
Abstract
Summary: Neuroradiologists generally do not fully appreciate the importance of the territory of the ascending pharyngeal artery. The ascending pharyngeal artery is a small but important artery that supplies multiple cranial nerves and anastomotic channels to the anterior and posterior cerebral circulations. Several disease processes in the head and neck involve the ascending pharyngeal artery. To evaluate and treat such diseases, it is necessary for neuroradiologists not only to know selective angiography and embolization techniques, but also the territory of the ascending pharyngeal artery, anastomoses, and vascular supply to the vasa nervorum of lower cranial nerves. Herein, the normal angiographic anatomy of the ascending pharyngeal artery, its relationship with neighboring territories, its importance in clinical situations, and research models are reviewed.
The ascending pharyngeal artery is a small vessel. Of the 13 territories, or angiosomes, in the head and neck region, the ascending pharyngeal artery is one of three without cutaneous involvement. Selective angiography and embolization provide increasingly ready access to the ascending pharyngeal artery; however, neuroradiologists generally do not fully appreciate the clinical importance of its territory.
Normal angiographic anatomy of the ascending pharyngeal artery is reviewed. Three-dimensional renditions of the artery’s angiosome are superimposed over arterial anatomy to elucidate crucial arterial anastomoses and the supply to vasa nervorum of lower cranial nerves. The relationship of the vessel’s angiosome to neighboring territories is presented, along with potential communications with the internal and external carotid and vertebrobasilar systems.
The ascending pharyngeal artery has importance in multiple clinical situations in which interventional neuroradiology management plays a central role. Among these are trauma, epistaxis, high-grade head and neck tumors, vascular lesions, skull base tumors, subarachnoid hemorrhage, and agenetic or occluded internal carotid artery. In addition, the ascending pharyngeal artery supplies the swine “rete mirabile,” a reliable animal model for arteriovenous malformations.
Three-dimensional representation of the territory of the ascending pharyngeal artery and major anastomoses elucidate the importance of this vessel. The ascending pharyngeal artery, although small, includes several important deep-tissue extra- and intracranial structures involved in a variety of disease processes.
Anatomy
Origin
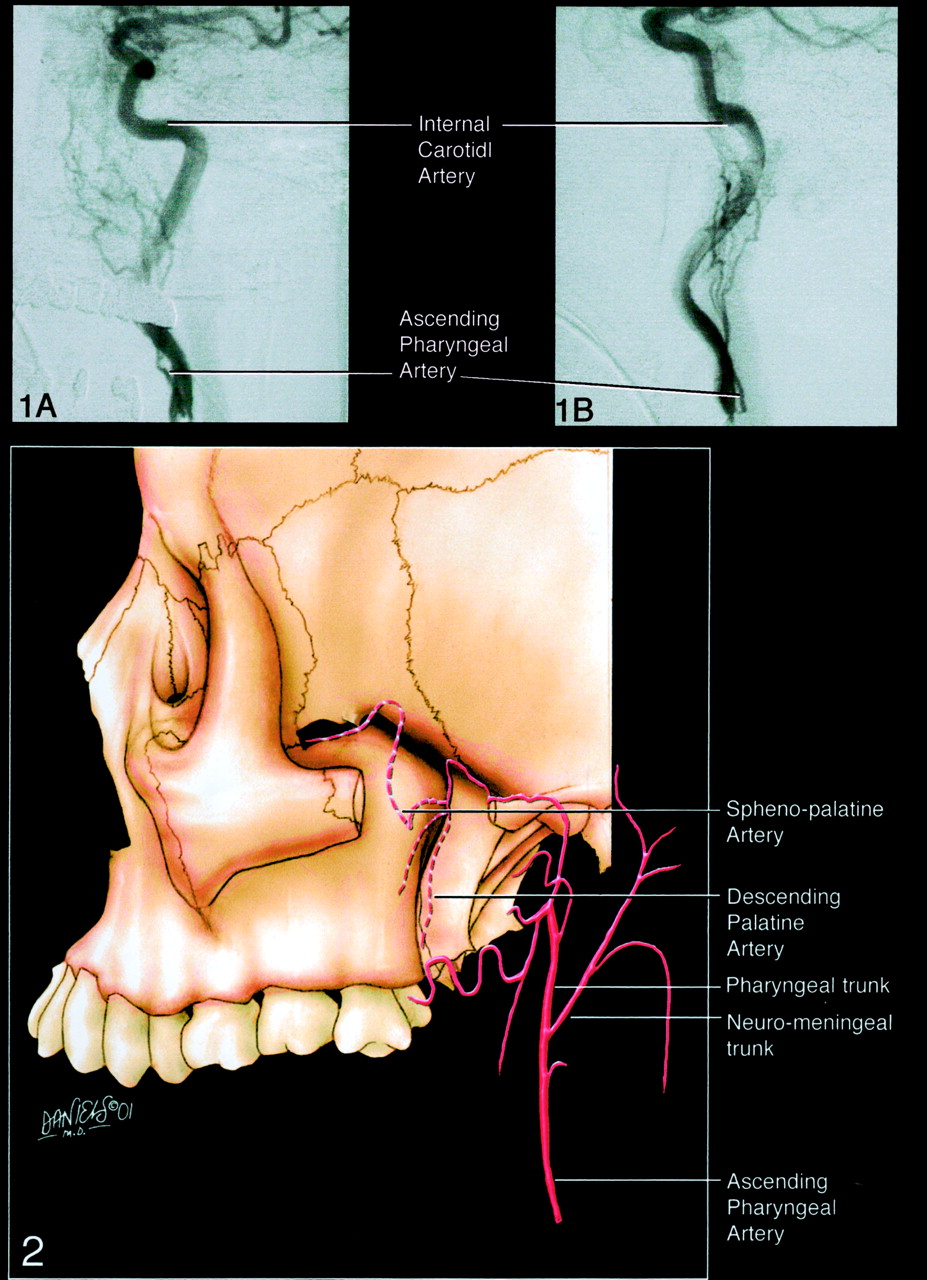
The ascending pharyngeal artery normally arises from the posterior wall of the proximal external carotid artery trunk, cephalad, and close to the source of the occipital artery (1, 2). However, the ascending pharyngeal artery may arise from the proximal occipital artery. Rare arrangements include origin from the internal carotid artery (3) (Fig 1A and B), or even from the ascending cervical artery. The latter configuration is explained by the separate origin of the ascending pharyngeal artery from the external carotid artery system in the embryo, where the ascending pharyngeal artery is part of the ventral pharyngeal territory.

A and B, Anteroposterior (A) and lateral (B) angiograms depict rare instances of the ascending pharyngeal artery arising from the internal carotid artery.
Branches
After a short common trunk, the ascending pharyngeal artery divides into two major trunks: anteriorly, the pharyngeal trunk, which is extracranial; posteriorly, the neuromeningeal trunk, which is intracranial and enters the posterior fossa through the foramen magnum (Fig 2) (1, 2). In rare instances, the neuromeningeal trunk may arise from the occipital artery or even the posterior auricular artery. The inferior tympanic branch arises between both trunks, and thus, is described separately because of its importance. Likewise, the musculospinal artery is described separately.
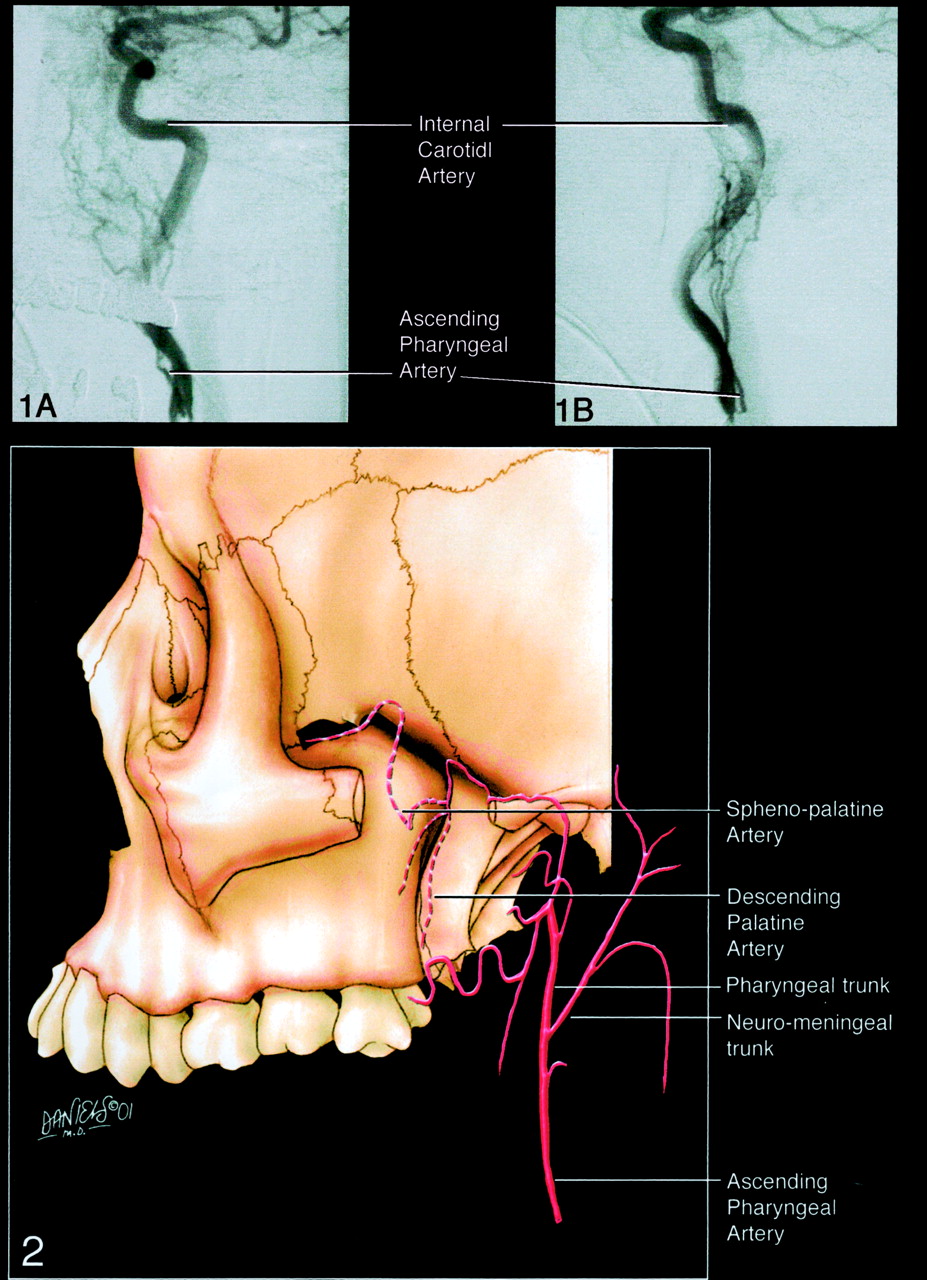
Diagram of the two major trunks of the ascending pharyngeal artery: anteriorly, the extracranial pharyngeal trunk; posteriorly, the neuromeningeal trunk, which is intracranial and enters the posterior fossa through the foramen magnum.
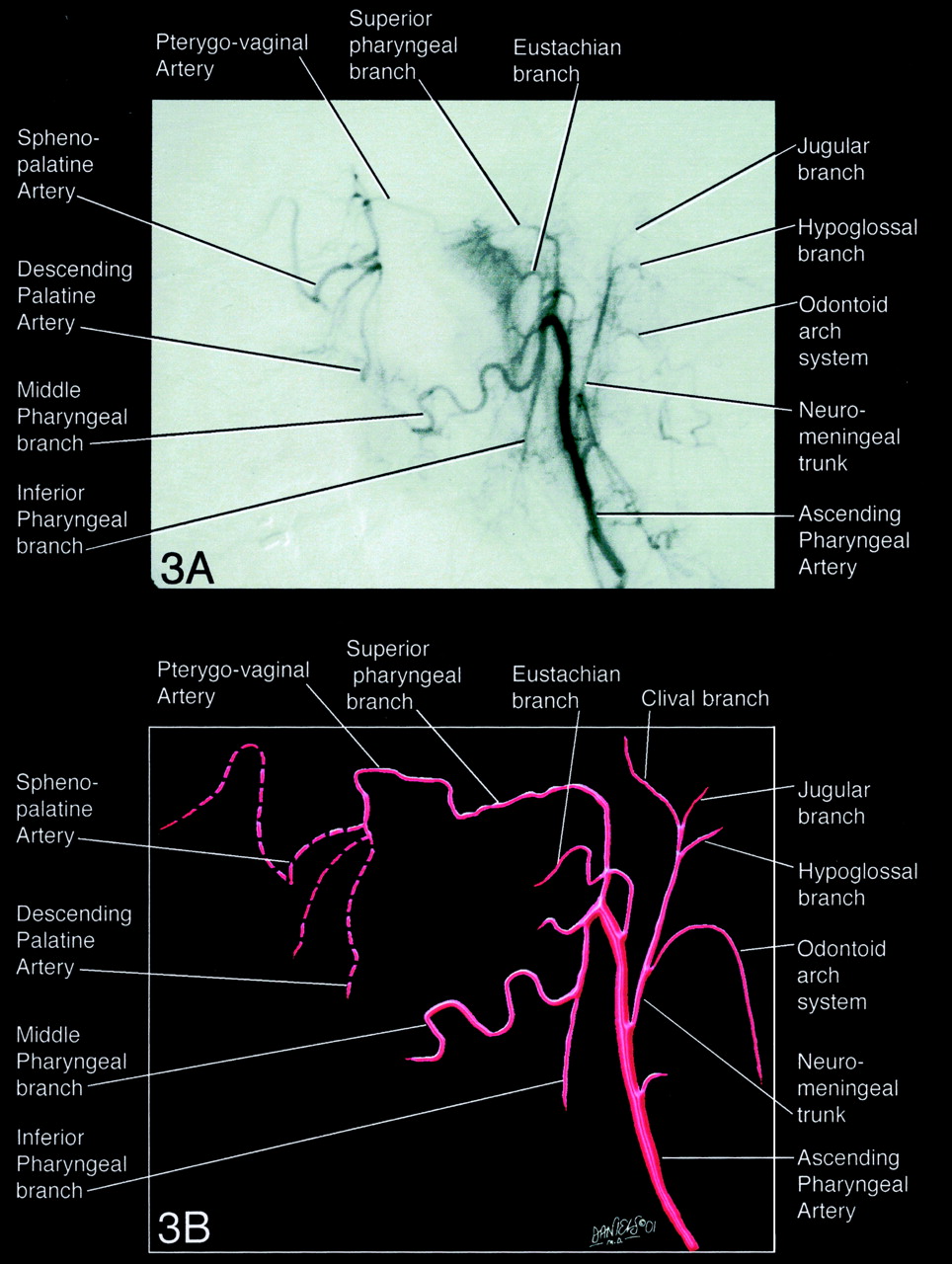
Pharyngeal Trunk.—The superior, middle, and inferior pharyngeal branches supply the pharyngeal submucosal spaces (Fig 3A and B). Abundant arterial anastomoses exist with the sphenopalatine system. A branch of the superior or middle pharyngeal artery system supplies the eustachian tube and the submucosal space of the fossa of Rosenmüller (Fig 3A and B). The superior pharyngeal artery may give rise to a carotid branch that runs along the internal carotid artery in the foramen lacerum and may anastomose with the inferolateral trunk.

Angiogram (A) and diagram (B) of the superior, middle, and inferior pharyngeal branches supplying the pharyngeal submucosal spaces.
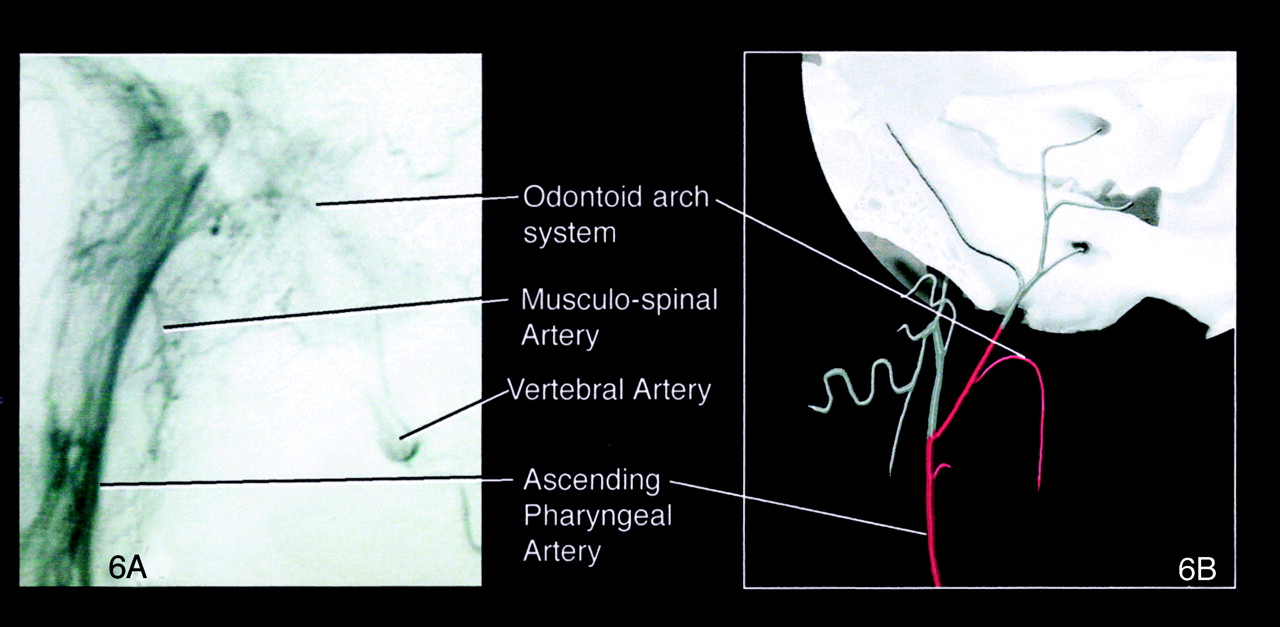
Neuromeningeal Trunk.—The two main divisions of the neuromeningeal trunk are the hypoglossal and jugular branches (Figs 4 and 5). The hypoglossal branch extends to the posterior fossa to the hypoglossal canal. It supplies the meninges of the posterior fossa and the vasa nervorum of cranial nerve XII. A posterior descending branch contributes to the odontoid arch system. This arterial arcade surrounds the dens and has transverse branches that anastomose with the anterior and posterior ascending arteries of the dens and is more concentrated around the neck of the odontoid (4). It also provides several branches that supply the first, second, and third cervical roots and the periosteum of the spinous processes and pedicles (Fig 6A and B). At the C2-C3 intervertebral space, it anastomoses with the vertebral artery. The jugular branch extends to the posterior fossa to the jugular foramen. It supplies the vasa nervorum of cranial nerves IX, X, and XI (5, 6). Three small branches leave the jugular foramen (Figs 4 and 5) to supply: superiorly, the meninges of the internal auditory canal; medially, the dura of the inferior petrosal sinus, and possibly, the vasa nervorum to cranial nerve VI proximal to Dorello’s canal; and laterally, the dura of the sigmoid sinus.

Diagram of the lateral view of the hypoglossal and jugular branches, the two main divisions of the neuromeningeal trunk. Top, superior view; bottom, inferior view; left, anterior view; right, posterior view.

View from above the hypoglossal and jugular branches. Top, superior view; bottom, inferior view; left, anterior view; right, posterior view.
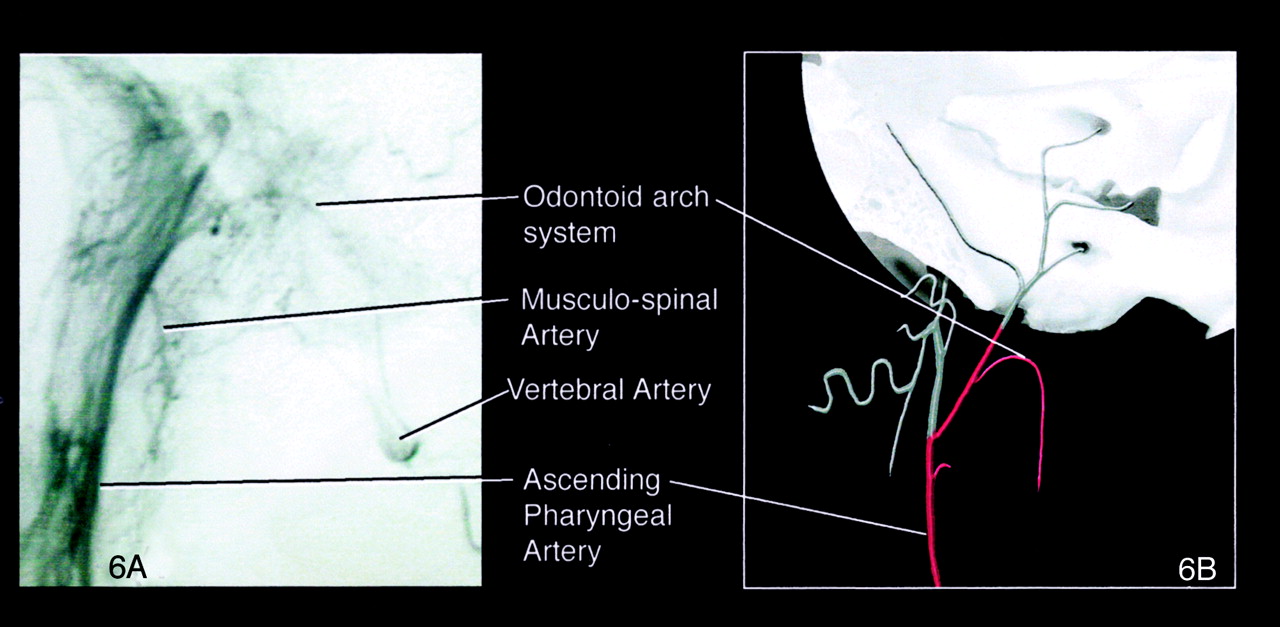
Angiogram (A) and diagram (B) of the odontoid arch system that gives rise to several branches that supply the first, second and third cervical roots and the periosteum of the spinous processes and pedicles. Top, superior view; bottom, inferior view; left, anterior view; right, posterior view.
Inferior Tympanic Branch
The inferior tympanic artery most commonly arises from the proximal aspect of the neuromeningeal trunk but can arise as a separate branch between the pharyngeal and neuromeningeal trunks (Fig 7A and B). It is close to cranial nerve IX and provides rami to the caroticotympanic branch of the internal carotid artery, the vasa nervorum of cranial nerve XI, and the vasa vasorum of the internal carotid artery. It also provides an anastomotic branch to the petrosquamosal branch of the middle meningeal artery and an anastomotic branch to the stylomastoid artery, which may supply the vasa nervorum to the facial nerve.
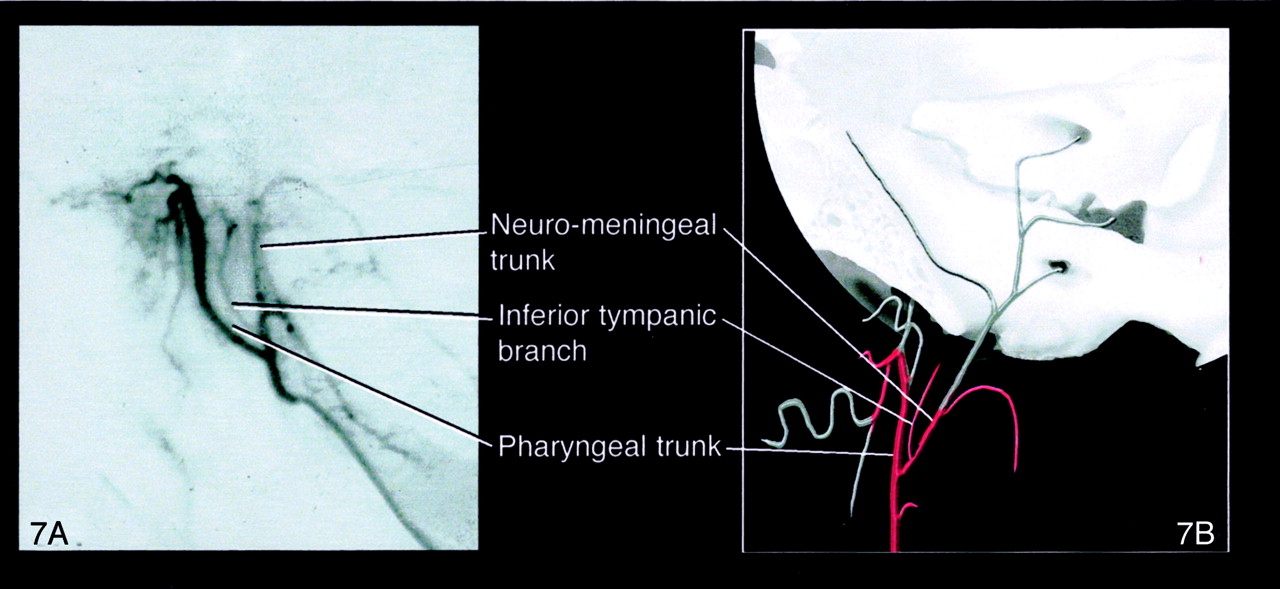
Angiogram (A) and diagram (B) of the inferior tympanic artery arising as a separate branch between the pharyngeal and neuropharyngeal trunks. Top, superior view; bottom, inferior view; left, anterior view; right, posterior view.
Musculospinal Artery
The musculospinal artery anastomoses with the vertebral artery at the level of the third intervertebral space (C2-C3) (Fig 6A and B). It also anastomoses with the most superior branch of the ascending cervical artery at C3 and with the deep cervical artery. It may supply the vasa nervorum to cranial nerve XI and the superior sympathetic ganglion.
Anastomoses to Major Arteries
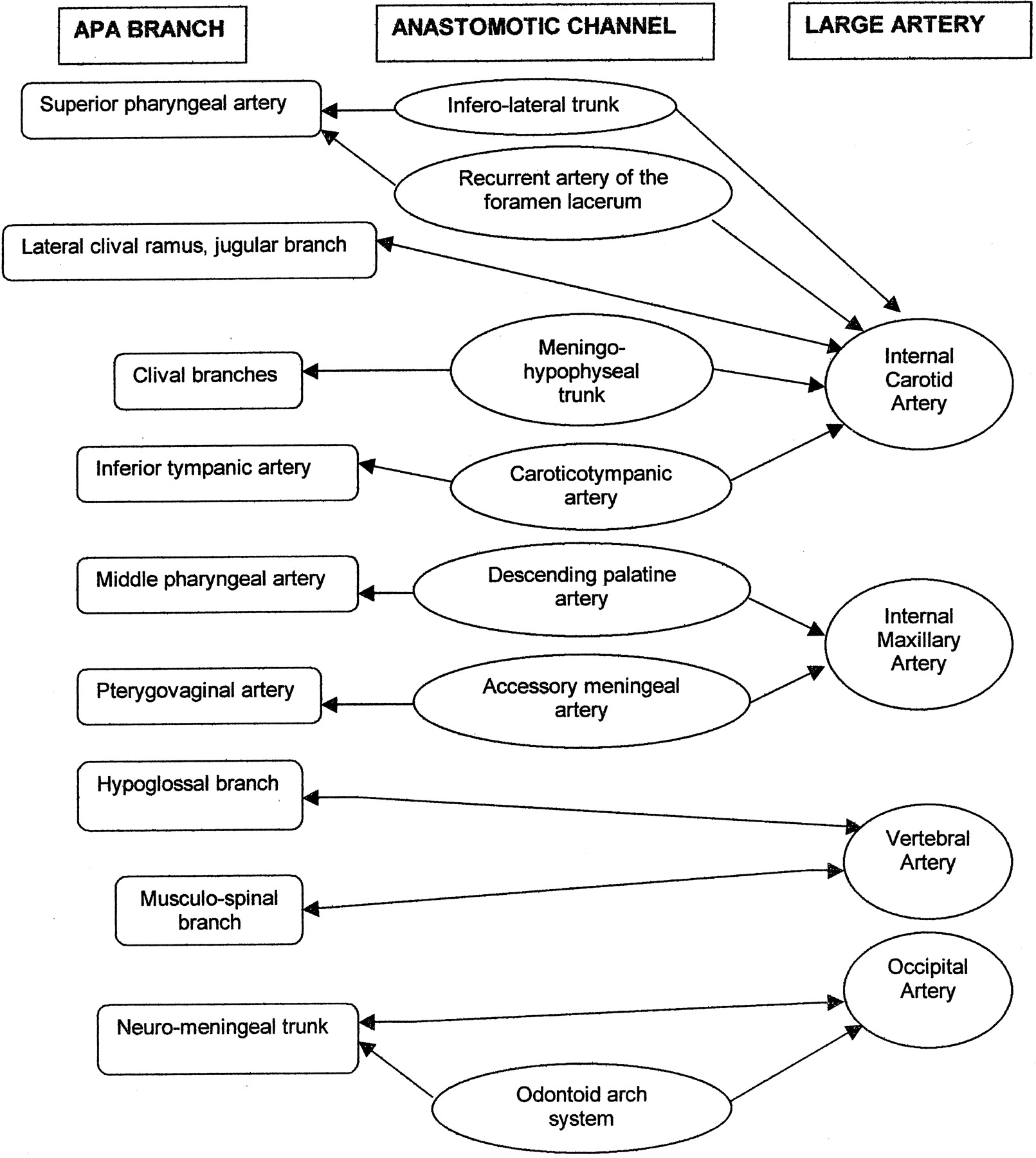
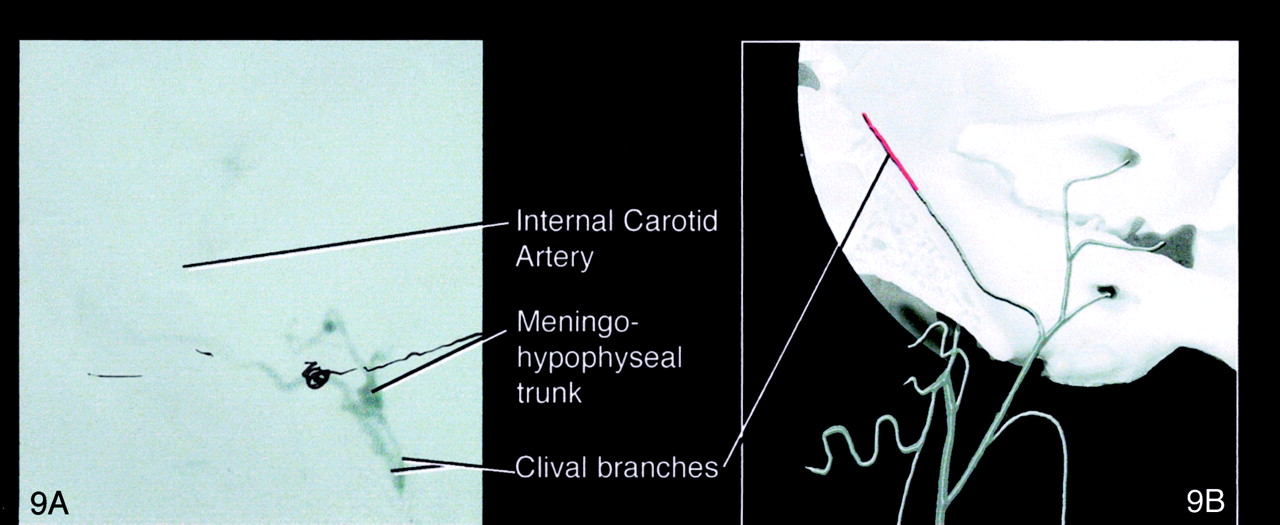
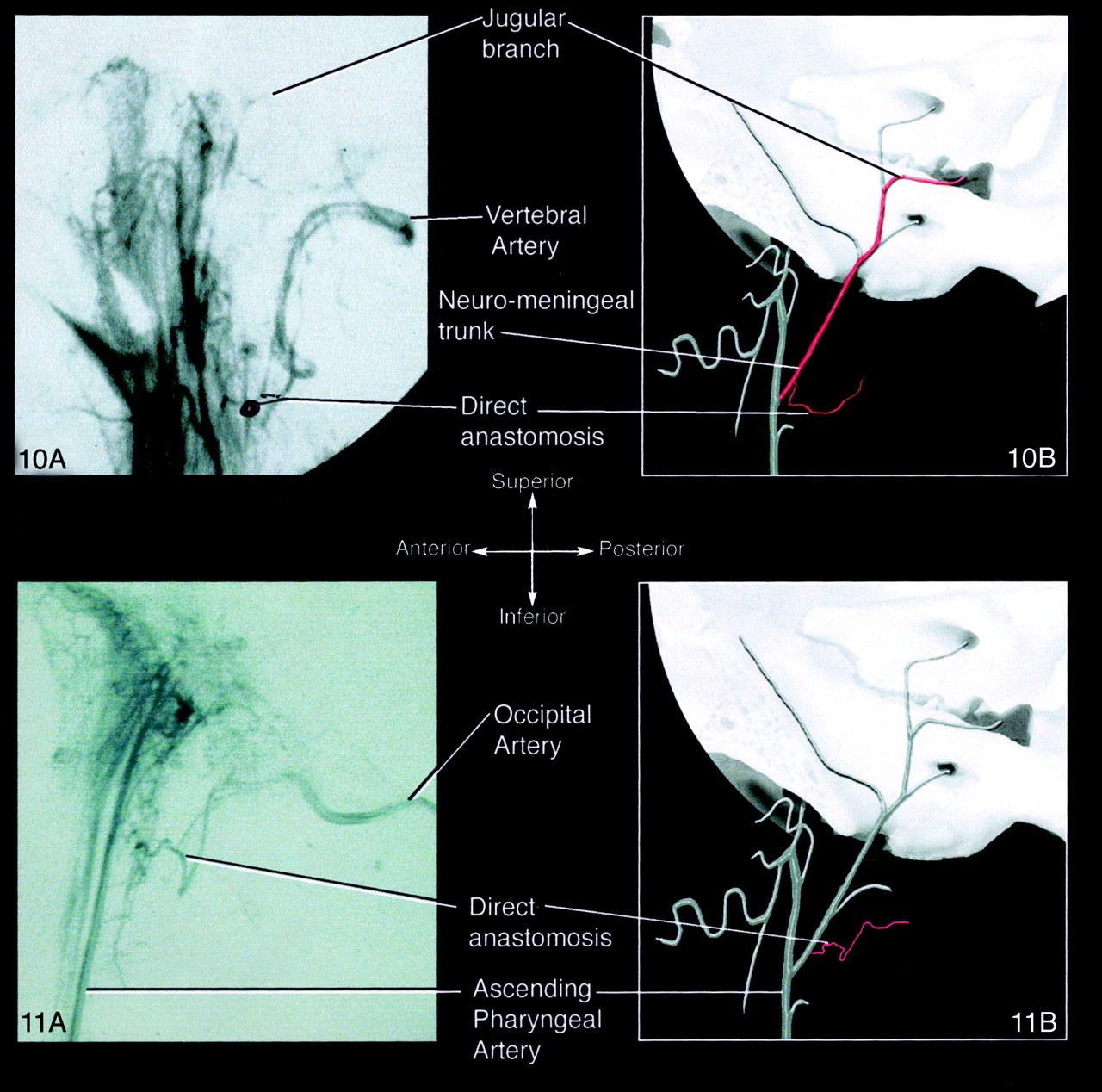
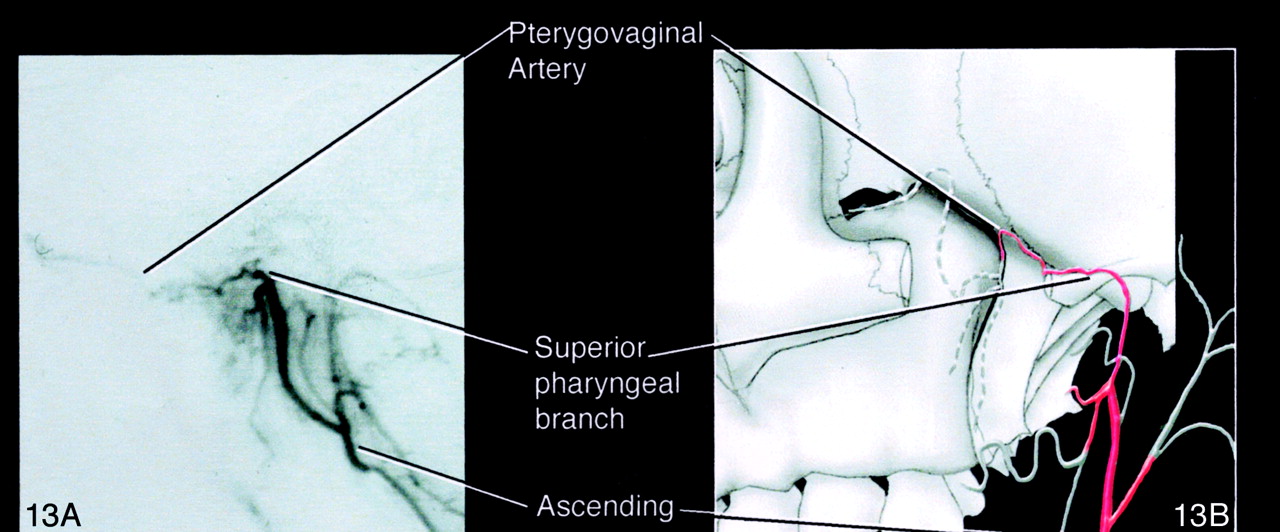
The ascending pharyngeal artery has potential anastomoses to all neighboring major arteries (Table and Fig 8). Anastomoses to the internal carotid artery are either direct via the lateral clival branch of the jugular artery or the recurrent artery of the foramen lacerum, or indirect, via the superior pharyngeal branch to the inferolateral trunk, the clival branches to the meningohypophyseal trunk (Fig 9A and B), or the inferior tympanic branch to the caroticotympanic branch. Anastomoses to the vertebral artery are through the hypoglossal branch and the musculospinal branch (Fig 10A and B). Anastomoses to the occipital artery can be either indirect through the odontoid arch system (Fig 11A and B) or direct through a common trunk (Fig 12A and B). Lastly, the ascending pharyngeal artery is connected to the internal maxillary artery at the level of the descending palatine artery through the middle pharyngeal branch (Fig 3A and B) or the pterygovaginal artery to the accessory meningeal artery (Fig 13A and B).
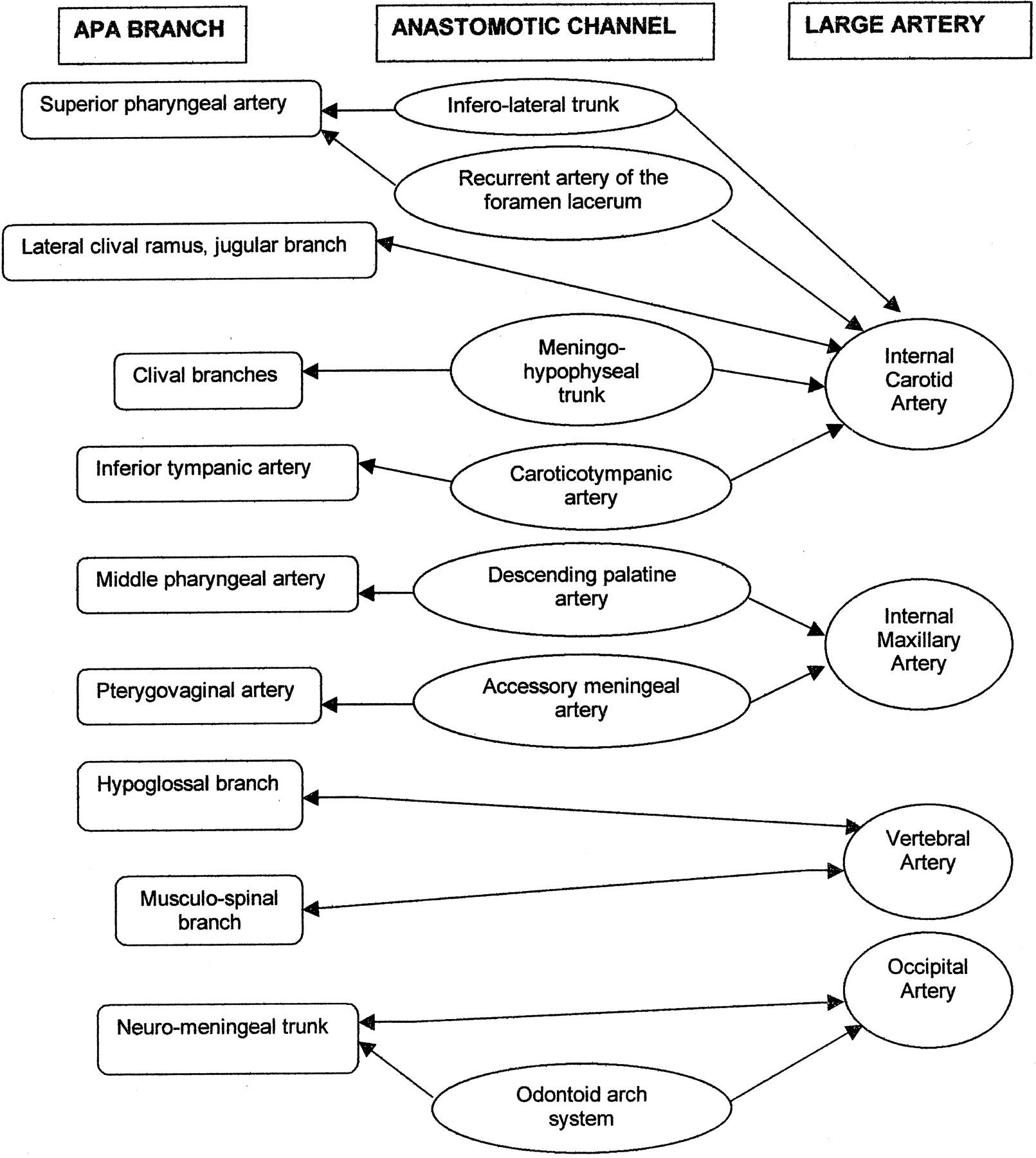
Diagram depicting ascending pharyngeal artery anastomoses.

Angiogram (A) and diagram (B) of the ascending pharyngeal artery communication with the internal carotid artery to the lateral clival branch of the jugular artery.

Angiogram (A) and diagram (B) of the ascending pharyngeal artery anastomoses to the vertebral artery via the hypoglossal branch and musculospinal branch. Top, superior view; bottom, inferior view; left, anterior view; right, posterior view.

Angiogram (A) and diagram (B) of anastomoses to the occipital artery via the odontoid arch. Top, superior view; bottom, inferior view; left, anterior view; right, posterior view.
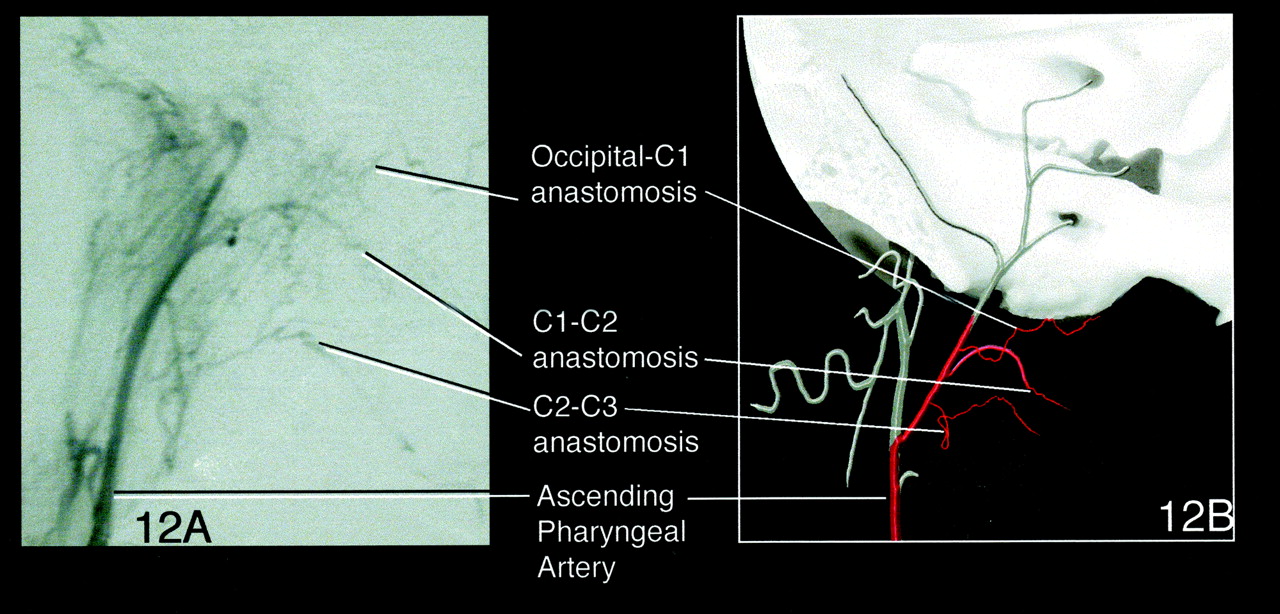
Angiogram (A) and diagram (B) of C1-C2 anastomoses to the occipital artery via the common trunk. Top, superior view; bottom, inferior view; left, anterior view; right, posterior view.

Angiogram (A) and diagram (B) of anastomoses via the pterygovaginal artery to the accessory meningeal artery. Top, superior view; bottom, inferior view; left, anterior view; right, posterior view.
Ascending pharyngeal artery anastomoses and foramina
Territory
Taylor and Palmer (7, 8) developed the concept of the angiosome, or vascular territory, in the late 1980s. These authors performed a rigorous dissection of tissue layers, including the skin, musculoaponeurotic system, muscles, bone, dura, and brain. Each layer was labeled and mapped to its respective arterial and venous contributors. Then the data were computer analyzed with color coding and three-dimensional reconstruction (7). In most cases, the territory of a superficial artery originating in the skin included the adjacent deep tissues, which generated the angiosome concept. Arteries were noted to closely follow the connective tissue framework. Direct cutaneous arteries of varying caliber, length, and attenuation are responsible for the skin supply in a given territory. In addition to this primary supply, numerous small indirect vessels reinforce the superficial vasculature before the main arteries penetrate to supply the deep tissues (8).
Thirteen angiosomes were defined in the head and neck region. These derive their supply from branches of the external carotid, internal carotid, and subclavian arteries, and their three-dimensional territories encompass skin, deep soft tissue, and bone. Only three of these angiosomes were noted to have no cutaneous involvement, containing only deep tissues. They were supplied by the ascending pharyngeal artery, the lingual artery, and the vertebral artery (7).
Clinical Relevance of the Ascending Pharyngeal Artery
Trauma
The ascending pharyngeal artery plays an important role in the healing process of Le Fort I osteotomies, because it supplies the attached posterior palatal soft-tissue pedicle. Le Fort osteotomies, as well as the fractures themselves, disrupt the pterygomaxillary junction by interrupting the descending palatine branches of the internal maxillary artery. Although an abundant mucosal alveolar anastomotic network in the maxilla remains, and the ascending palatine branch of the facial artery may be uninterrupted, much of the healing process is achieved by means of the ascending pharyngeal artery (9). In the same fashion, the ascending pharyngeal artery is directly involved in the closure of cleft palates (10).
Epistaxis
Embolization plays an increasing role in the management of epistaxis. Most commonly, the distal internal maxillary artery is the target vessel; less commonly, the facial artery serves as the site. Rarely is the ascending pharyngeal artery the only or a major source of severe epistaxis, requiring superselective embolization for successful control (11, 12).
High-Grade Head and Neck Tumors
Intraarterial embolization is proving to be useful for treating recurrent or high-grade head and neck cancers (13). Superselective microcatheter placement in various branches of the external carotid artery system is necessary for effective treatment. Specifically, superselective infusion of the ascending pharyngeal artery is necessary for successful embolization of cancer of the palate (13, 14).
Vascular Lesions
At the skull base, arteriovenous malformations and arteriovenous fistulas are uncommon but pose serious therapeutic challenges. Owing to its central position, the ascending pharyngeal artery can be a major feeder to arteriovenous fistulas (15) or arteriovenous malformations (16, 17).
Skull Base Tumors
Predictably, the ascending pharyngeal artery is the primary source of supply to meningiomas (Fig 13A and B) and glomus jugulare and tympanicum tumors (2) (Fig 14A and B) of the jugular foramen region. Giant cell tumors (18), hemangiopericytomas, and extramedullary plasmacytomas can occur in the jugular foramen, mimic glomus jugulare tumors in all aspects of their clinical and radiographic presentation (19), and derive their supply from the ascending pharyngeal artery. The ascending pharyngeal artery is even the primary vascular supply of the rare primary adenomatous tumor of the middle ear (20).

Angiogram (A) and diagram (B) of the ascending pharyngeal artery supplying a meningioma. Top, superior view; bottom, inferior view; left, anterior view; right, posterior view.
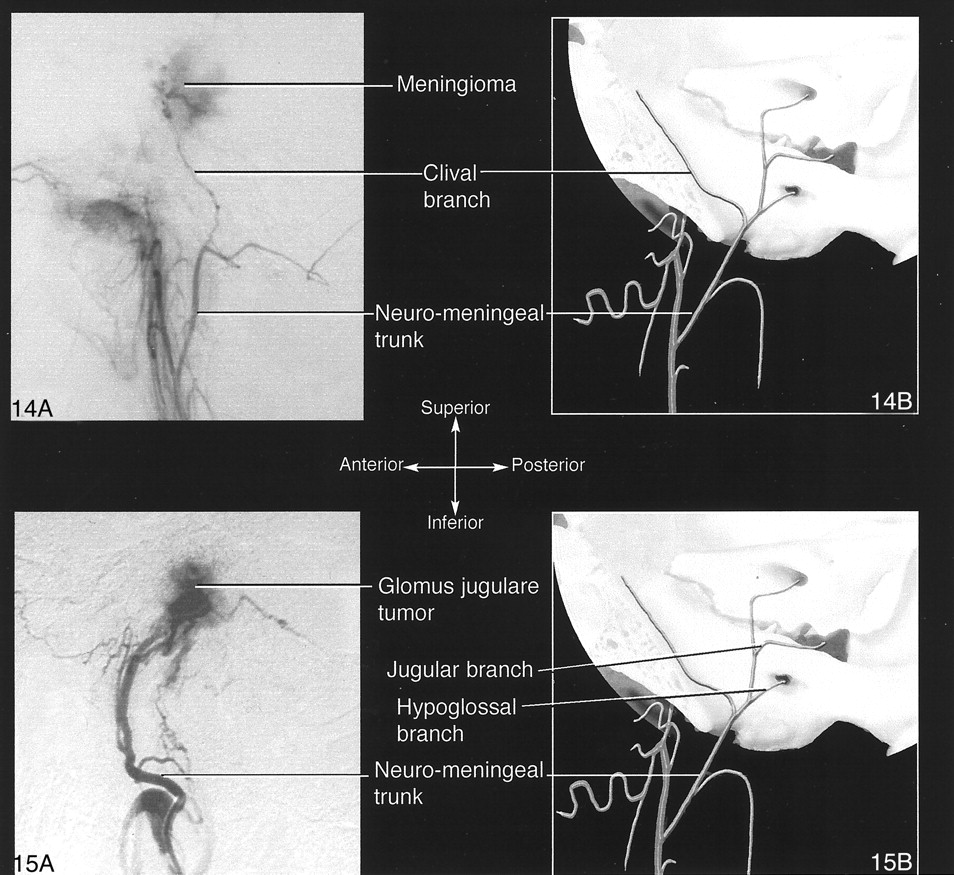
Angiogram (A) and diagram (B) of the ascending pharyngeal artery supplying a glomus jugulare tumor. Top, superior view; bottom, inferior view; left, anterior view; right, posterior view.
Subarachnoid Hemorrhage
Subarachnoid hemorrhage from rupture of a saccular aneurysm of the posterior clival meningeal branch of the ascending pharyngeal artery has been reported (21).
Collaterals to Agenetic or Occluded Internal Carotid Artery
The ascending pharyngeal artery can function as collaterals to an agenetic internal carotid artery (22), in which case the most common configuration is replacement of the petrous segment with an intratympanic ascending pharyngeal artery loop. The ascending pharyngeal artery can also be recruited in case of an occluded internal carotid artery (23). Persistent collateral circulation with the distal carotid artery at the skull base has been described and shown to be a potential source of emboli into the retinal or intracranial territories (24).
Neurovascular Research Models
Because it has vascular characteristics likened to those of an arteriovenous malformation nidus, the swine rete mirabile has been proposed as a model to study the kinetics of liquid embolic agents (25, 26). The ascending pharyngeal artery supplies the rete mirabile.
Conclusion
The ascending pharyngeal artery, although small, is an important vessel with a territory that includes several deep extra- and intracranial structures involved in a variety of disease processes. A three-dimensional representation of the vessel’s territory and major anatomoses may help the reader to better appreciate these points.
Acknowledgments
The authors are indebted to Cathy Marszalkowski for expert assistance in editing this work.
References
- Received August 16, 2001.
- Accepted after revision January 29, 2002.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Endovascular treatment strategy, technique, and outcomes for dural arteriovenous fistulas of the marginal sinus region
- Anatomical Structures, Cell Types, and Biomarkers Tables Plus 3D Reference Organs in Support of a Human Reference Atlas
- Variant ascending pharyngeal artery maintaining flow in a subocclusive internal carotid artery
- Transvenous coil embolization with intra-operative cone beam CT assistance in the treatment of hypoglossal canal dural arteriovenous fistulae
- The road less traveled: transarterial embolization of dural arteriovenous fistulas via the ascending pharyngeal artery
- Onyx embolization of dural arteriovenous fistulas of the cavernous sinus through the superior pharyngeal branch of the ascending pharyngeal artery
- Onyx embolization of dural arteriovenous fistulas of the cavernous sinus through the superior pharyngeal branch of the ascending pharyngeal artery
- Severe epistaxis after nasogastric tube insertion requiring arterial embolisation
- Balloon-augmented Onyx embolization of a dural arteriovenous fistula arising from the neuromeningeal trunk of the ascending pharyngeal artery: technical report
- Dangerous Extracranial-Intracranial Anastomoses and Supply to the Cranial Nerves: Vessels the Neurointerventionalist Needs to Know