncture to evaluate malignancy, which had negative findings. Given the presenting symptoms, she underwent facial electromyography that did not demonstrate findings of denervation. She also underwent a PET/CT, which revealed no abnormal radiotracer uptake in the enhancing foramen magnum lesions or elsewhere in the body. A catheter angiogram did not show vascular enhancement associated with the lesions. She underwent further MR imaging at our institution.
Imaging
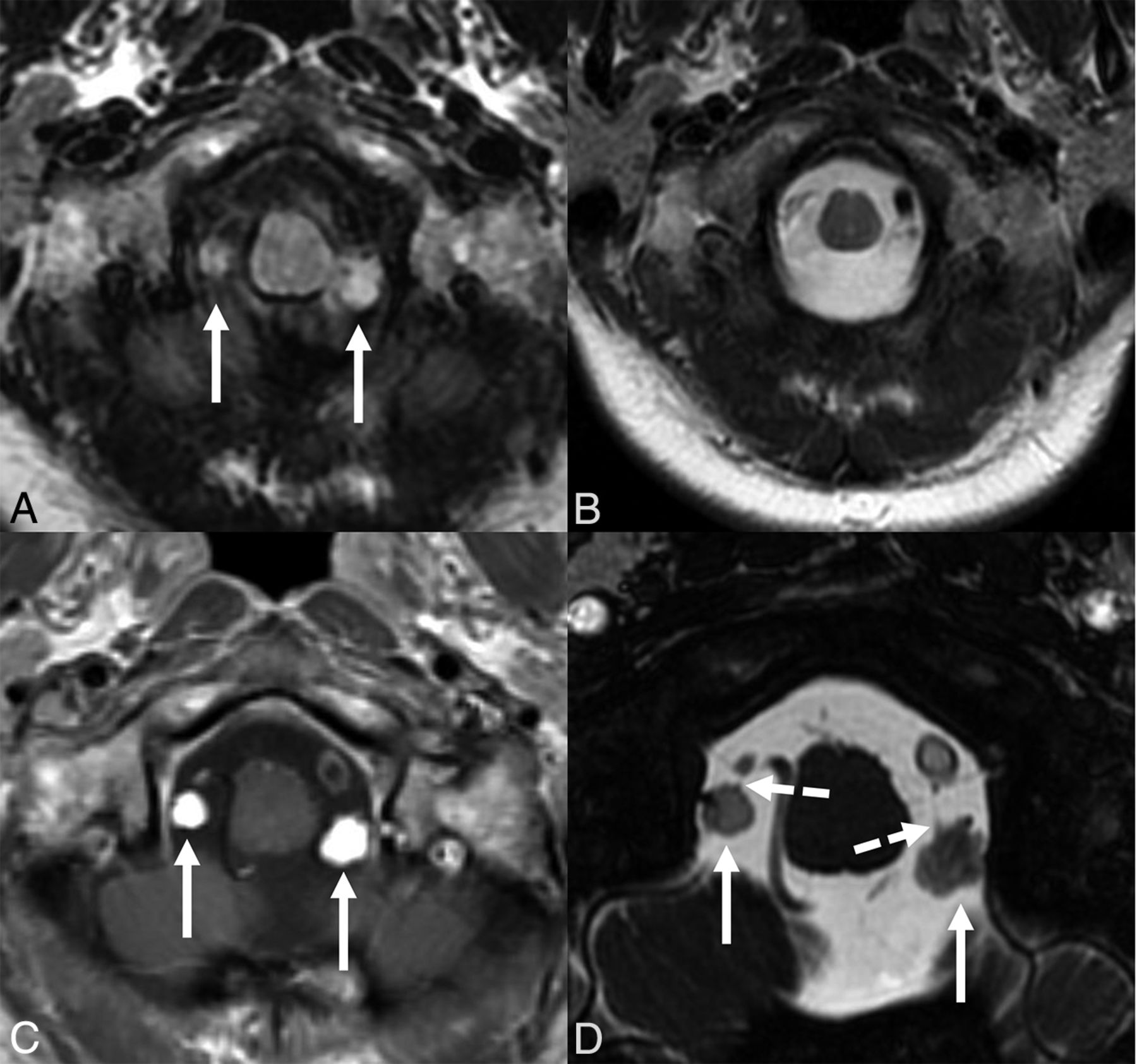
Contrast-enhanced 3T MR imaging of the brain demonstrated 2 small, rounded avidly-enhancing intradural extramedullary lesions at the foramen magnum, posterior to the vertebral arteries, superior to their dural insertion (Fig 1). These lesions were hyperintense on T2-weighted FLAIR imaging, isointense to CSF and, therefore, undetectable on T2-weighted imaging, and did not have restricted diffusion or susceptibility-weighted artifact. Compared with the MR imaging from 9 months prior, they were slightly increased, measuring 8 × 6 × 7 mm on the left (previously 7 × 5 × 6 mm) and 5 × 4 × 5 mm on the right (previously 4 × 3 × 4 mm). Additionally, there was a third lesion just inferior to the right lesion and not within the FOV on the prior study. This lesion had imaging characteristics similar to those of the other lesions, measuring 7 × 6 × 8 mm, and was at the level of the dural puncture of the right vertebral artery. All 3 lesions were adjacent to the spinal accessory nerve (SAN). Contrast-enhanced MR imaging of the remainder of the spine did not show any additional lesions. Given the growth during a short period, the differential diagnosis was broad and included peripheral nerve sheath tumors, metastatic disease, and inflammatory conditions such as a sarcoid. At this time, these lesions had not been previously described in the literature.1

Multiple axial images show 2 intradural extramedullary lesions (solid arrows) at the foramen magnum posterior to the vertebral arteries, superior to their dural insertion. The lesions demonstrate hyperintense signal on T2-weighted FLAIR imaging (A), are isointense to CSF on T2-weighted imaging (B), and are avidly enhancing (C). FIESTA imaging (D) shows contact with the spinal accessory nerve (broken arrows).
Operative Report
Given the differential diagnoses, the patient underwent surgical resection with a midline suboccipital craniectomy and C1 laminectomy. The lesion on the left was near the vertebral artery and its branches but was not attached to them. It was adherent to a lower cranial nerve, identified as the left SAN on intraoperative nerve monitoring. The lesion was covered with a yellow membrane over an apparent cyst with a more solid and firm component deep to that (Fig 2). Intraoperative cranial nerve monitoring indicated changes compatible with nerve irritation; therefore, a small amount of residual lesion densely adherent to the nerve was not resected. The right-sided lesions with mixed cystic and solid components were debulked because they were adherent to lower cranial nerve rootlets, suspected of being the SAN but not confirmed by electromyography. The patient had an uneventful postoperative course without findings of CSF leak or cranial nerve deficit.

Intraoperative photograph demonstrates the lesion with a superficial yellow membrane over an apparent cyst with a more solid and firm component deep to that. The lesion was adherent to a lower cranial nerve, identified as the left SAN on intraoperative nerve monitoring.
Pathology
Pathology received a specimen entirely composed of arachnoid tissue containing a small (11 mm), hypocellular, and densely fibrotic nodule without specific features as illustrated in Fig 3A. The nodule contained scant arachnoid cells separated by thick collagenous fibers (Fig 3B). There were no histologic features to suggest a neoplasm or meningioma. Only focally small nests of meningothelial cap cells with focal psammoma body formation were present in the overlying arachnoid membrane (Fig 3C), a finding commonly present in the arachnoid of adults, which tends to increase with advancing age.

H&E sections of the resected specimen illustrate the densely fibrotic nodule (A), involving the arachnoid (B). Small nests of meningothelial cap cells with focal psammoma body formation are present (C), adjacent to the nodule.
DISCUSSION
This is the first pathology-proved case of benign enhancing foramen magnum lesions (BEFML). We found that these lesions are fibrotic arachnoid nodules adherent to the dorsal aspect of the SAN. It is important to demonstrate that these pathology-proved lesions are benign and do not need surgical resection.
McGuinness et al1 were the first to describe BEFML by their MR imaging appearance. They noted that the enhancing lesions were hyperintense on 3D T2-weighted FLAIR, round or ovoid in morphology, and posterior to the intradural vertebral artery. The lesions were thought to represent a venous varix or a ganglia/pseudoganglia of the C1 nerve or spinal roots of the SAN. The occult appearance on 2D T2-weighted imaging helps differentiate these lesions from the typical appearance of other lesions including meningioma, schwannoma, aneurysm, and metastasis.2 A minority of meningiomas, schwannomas, and metastatic diseases can appear T2 hyperintense but not necessarily occult on T2-weighted imaging. While cystic lesions such as arachnoid, neurenteric, or synovial cysts could be occult on T2, they would not enhance.3 Our patient presented and underwent surgery before the published work by McGuinness et al.
Rosskopf et al4 published a case report on the intraoperative appearance of BEFML without pathologic confirmation and thought that these lesions represented a venous structure. Antonucci et al5 presented a single case of a patient with intracranial melanoma metastases in addition to a small enhancing left foramen magnum lesion that remained stable for 18 months, suggesting a benign process.
The largest study of these foramen magnum lesions was performed by Kogue et al,6 who reviewed 3D T2-weighted FLAIR imaging of 3717 patients and found what they termed high-signal lesions (HSL) posterior to the intradural vertebral artery in 127 patients (3.4%). They noted that all lesions were in contact with the SAN. Their lesions had a mean maximum diameter of 3.8 mm, with an upper range of 11.5 mm. As was the case with our patient, they found that 8.7% of patients had foramen magnum lesions that increased in size with time. On follow-up imaging of our patient 1 year after resection, there were no signs of recurrence or progression. A subsequent study by Kogue et al7 using a 3D balanced fast-field echo sequence found that all lesions contacted the SAN.
The SAN is classically known as providing motor fibers to the sternocleidomastoid and trapezius muscles. However, other studies have suggested that the SAN may transmit sensory/nociceptive signals as well.8,9 Anatomically, the SAN has 2 origins: one that is derived from the upper 5 or 6 cervical spinal cord rootlets and the other arising from the brainstem. Some propose that the SAN starts with mixed motor and sensory components; however, the sensory neurons migrate to the spinal nerve. This process is often incomplete; therefore, neuron cell bodies can be found scattered throughout the nerve.10
Fahmy11 suggested that ganglion cells along the SAN migrate distally with age, given the greater abundance and conspicuity of ganglion cells in a 3-month-old child compared with an adult and greater in the distal SAN relative to proximal. In a postmortem study, Tubbs et al12 found that 14.8% of the specimens had focal enlargements contacting the dorsal aspect of the SAN at the foramen magnum. These enlargements were described as ectopic glial rests or heterotopias within the leptomeninges of the SAN and did not contain ganglion or neuronal cells.
Further work is needed to elucidate the true process that leads to these benign nodules associated with the SAN. Radiologists should be familiar with the typical appearance and benign nature of these lesions so that other entities do not have to be invoked in a differential diagnosis. This is the first work to show pathologic confirmation of what has been previously termed BEFML or HSL.
Case Summary
T2-hyperintense, enhancing, small lesions located posterior to the intradural vertebral artery at the foramen magnum have been previously described as BEFML or HSL.
Previous work has shown that a small percentage (8.7%) of these lesions increase in size.
These were previously presumed to be a venous varix or associated with the SAN.
This is the first pathology-proven case compatible with a fibrotic arachnoid nodule adherent to the leptomeninges of the SAN. While they can enlarge with time, they are benign and do not require treatment.
Footnotes
Disclosure forms provided by the authors are available with the full text and PDF of this article at www.ajnr.org.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received May 21, 2023.
- Accepted after revision June 27, 2023.
- © 2023 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.