
Abstract
BACKGROUND AND PURPOSE: Maneuvers that distend a lumen facilitate radiographic examinations. In evaluation of the upper aerodigestive tract, Valsalva and phonation maneuvers complement barium fluoroscopy. The current work investigates “puffed-cheek” CT to improve visualization of oral cavity tumors.
METHODS: Seven patients (ages 17 to 86 years) underwent conventional and puffed-cheek CT. Five had squamous cell carcinoma, one had benign verrucous hyperplasia of the buccal mucosa, one had “cheek swelling,” and one had a pulsatile cheek mass. Conventional contrast-enhanced axial CT scans (3-mm thick, no interslice gap) were obtained through the oral cavity and neck. Each patient then pursed the lips and puffed out the cheeks, and axial images were obtained through the oral cavity (puffed-cheek scans).
RESULTS: Three patients had normal conventional CT scans whereas puffed-cheek scans clearly showed the mass. Conventional CT in three patients showed a mass inseparable from two mucosal surfaces whereas puffed-cheek images clearly showed which surface the tumor involved. Two patients had normal conventional and puffed-cheek CT studies; in one, the physical examination was also normal. The other patient was a teenager with orthodontic appliances that created artifacts on both conventional and puffed-cheek images. Conventional angiography in this patient revealed a facial artery aneurysm.
CONCLUSION: The puffed-cheek CT maneuver is easily taught, and patients comply readily. Puffed-cheek CT scans provide a clearer and more detailed evaluation of mucosal surfaces of the oral cavity than do conventional scans. In selected patients, the puffed-cheek technique can supplement conventional CT studies.
Small mucosal tumors of the oral cavity are usually not visible on conventional CT studies. Large, bulky tumors are apparent, but CT may not be able to determine the surface of origin of a bulky tumor.
Phonation and other maneuvers that distend a normally collapsed lumen facilitate examination of the upper aerodigestive tract for clinicians and radiologists (1–5). This report investigates the usefulness of one such maneuver, the “puffed-cheek” CT scan.
Methods
Between 1991 and 1997, seven patients (four women and three men, ages 17 to 86 years) for whom there was a histologic diagnosis or clinical concern of a tumor or mass of the oral cavity or cheek underwent both conventional and puffed-cheek CT imaging. Five patients either were known to have or were subsequently shown to have squamous cell carcinoma (three of these tumors arose from or involved the buccal mucosa, one arose from the retromolar trigone, and one arose from the maxillary alveolar ridge), one patient had benign verrucous hyperplasia of the buccal mucosa, one patient reported “cheek swelling,” and one patient had a pulsatile cheek mass, for a total of eight types of abnormality in the seven patients. (One patient had squamous cell carcinoma on one side of the oral cavity and verrucous hyperplasia on the other side.)
Axial CT scans (3-mm thick with no interslice gap) were initially obtained through the oral cavity and neck after intravenous administration of contrast material. These constituted the conventional CT scans. Each patient was then asked to purse the lips and puff out the cheeks. Additional axial images (3- or 5-mm thick with no interslice gap) were obtained through the oral cavity (hard palate through mandible). These constituted the puffed-cheek CT scans. The locations for the small number of additional images were selected from the initial axial scans. Additional intravenous contrast material was not administered, but residual contrast agent was usually present. One radiologist interpreted both the conventional and puffed-cheek images.
Results
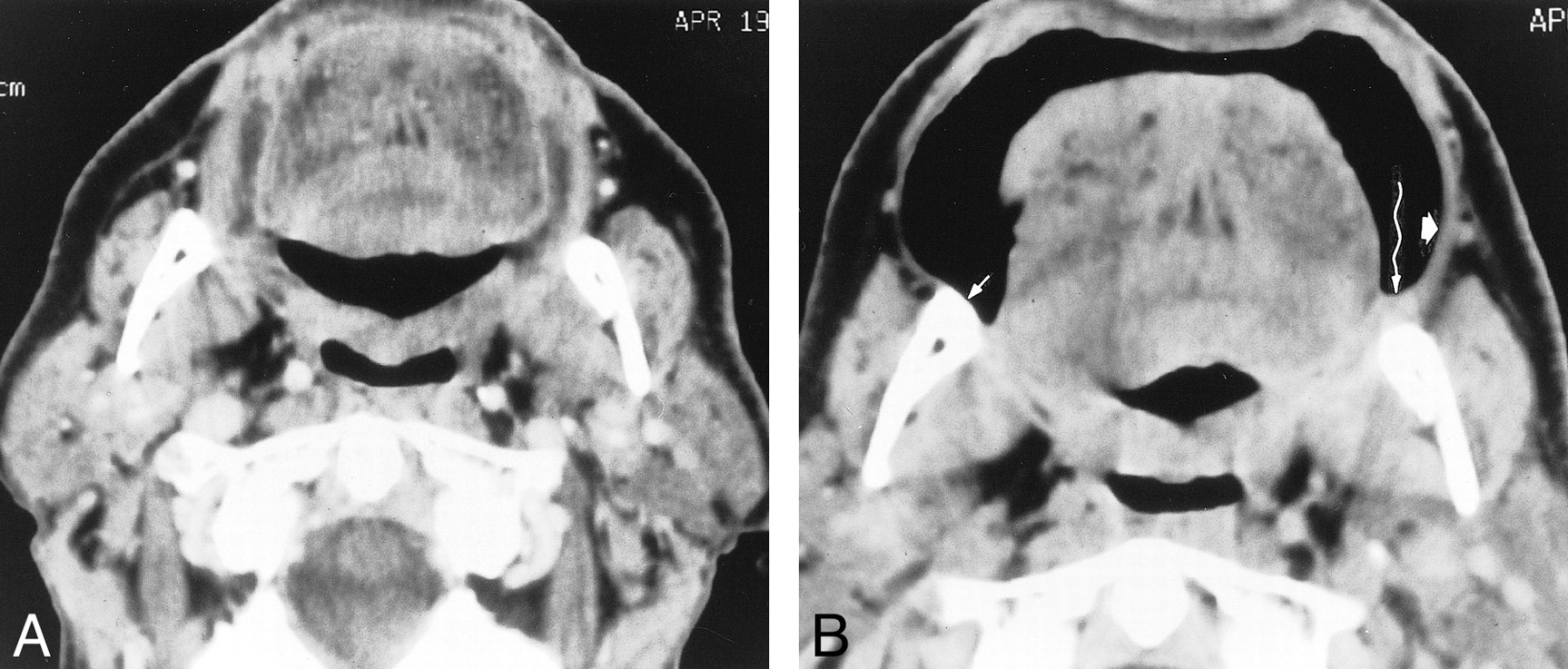
In two patients, both the conventional and the puffed-cheek CT scans were normal (Fig 1). In one of these (Fig 1A), the physical examination was also normal, and no source for the patient's complaint of cheek swelling was identified. The other patient was a teenager with orthodontic appliances that created significant artifacts on both the conventional and puffed-cheek CT studies (Fig 1B). A facial artery aneurysm was subsequently identified at conventional angiography.

Normal anatomy on puffed-cheek CT scans in two patients. A, 42-year-old woman with cheek swelling. Puffed-cheek axial CT scan at the level of the maxilla is normal. The patient's physical examination and subsequent follow-up were also normal. The muscles of facial expression, seen especially well on the puffed-cheek CT scan, include the orbicularis oris (long arrows), levator anguli oris (open white arrows), risorius, and buccinator. Note streak artifacts from the mandible bilaterally (open black arrows). B, 18-year-old man with a facial artery aneurysm. Puffed-cheek axial CT scan at the level of the mandible is normal. The orbicularis oris muscle thickens laterally (arrows), where depressor anguli oris and risorius interdigitate and insert. The buccinator and buccal mucosa create a homogeneous soft tissue band (arrowheads), partially distorted here by the streak artifacts from orthodontic appliances. A skin marker on the right cheek (unmarked) indicates the clinically palpable aneurysm
Three patients had no abnormality on conventional CT scans but the puffed-cheek CT scan clearly showed a mass (Figs 2 and 3). Two of these patients had squamous cell carcinoma and one had verrucous hyperplasia of the buccal mucosa.

61-year-old man with invasive squamous cell carcinoma of the left buccal mucosa. A, Conventional axial CT scan through the occlusal plane is normal. B, Puffed-cheek axial CT scan shows an exophytic nodule (straight arrow) on the left buccal mucosa. The buccal mucosa and buccinator muscle together form a smooth soft tissue band (arrowheads). Curved arrows indicate orbicularis oris and associated muscles
The conventional CT studies in three patients showed a mass in the oral cavity that was inseparable from two mucosal surfaces (Fig 4A). The puffed-cheek images clearly showed which surface the tumor involved (in the case of Fig 4B, both surfaces). All these tumors were squamous cell carcinomas. In each case of tumor, puffed-cheek studies showed the location and extent of the tumor better than conventional CT scans did.
64-year-old man with squamous cell carcinoma of the retromolar trigone. A, Conventional axial CT scan below the occlusal plane is normal. B, Puffed-cheek axial CT scan shows a small tumor in the left retromolar trigone (wavy arrow), inseparable from the mandible. The right retromolar trigone is normal (short thin arrow). The buccinator/buccal mucosa complex is thicker on the side of the tumor (short wide arrow) than on the normal (right) side
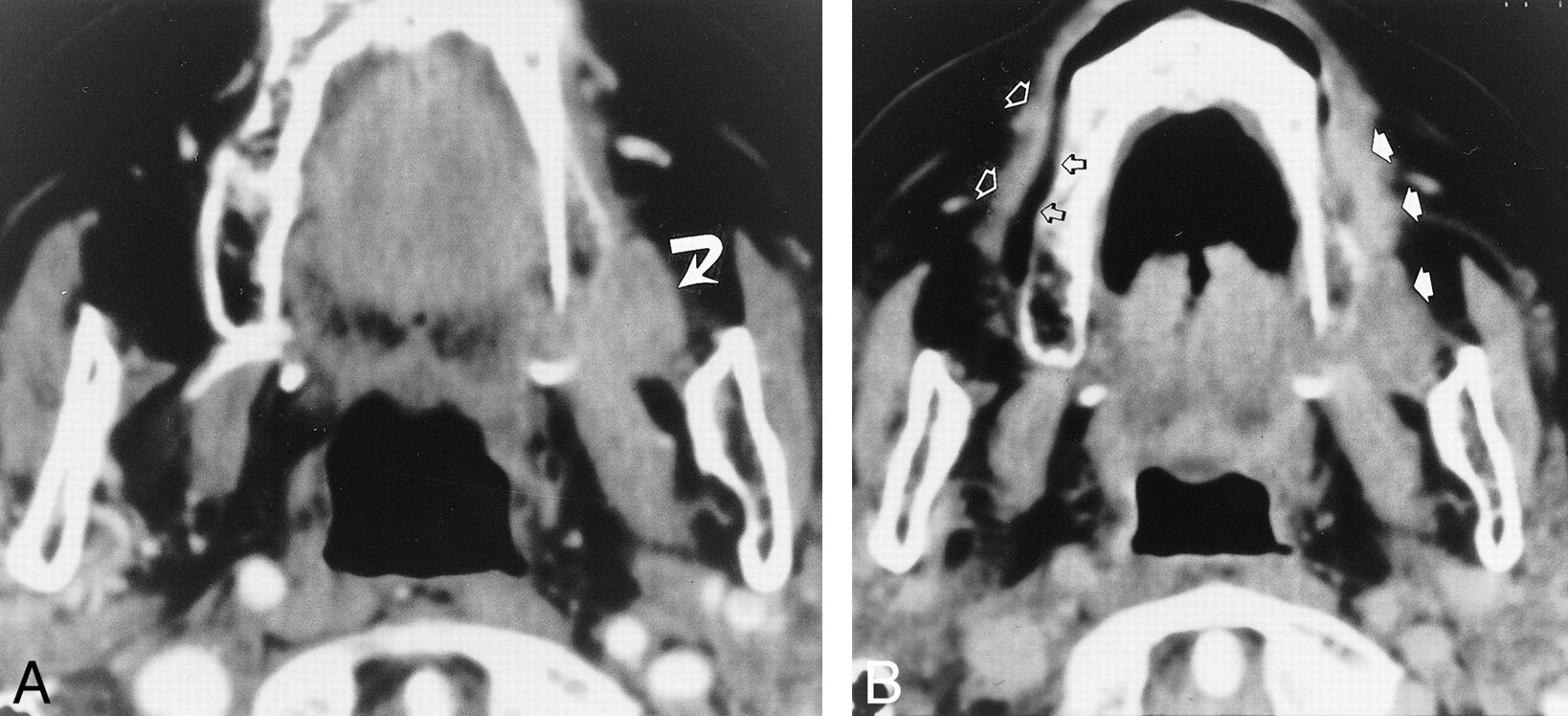
77-year-old woman with squamous cell carcinoma of the maxilla. A, Conventional axial CT scan through the lower maxilla shows the tumor (arrow) inseparable from the gingival (alveolar) and buccal (cheek) mucosal surfaces. B, On the normal (right) side, the puffed-cheek axial CT scan separates the gingival mucosa and the alveolus (open black arrows) from the buccal mucosa and the buccinator muscle (open white arrows). The tumor thickens the cheek on the left side (solid arrows) and extends around the sulcus to the gingival mucosa. The combination of direct extension of tumor and decreased pliability of the cheek because of tumor invasion makes the two surfaces (buccal, gingival) inseparable
Discussion
The oral cavity includes the anterior two thirds of the tongue, the floor of the mouth, the mandibular alveolus, the maxillary alveolus, the hard palate, the lips, and the cheeks (buccomasseteric region) (6). The oral cavity lies anterior to the soft palate, the anterior tonsillar pillars, and the circumvallate papillae of the tongue (6).
Visual inspection and bimanual palpation are the cornerstones of diagnosis of oral cavity disease (7). Apposition of two mucosal surfaces limits both the clinical and radiologic examinations. In the upper aerodigestive tract, phonation and Valsalva maneuvers that distend the lumen with air reveal the mucosa in greater detail and allow a more detailed evaluation of tumors (1–5). For example, saying “eeeeee” distends the tonsillar fossae, valleculae, and pyriform sinuses (2). When the patient puffs against a finger held at his lips as if “to inflate a balloon” (3), he distends his hypopharynx, especially the pyriform sinuses and postcricoid region.
Perhaps because the oral cavity is eminently accessible to clinical examination (8), CT and MR studies are not primary diagnostic tools. Rather, CT and MR complement the clinical examination by delineating deep extension of tumors, including bone erosion, and by identifying metastatic cervical lymphadenopathy.
CT and MR examinations of oral cavity tumors have two important limitations. A small mucosal tumor is often invisible on CT or MR images; it may be impossible to determine which surface a tumor arises from (or invades) when two mucosal surfaces are in contact (apposed). Neither limitation renders the study useless. The primary role of CT or MR imaging is to evaluate deep invasion by tumor and to identify (or exclude) cervical lymphadenopathy. However, knowing (and seeing) the precise location of any abnormality generally improves (and focuses) the radiologist's evaluation. Puffed-cheek CT scans can show the tumor location when the location might otherwise not be known. Admittedly, this information is usually readily apparent on clinical examination, but the radiologist does not always have the time or opportunity to examine the patient or to discuss the case in detail with the referring clinician.
The surfaces of the oral cavity that are often in contact are the buccal (cheek) mucosa more posteriorly or the labial (lip) mucosa more anteriorly, and the alveolar (gingival) mucosa of the mandible and maxilla. In puffed-cheek CT scans of the oral cavity, air separates these mucosal surfaces. Air in the oral cavity will highlight a bulky exophytic mass, a subtle wall thickening, and an ulceration. Air makes such an excellent “contrast medium” that, in the current study, bone algorithms added little to the information on the soft tissue algorithms (Fig 5). The frenulum of the upper lip, a normal structure, was more conspicuous on the bone algorithm (Fig 5B). However, the soft tissue algorithms showed details of the tumor better. Bone algorithms were therefore deemed unnecessary except to evaluate bone erosion.

86-year-old woman with verrucous hyperplasia of the buccal mucosa. A, Puffed-cheek axial CT scan (soft tissue algorithm) shows the exophytic mass (arrows). B, Puffed-cheek axial CT scan (bone algorithm) also shows the mass (short arrows). Only the bone algorithm shows the frenulum of the upper lip (long arrow), a normal structure. However, the soft tissue algorithm provides much greater detail of the tumor
Puffed cheek images are useful for the assessment of both benign (Figs 1 and 5) and malignant (Figs 2–4) disease. The one false-negative finding in this study was a mass (facial artery aneurysm) deep within the cheek (Fig 1B). The lack of a mucosal component may explain the inability of CT to show the aneurysm. However, an even greater limiting factor may have been the pronounced streak artifacts from the young patient's orthodontic appliances.
The puffed-cheek maneuver is easily taught, and patients comply readily. Initially, the patients were asked to suspend respiration for the duration of the maneuver. Subsequently, it became apparent that it is possible to puff out the cheeks and continue breathing quietly. This further improved patient compliance and the quality of the study.
The puffed-cheek maneuver added a negligible amount of time to the total scan duration. To create a brief and tailored study, precise scanning locations were chosen from the conventional (nonpuffed) images.
Puffed-cheek images show unfamiliar normal anatomy that could be mistaken for disease. The muscles of facial expression—among them, the risorius, the levator anguli oris, the depressor anguli oris, and the orbicularis oris muscles (9)—create conspicuous soft tissue “masses” when the cheeks are stretched by air (Figs 1A and B, 2B, and 3B). The buccinator muscles (Figs 1A and B, 2B, and 3B) are seen better on puffed-cheek images than on the conventional CT scans, but these broad, bandlike muscles are unlikely to be mistaken for disease. To date, there is no evidence that the puffed-cheek maneuver obscures findings.
The current study is small, and includes only CT studies. The same maneuver could be used with MR imaging, although it might be slightly more awkward for patients to sustain the puffed-cheek maneuver for the 3 to 5 minutes required for even a fast spin-echo MR pulse sequence.
Conclusion
Puffed-cheek CT scans provide a clearer and more detailed evaluation of mucosal surfaces of the oral cavity than do conventional (nonpuffed) images. In selected patients, the puffed-cheek technique can supplement conventional CT.
Acknowledgments
I am grateful to Christine Wagner for her gracious and good-natured assistance throughout a variety of manuscript alterations.
Footnotes
1 Presented in part at the annual meeting of the American Society of Neuroradiology, Philadelphia, May 1998.
↵2 Address reprint requests to Jane L. Weissman, MD.
- Received July 31, 2000.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cross-Sectional Imaging of Third Molar-Related Abnormalities
- Imaging the oral cavity: key concepts for the radiologist
- Gauze Padding: A Simple Technique to Delineate Small Oral Cavity Tumors
- Evaluating "Eee" Phonation in Multidetector CT of the Neck
- Tumor Volume Assessment by 18F-FDG PET/CT in Patients with Oral Cavity Cancer with Dental Artifacts on CT or MR Images