
Abstract
BACKGROUND AND PURPOSE: Recent work has shown that fluid-attenuated inversion recovery (FLAIR) imaging with contrast enhancement is highly sensitive for detecting subarachnoid space disease. We hypothesized that contrast-enhanced FLAIR imaging has superior sensitivity to contrast-enhanced T1-weighted MR imaging in detecting leptomeningeal metastases.
METHODS: Sixty-eight patients referred for suspected leptomeningeal metastases underwent 74 MR imaging studies. The patients had either temporally related cytologic proof of leptomeningeal metastases or negative results of clinical follow-up confirming absence of leptomeningeal metastases. The MR imaging examinations included unenhanced and contrast-enhanced FLAIR images and contrast-enhanced T1-weighted MR images that were independently reviewed by two neuroradiologists blinded to the results of cytology. Each of the three sequences was reviewed individually and separately and was assigned a score of positive or negative for leptomeningeal metastases. Discrepancies were settled by consensus.
RESULTS: Of the 17 studies of patients with cytology-proven leptomeningeal metastases, two were positive based on unenhanced FLAIR images, seven were positive based on contrast-enhanced FLAIR images, and 10 were positive based on contrast-enhanced T1-weighted MR images. Of the 57 studies of patients without leptomeningeal metastases, 53 were negative based on unenhanced FLAIR images, 50 were negative based on contrast-enhanced FLAIR images, and 53 were negative based on contrast-enhanced T1-weighted MR images. The sensitivity and specificity of unenhanced FLAIR images for detecting leptomeningeal metastases were 12% (two of 17) and 93% (53 of 57), respectively. The sensitivity and specificity for contrast-enhanced FLAIR images for detecting leptomeningeal metastases were 41% (seven of 17) and 88% (50 of 57), respectively. The sensitivity and specificity of contrast-enhanced T1-weighted MR images for detecting leptomeningeal metastases were 59% (10 of 17) and 93% (53 of 57), respectively.
CONCLUSION: Contrast-enhanced fast FLAIR sequences are less sensitive than standard contrast-enhanced T1-weighted MR sequences in detecting intracranial neoplastic leptomeningeal disease.
Imaging of the diseases of the leptomeninges has evolved. Contrast-enhanced T1-weighted MR imaging represented an advance over CT in depicting leptomeningeal diseases (1, 2). Fluid-attenuated inversion recovery (FLAIR) imaging has been known to be sensitive for parenchymal lesions (3–6). However, FLAIR images have also shown sensitivity for leptomeningeal processes (7, 8). The exact role of contrast-enhanced T1-weighted MR imaging versus FLAIR imaging in assessing the leptomeninges/subarachnoid space has not yet been determined.
In the specific setting of leptomeningeal metastases, contrast-enhanced T1-weighted MR imaging has been shown to have superior sensitivity to that of unenhanced FLAIR imaging (9). Recent work, however, has shown that contrast-enhanced FLAIR imaging is highly sensitive for detecting subarachnoid space disease (10). We hypothesized that contrast-enhanced FLAIR imaging has superior sensitivity to contrast-enhanced T1-weighted MR imaging in detecting leptomeningeal metastases. Our study compared unenhanced FLAIR images, contrast-enhanced FLAIR images, and contrast-enhanced T1-weighted MR images in detecting leptomeningeal metastases.
Methods
From April 2000 to December 2000, we routinely obtained a contrast-enhanced FLAIR sequence of any patient referred for imaging of the brain with clinical suspicion of leptomeningeal metastases. All MR imaging studies of the brain included unenhanced FLAIR imaging and contrast-enhanced T1-weighted MR imaging. A total of 88 studies were conducted. Two of the MR imaging studies of the brain could not be evaluated because of motion artifact. Seventy-four of the cases could be classified as either positive or negative for leptomeningeal metastases based on cytologic and clinical criteria.
In reviewing the clinical records, we considered leptomeningeal metastases to be present if positive results of CSF cytologic examination were obtained either 14 days before or 14 days after MR imaging of the brain. We considered leptomeningeal metastases to be absent if there was no clinical evidence of leptomeningeal disease with follow-up of ≥2 months and no positive cytology. The clinical criteria called for no new or progressive neurologic deficits for ≥2 months after MR imaging. Negative CSF cytology is not adequate because even three separate lumbar punctures can have a false negative rate of ≤10% (11). Additionally, none of these patients was being treated for leptomeningeal metastatic disease.
The 74 studies were of 68 patients (six patients each underwent imaging twice). The mean patient age was 42 years (age range, 6–78 years; 38 female and 30 male patients). The diagnoses were leukemia (16 patients), lymphoma (15 patients), breast carcinoma (11 patients), melanoma (six patients), lung carcinoma (four patients), sarcoma (three patients), ependymoma (two patients), primitive neuroectodermal tumor (two patients), glioblastoma (two patients), adenocarcinoma (one patient), neuroendocrine carcinoma (one patient), esophageal carcinoma (one patient), laryngeal carcinoma (one patient), germinoma (one patient), cervix carcinoma (one patient), and choriocarcinoma (one patient).
MR imaging examinations were performed on 1.5-T systems. The FLAIR sequences were obtained in the axial plane with flow compensation and were fast FLAIR sequences: inversion time, 2200 ms; 10,000/147 [TR/effective TE]; echo train length, 22; bandwidth, 16 kHz; matrix, 256 × 160. Axial view FLAIR images and axial view T1-weighted MR images were obtained after the IV administration of contrast material at a dose of 0.2 cc per kg of body weight. T1-weighted MR images were not obtained with flow compensation: 600/8 (TR/TE); bandwidth, 16 kHz; matrix, 256 × 192. In both sequences, the field of view was 20 cm, with a section thickness of 5 mm and an intersection gap of 1.5 mm. In 44 studies, the contrast-enhanced T1-weighted MR images were obtained before the contrast-enhanced FLAIR images, and in 30 studies, the contrast-enhanced FLAIR images were obtained before the contrast-enhanced T1-weighted MR images.
The unenhanced axial view FLAIR images, contrast-enhanced axial view FLAIR images, and contrast-enhanced axial view T1-weighted MR images were separated from each other. Each sequence was reviewed separately by two senior neuroradiologists (L.E.G., S.K.S.) who were blinded to patient identity and clinical outcome. The two reviewers independently rated each sequence as positive or negative for leptomeningeal metastases. A positive rating was assigned when abnormal signal intensity or enhancement was present in the cisterns (including cranial nerves), sulci, or along any pial surface. Any discrepancies between the two reviewers were resolved by consensus.
Results
Of the 17 cases in which cytology was positive, unenhanced FLAIR images were positive in two cases, contrast-enhanced FLAIR images were positive in seven, and contrast-enhanced T1-weighted MR images were positive in 10. In the setting of proven leptomeningeal metastases, unenhanced FLAIR images had a sensitivity of 12% (two of 17), contrast-enhanced FLAIR images had a sensitivity of 41% (seven of 17), and contrast-enhanced T1-weighted MR images had a sensitivity of 59% (10 of 17). Combining all three imaging sequences, MR imaging had an overall sensitivity of 65% (11 of 17) (Table 1).
Results of MR readings for leptomeningeal metastases in positive CSF cases
Of the 57 cases in which leptomeningeal metastatic disease was not present, unenhanced FLAIR images were negative in 53 cases, contrast-enhanced FLAIR images were negative in 50, and contrast-enhanced T1-weighted MR images were negative in 53. The specificity of unenhanced FLAIR images was 93% (53 of 57), the specificity of contrast-enhanced FLAIR images was 88% (50 of 57), and the specificity of contrast-enhanced T1-weighted MR images was 93% (53 of 57). In reviewing the false positive cases, with one exception, these patients had histories of treated leptomeningeal metastases. One patient had viral encephalitis clinically. There were four false positive readings among the unenhanced FLAIR images, seven false positives among the contrast-enhanced FLAIR images, and four false positives among the contrast-enhanced T1-weighted MR images (Table 2).
Results of MR readings for negative leptomeningeal metastases cases
A review of the cases with proven leptomeningeal metastases showed one study in which contrast-enhanced T1-weighted MR images were falsely negative whereas both FLAIR sequences were positive (Fig 1). No supplemental oxygen was administered to the patient during this study (12). There were four studies in which both FLAIR sequences were falsely negative whereas the contrast-enhanced T1-weighted MR images were positive. Close evaluation of these FLAIR images did not reveal any pulsation artifact near the findings located by the contrast-enhanced T1-weighted MR images. The location of the lesions included the surfaces of the midbrain (Fig 2), the cerebellum (Fig 3), and within the sylvian fissure. In addition, the timing of the contrast-enhanced T1-weighted MR and FLAIR sequences was not fixed; in two of the four studies, the FLAIR images were obtained after the T1-weighted MR images.

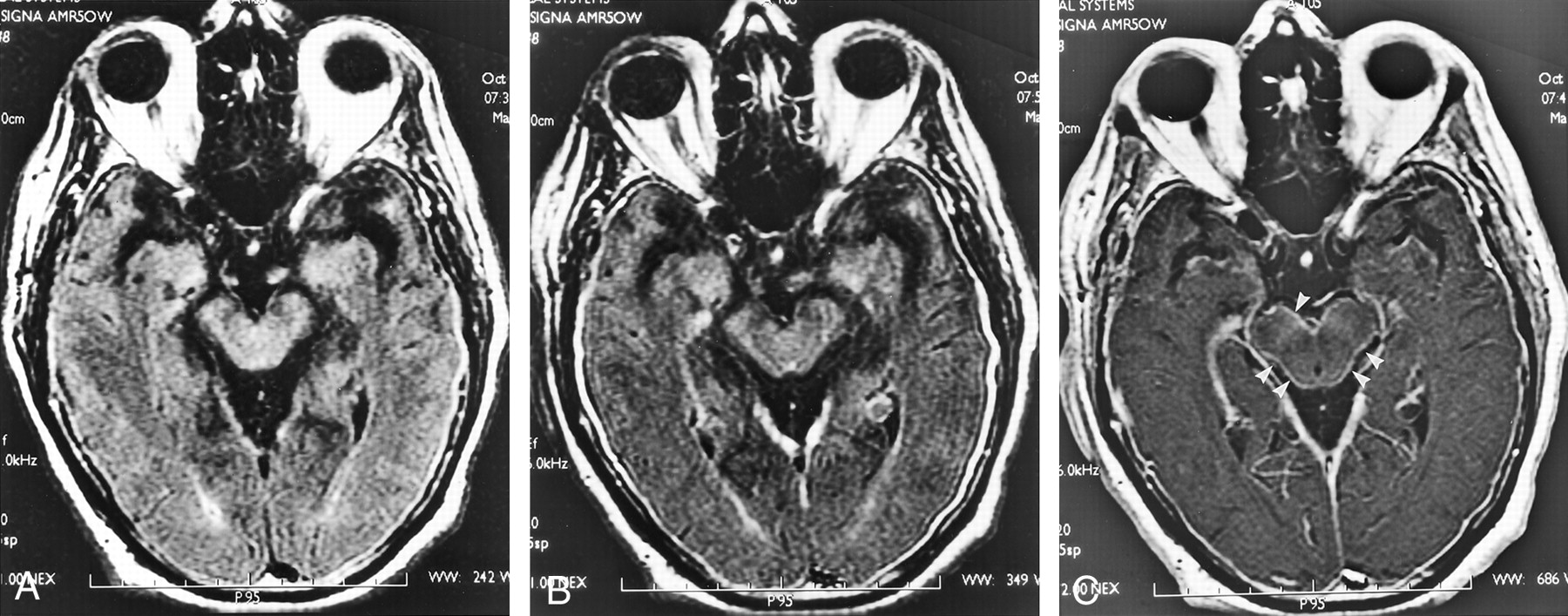
Axial view MR images of a 41-year-old male patient with leptomeningeal metastases from laryngeal squamous cell carcinoma.
A, Unenhanced FLAIR image (10,000/147; inversion time, 2200 ms) shows diffuse abnormal signal intensity in the subarachnoid space (arrowhead).
B, Contrast-enhanced FLAIR image (10,000/147; inversion time, 2200 ms) shows diffuse abnormal signal intensity in the subarachnoid space (arrowheads).
C, Contrast-enhanced T1-weighted MR image (600/8) is falsely negative. Parenchymal metastasis is also identified (arrow).
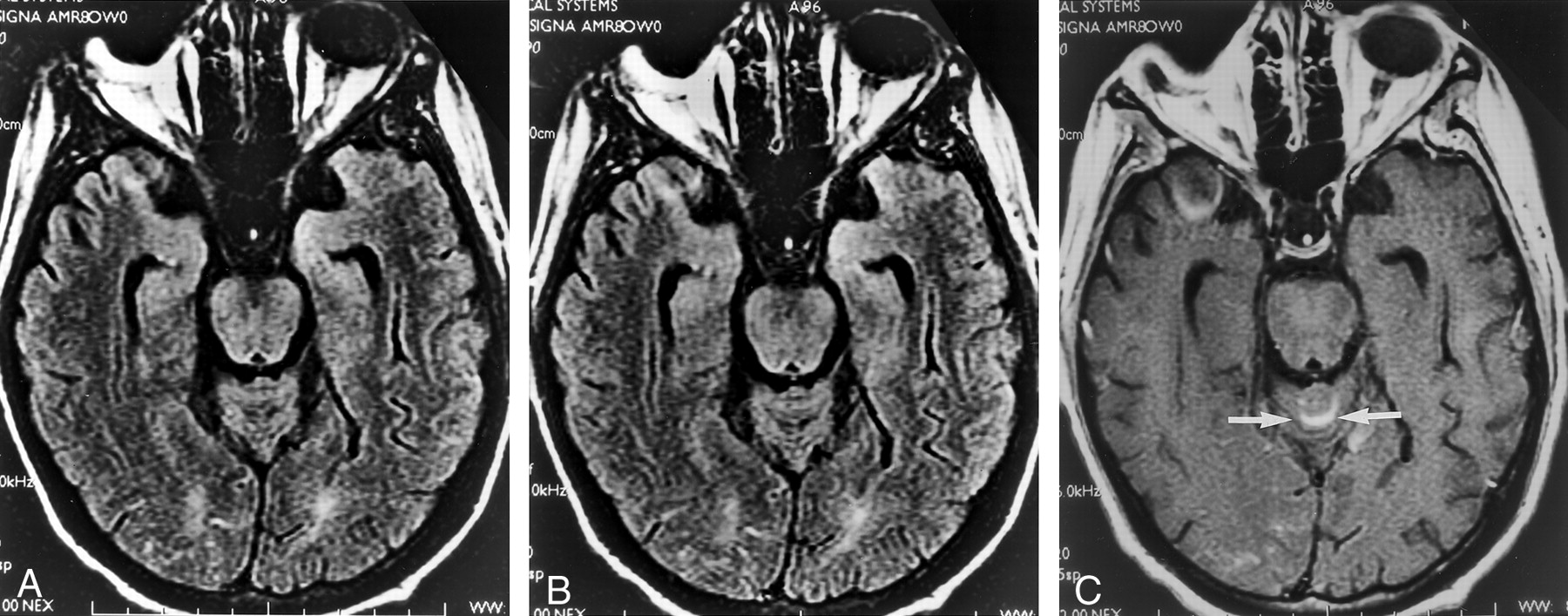
Axial view MR images of a 59-year-old male patient with leptomeningeal metastases from ependymoma.
A, Unenhanced FLAIR image (10,000/147; inversion time, 2200 ms) appears unremarkable.
B, Contrast-enhanced FLAIR image (10,000/147; inversion time, 2200 ms) appears unremarkable.
C, Contrast-enhanced T1-weighted MR image (600/8) shows enhancement along the surface of the midbrain (arrowheads). Thickened, enhancing dura is also identified on the contrast-enhanced images.
Axial view MR images of a 26-year-old male patient with leptomeningeal metastases from leukemia.
A, Unenhanced FLAIR image (10,000/147; inversion time, 2200 ms) is negative.
B, Contrast-enhanced FLAIR image (10,000/147; inversion time, 2200 ms) is negative.
C, Contrast-enhanced T1-weighted MR image (600/8) shows enhancement along the superior surface of the cerebellum (arrows). Artifact is noted in the right temporal and occipital lobes.
To assess interobserver reliability, discrepancies between the two reviewing neuroradiologists were calculated for each sequence. Four discrepancies occurred regarding the unenhanced FLAIR images, seven discrepancies regarding the contrast-enhanced FLAIR images, and four discrepancies regarding the contrast-enhanced T1-weighted MR images. The respective interobserver reliabilities of unenhanced FLAIR images, contrast-enhanced FLAIR images, and contrast-enhanced T1-weighted MR images were 93% (53 of 57), 88% (50 of 57), and 93% (53 of 57), respectively.
Discussion
Leptomeningeal metastatic disease is an important diagnosis to make. Untreated malignant leptomeningeal metastases decreases survival time to <3 months (11, 13, 14). Specific therapy for leptomeningeal metastases must be initiated to slow the progression of the disease (11). Imaging plays a key role in the diagnosis and management of leptomeningeal metastases because it often provides the first clue to the presence of the disease. In addition, CSF cytology is often falsely negative. T1-weighted MR images with paramagnetic contrast have long been the technique of choice for assessing leptomeningeal disease (1, 2), and the reported sensitivity has been as high as 71% (1).
FLAIR images are sensitive for detecting subarachnoid or leptomeningeal lesions, including hemorrhage, inflammation, and neoplasm (7, 8). More recently, because of the contribution of T1 shortening to FLAIR images, contrast-enhanced FLAIR images have been used to assess intra-axial (15–18) and extra-axial lesions (10). Specifically, contrast-enhanced fast FLAIR imaging is sensitive for the evaluation of inflammatory leptomeningeal lesions (10). The reasons for this sensitivity of contrast-enhanced FLAIR imaging include the suppression of adjacent CSF, typical lack of enhancement of normal cortical vessels (as compared with contrast-enhanced T1-weighted MR images), and magnetization transfer saturation effects in fast FLAIR sequences (10). Just as magnetization transfer saturation effects improve visualization of lesion enhancement on fast T1-weighted MR images (19), a similar benefit would be expected with fast FLAIR sequences (20). Because of the enhancement of leptomeningeal lesions on contrast-enhanced FLAIR images, it would seem that contrast-enhanced FLAIR imaging would surpass contrast-enhanced T1-weighted MR imaging in diagnosing leptomeningeal metastases.
Our data showed that contrast-enhanced T1-weighted MR imaging remains the most sensitive single sequence for depicting leptomeningeal metastases. Moreover, the combination of unenhanced FLAIR and contrast-enhanced T1-weighted MR imaging did not yield any false negative cases that were detected only by contrast-enhanced FLAIR imaging. Combining all sequences, MR imaging had an overall sensitivity of 65% (11 of 17) in detecting leptomeningeal metastases. Additionally, contrast-enhanced FLAIR imaging is slightly less specific (88%) than either unenhanced FLAIR or contrast-enhanced T1-weighted MR imaging (93%) in the setting of treated leptomeningeal metastases.
Our data are limited in three respects. First, the minimum follow-up for “negative” leptomeningeal metastases was 2 months. It is possible that leptomeningeal metastatic disease state was present at the time of MR imaging but not evident by the time of clinical follow-up until >2 months. Second, the number of proven positive cases was only 17, making the sensitivity data less robust than the specificity data. Third, the specificity of FLAIR imaging may be higher than we have stated because we do not know whether oxygen was administered in the cases of false positive FLAIR images.
Despite these limitations, the addition of contrast-enhanced FLAIR imaging was not as beneficial in diagnosing leptomeningeal metastases as hypothesized. The reason for this relative lack of sensitivity in comparison with contrast-enhanced T1-weighted MR imaging is not clear. One possibility is that our standard contrast-enhanced T1-weighted MR imaging was better at detecting leptomeningeal lesions than imaging used in previous studies using magnetization transfer saturation with the T1-weighted MR imaging (10). More cortical vessels are seen when magnetization transfer saturation is used with contrast-enhanced T1-weighted MR imaging (21). Leptomeningeal lesions may be less conspicuous as a result.
FLAIR images have their own limitations. Previous work suggests that because many leptomeningeal metastatic lesions involve cranial nerves, CSF pulsation artifact on FLAIR images masks the lesions detected by contrast-enhanced T1-weighted MR imaging (9). In our cases, there was no artifact on the FLAIR images in the subarachnoid space where the lesions were detected only by contrast-enhanced T1-weighted MR imaging. Additionally, none of these findings involved cranial nerves. Another consideration is that FLAIR imaging is less sensitive to the T1 shortening effects of contrast material at higher concentrations (10). This has been shown in a phantom, but it is not clear when such an effect is expected in vivo (10). For our MR imaging, we used the standard dose of contrast material for imaging of the brain; in no case was a higher dose or extra contrast material administered. The concentration of contrast material within a lesion at a certain time also depends on blood flow, capillary permeability, and timing of imaging with respect to the IV administration of the contrast material. In our studies, the contrast-enhanced FLAIR sequence was randomly obtained either before or after the contrast-enhanced T1-weighted MR sequence. There is not enough data from which to draw any conclusions regarding the differences in conspicuity on MR images between different histologic types of leptomeningeal metastatic lesions.
Conclusion
In summary, contrast-enhanced fast FLAIR imaging is less sensitive than standard contrast-enhanced T1-weighted MR imaging in detecting intracranial neoplastic leptomeningeal disease.
Footnotes
This work was presented at the 39th Annual Meeting of the American Society of Neuroradiology, Boston, April 23–27, 2001.
References
- Received October 2, 2001.
- Accepted after revision January 2, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Autocrine CXCL1-CXCR2 Signaling Mediates Leptomeningeal Resistance to Radiation Therapy
- Palliative approach to leptomeningeal carcinomatosis in oesophagogastric junction cancer
- Application of 3D Fast Spin-Echo T1 Black-Blood Imaging in the Diagnosis and Prognostic Prediction of Patients with Leptomeningeal Carcinomatosis
- Headache in a young woman: leptomeningeal metastasis as the first presentation of underlying breast malignancy
- Development of a Standardized MRI Scoring Tool for CNS Demyelination in Children
- Isolated Acute Nontraumatic Cortical Subarachnoid Hemorrhage
- Comparison of the Added Value of Contrast-Enhanced 3D Fluid-Attenuated Inversion Recovery and Magnetization-Prepared Rapid Acquisition of Gradient Echo Sequences in Relation to Conventional Postcontrast T1-Weighted Images for the Evaluation of Leptomeningeal Diseases at 3T