
Abstract
SUMMARY: Fluid-fluid levels can occur whenever different fluid densities are contained within a cystic or compartmentalized lesion, usually related to the evolution of hematoma or necrosis. Review of the literature demonstrated that throughout the skeletal system, the most common etiology for fluid-fluid levels is aneurysmal bone cyst, but there are no dedicated studies of the pediatric calvaria, to our knowledge. In this report, we present clinicopathologic characteristics and CT and MR imaging of 11 patients with pediatric skull mass lesions demonstrating fluid-fluid levels. MR imaging demonstrated more fluid-fluid levels compared with CT in all cases. The etiologies of skull lesions with fluid-fluid levels were Langerhans cell histiocytosis in 4 (36.6%), aneurysmal bone cysts in 3 (27.2%), cephalohematoma in 3 (27.2%), and metastatic neuroblastoma in 1 (9%). Radiologists should be aware of the other etiologies of calvarial lesions with fluid-fluid levels in the pediatric skull.
ABBREVIATIONS:
- ABC
- aneurysmal bone cyst
- FFL
- fluid-fluid level
- LCH
- Langerhans cell histiocytosis
Fluid-fluid levels (FFLs) may occur whenever different fluid densities are contained within a cystic or compartmentalized structure, usually related to hemorrhage or necrosis.1,2 Image acquisition near perpendicular to the plane of the FFL is required to optimally demonstrate it.1,2 FFLs in skeletal lesions have been a well-known imaging feature of aneurysmal bone cyst (ABC)3,4 for many decades. To our knowledge, there is no dedicated study focusing on the different etiologies of FFLs in the pediatric population and there is no study focused on fluid-fluid levels in calvarial lesions. However, 2 large studies primarily in adult patients have demonstrated that ABCs are the most common etiology of osseous lesions with FFLs throughout the body.5,6 Despite these data, the presence of FFLs remains a nonspecific finding and can be seen in a wide range of benign and malignant bone lesions, including fibrous dysplasia, telangiectatic osteosarcoma, osteoblastoma, simple bone cyst, lymphatic malformations, Ewing sarcoma, brown tumor, giant cell tumor, and chondroblastoma.5⇓⇓⇓–9
In this study, head CT and MR imaging of pediatric patients having skull lesions with FFLs were retrospectively reviewed with the aim of characterizing these lesions.
Case Series
Patients
The study was performed with approval of the institutional review board and was compliant with guidelines of the Health Insurance Portability and Accountability Act. We performed a retrospective review of records of pediatric patients with skull masses diagnosed between 2002 and 2012. Cases were ascertained from teaching files of the authors and a computerized search of the PACS for patients younger than 18 years of age who were diagnosed with a skull lesion showing fluid-fluid levels on CT or MR imaging. The search terms included various combinations and derivatives of “fluid-fluid,” “blood-fluid,” “fluid levels,” “skull,” and “calvarium.” Medical records were reviewed for patient age, sex, history of recent trauma to the lesion, history of coagulopathy, types of treatment, and histopathologic diagnosis. Patients with a history of surgery on the skull were excluded. The etiologic diagnosis was made by histopathologic examination of resected lesions in 6 patients and of biopsied specimens in 1 patient. In 3 patients who were classified as having cephalohematoma, the diagnosis was made on the basis of characteristic clinical presentation, history of traumatic vaginal delivery, and/or spontaneous resolution of the lesion by consensus of pediatric neuroradiologists and by review of medical records. Finally, 1 patient with primary neuroblastoma was diagnosed as having metastatic involvement of the skull on the basis of typical imaging findings of neuroblastoma both on CT and MR imaging and considerable improvement of the lesion after targeted chemotherapy.
CT and MR Imaging
CT was performed on various multidetector CT scanners (Siemens, Erlangen, Germany), and MR imaging was performed on 1.5T or 3T magnets (Siemens) with standard clinical protocols used at the time of the study. Axial CT sections were reconstructed at 3- or 5-mm thicknesses. MR imaging sequences varied among patients but generally included pre- and postcontrast T1-weighted, T2-weighted, fluid-attenuated inversion recovery, echo-planar spin-echo diffusion-weighted imaging, and either T2* gradient-echo susceptibility or susceptibility-weighted imaging.
The CT and MR imaging studies of these patients were reviewed by 2 pediatric neuroradiologists by consensus, and the findings were tabulated. For each scan, lesion location, number of fluid-fluid levels, and the presence or absence of soft-tissue components were evaluated. Diagnosis of hemorrhage was based on hyperattenuation on noncontrast CT or typical MR imaging findings (mainly hyperintensity on T1-weighted, hypointensity on T2-weighted, and/or susceptibility on gradient-echo or susceptibility-weighted images).
Clinicopathologic and Imaging Findings
Eleven patients (6 male, 5 female) with skull lesions showing fluid-fluid levels met the inclusion and exclusion criteria (Table). The mean age of patients at the time of primary diagnosis was 6.2 ± 6.1 years (range, 8 days to 16 years). The etiologies of the lesions included Langerhans cell histiocytosis (LCH) (n = 4 [36.6%]), aneurysmal bone cyst (n = 3 [27.2%]), cephalohematoma (n = 3 [27.2%]), and neuroblastoma (n = 1 [9%]).
Demographic, clinical, imaging, and histopathologic findings of pediatric patients with FFLs in skull lesions
In 7 patients, both CT (4 noncontrast, 3 contrast-enhanced) and MR imaging with and without contrast were performed. MR imaging with and without contrast was the only imaging technique in another 4 patients. In the 7 patients in whom a CT had been performed, FFLs were identified in 6 patients (85%). The mean number of fluid-fluid levels detected on CT was 3.5 ± 3.2 (range, 1–9). FFLs were present on MR imaging in all 11 patients (100%). The mean number of detected fluid-fluid levels on MR imaging was 9.2 ± 9.1 (range, 1–29). The number of observed FFLs was significantly higher on MR imaging compared with CT (Z = −2.36, Wilcoxon signed-rank test, P = .018).
Three of 4 patients with LCH demonstrated prominent soft-tissue components (75%, Fig 1). The 3 patients with LCH who had undergone CT showed sharply marginated bone destruction. None of the patients with LCH showed substantial cystic bone expansion. Two patients with LCH (patients 1 and 7) had a history of minor recent trauma to the lesion before imaging, having hit their head against a fish tank and television remote, respectively. There was no evidence of an abnormal coagulation profile in any of the patients. In patients with ABCs, 2 had primary ABCs and 1 had ABC in the setting of fibrous dysplasia. All patients with ABCs showed bone expansion (Fig 2).

MR imaging in a patient with Langerhans cell histiocytosis. Axial T1- (A) and T2-weighted (B) images reveal multiple FFLs. An enhancing solid soft-tissue component is seen medially on postcontrast axial (C) and coronal (D) T1-weighted images.

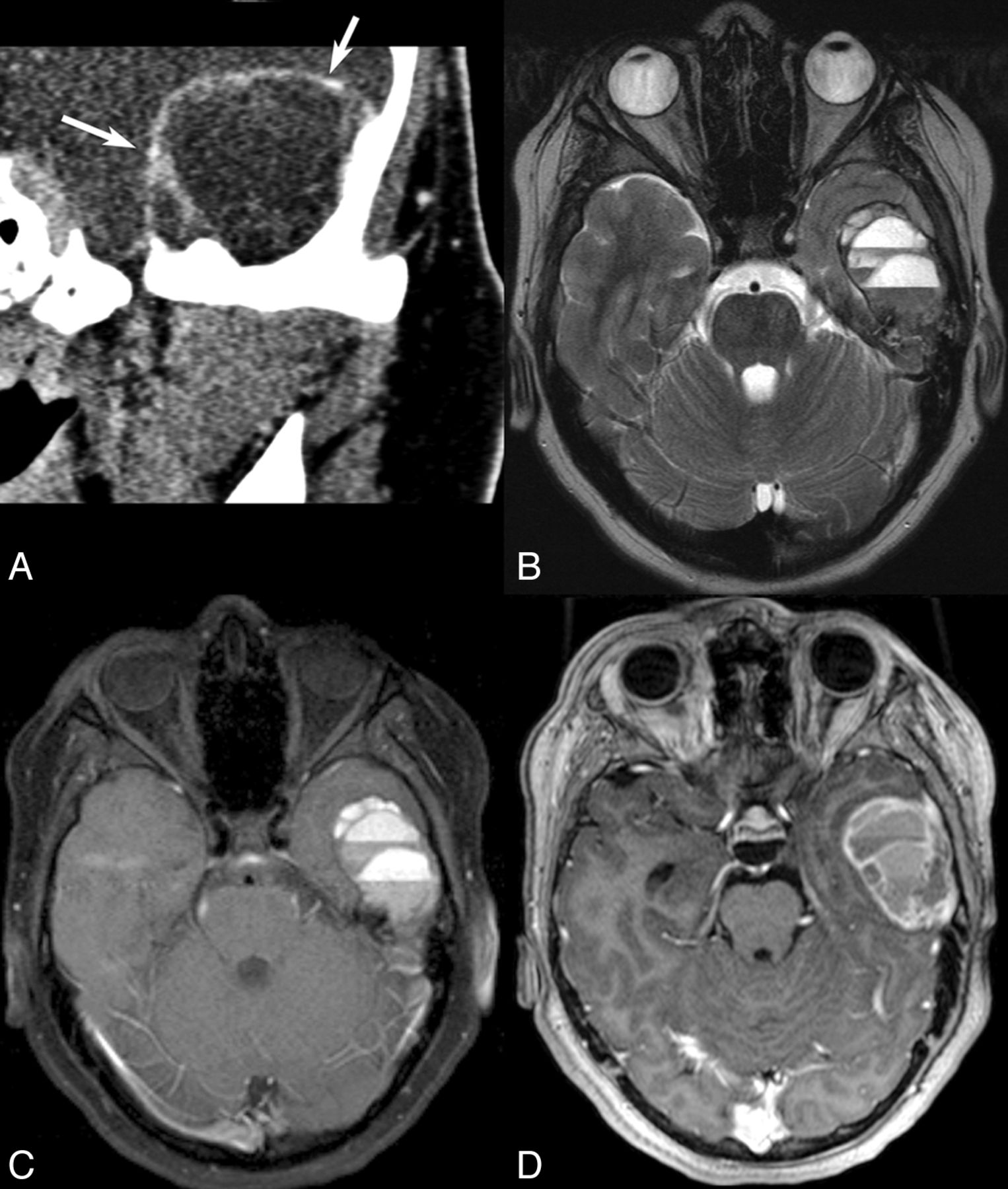
CT and MR imaging findings in a patient with an aneurysmal bone cyst. Coronal CT scan (A) reveals marked bone expansion by a well-defined cystic-appearing mass projecting into the left temporal fossa with very thin remnants of the bony cortex seen in the wall (arrows). T2-weighted (B) and precontrast T1-weighted (C) images reveal multiple FFLs. Peripheral and septal enhancement is noted on CT (A) and postcontrast T1-weighted images (D), but no large enhancing solid soft-tissue component is identified.
All 3 patients with ABCs underwent surgical resection. Among the patients with LCH, 3 underwent surgical resection and 1 (patient 9) underwent chemotherapy after biopsy. Most interesting, follow-up imaging of this latter patient 3.5 months after completion of chemotherapy revealed a considerable increase in the number of FFLs, from 14 to >50 (Fig 3). The 1 patient with metastatic neuroblastoma also underwent treatment with chemotherapy, with a substantial decrease in the size of the lesion (Fig 4). None of the patients with cephalohematoma had a detectable solid or enhancing soft-tissue component at the time of the study, and no frank bone destruction was seen on CT or MR imaging (Fig 5). All patients with cephalohematoma were managed conservatively.

CT and MR imaging findings in a patient with Langerhans cell histiocytosis. Noncontrast CT (A) reveals a lytic lesion with a prominent soft-tissue component and well-defined bone destruction. An FFL is faintly seen (arrow). T2-weighted image (B) and postcontrast T1-weighted image (C) show a few FFLs and enhancement of soft-tissue components, respectively. Axial T2-weighted image (D) following chemotherapy now reveals an increase in the number of FFLs.
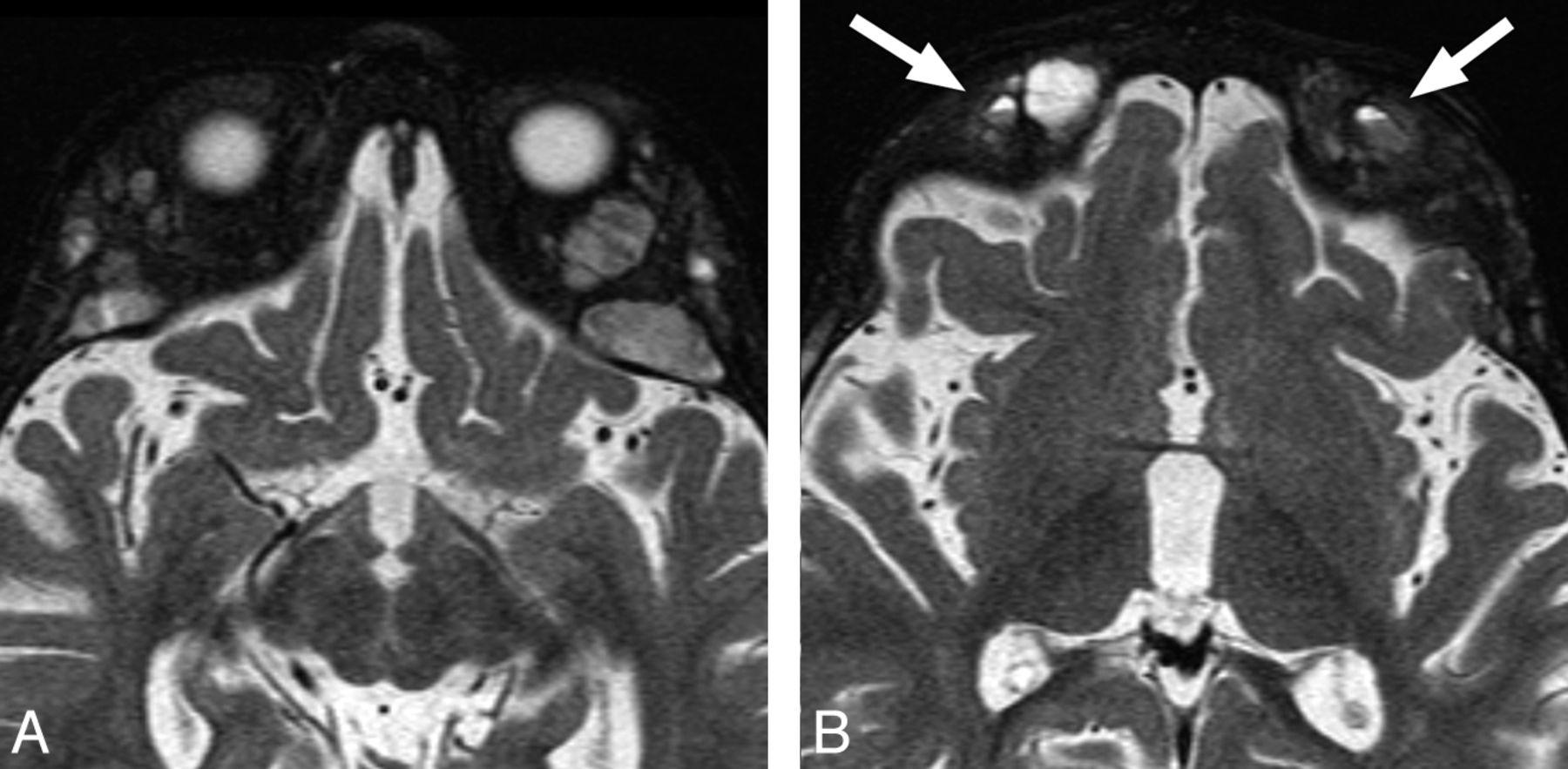
MR imaging findings in a patient with neuroblastoma demonstrate typical bone marrow infiltration and expansion by metastases (A). Multiple small FFLs are seen in the lesions (B).

MR imaging of a 3-month-old patient found to have a bump on the head on physical examination. T2-weighted axial image shows an FFL within a cephalohematoma (arrow), confirmed to be within the bone on multiple planes and sequences (not shown).
Discussion
Generally, a bone lesion with FFLs is considered more likely to represent an ABC; therefore, it was surprising to us that our review of pediatric skull lesions revealed that LCH was the most common etiology of skull lesions with FFLs, followed by ABC. There is no dedicated study on the most common etiology of osseous lesions with FFLs in pediatric patients, to our knowledge. In addition, large studies that may have included some pediatric patients had not published their detailed results based on age groups,5⇓–7 and the current literature is mainly limited to published case reports.9⇓⇓⇓⇓–14
There are only 2 case reports describing the presence of fluid-fluid level in LCH.12,14 In both of these cases, the FFL was demonstrated on both CT and MR imaging. The FFL in LCH represents hemorrhage, which may be triggered by trauma or may be spontaneous hemorrhage. Albadr et al12 reported sudden spontaneous scalp swelling in a patient with LCH of the skull, which was then proved to be secondary to hemorrhage. Chen et al15 reported a patient with LCH of the skull complicated by a spontaneous epidural hematoma. Another potential hypothesis for hemorrhage in LCH is development of aneurysmal bone cyst features, which have been reported to be observed on histology in LCH.16,17 In our patients with LCH, 2 had a history of recent minor trauma, but the other 2 did not. Most interesting, the number of FFLs dramatically increased in 1 patient following chemotherapy (Fig 3), though the overall size of the lesions did decrease. Chemotherapy was used in this patient because there was orbital osseous involvement.18 No evidence of secondary ABC formation was demonstrated on histology in any of the 4 patients with LCH in this study.
We believe that several factors may contribute to the relatively high prevalence of LCH with FFL in this study. First, LCH is relatively more common in the pediatric population compared with adults, and the skull is the most frequently involved site in LCH.19 On the other hand, while ABCs can also occur in young patients, they are most often found in the metaphyses of long bones and rarely affect the skull.3,4,13 Despite the presence of FFLs, we believe that LCH may still potentially be differentiated from ABC on the basis of the presence of characteristic imaging findings such as sharp, nonsclerotic borders with a punched out appearance, lack of demonstrable bone expansion, and uneven destruction of the outer and inner cranial tables with a beveled edge contour on CT, though this may not be possible in all cases. The distinction may be more difficult on MR imaging. Another differentiating feature of LCH can be the presence of a prominent soft-tissue component, which was demonstrated in most of the patients in this study, though occasionally an obvious soft-tissue component may not be present.
ABCs have been reported in many locations, including the orbit, occipital bone, frontal bone, temporal bone, parietal bone, and skull base.20⇓–22 In this study, we found 2 primary ABCs and a secondary ABC in the setting of fibrous dysplasia. The coexistence of an aneurysmal bone cyst and a companion lesion is well-known and is consistent with the concept of local hemodynamic changes secondary to precursor pathology. Trauma, benign lesions of the skeleton (eg, chondroblastoma, chondromyxoid fibroma, osteoblastoma, giant cell tumor, fibrous dysplasia), and even some malignant tumors (eg, osteosarcoma, chondrosarcoma, hemangioendothelioma) have been associated with development of aneurysmal bone cysts.10,17,23 In the setting of fibrous dysplasia, secondary ABC formation can occur in addition to the more common evolving fibrous dysplasia with lytic areas or cystic degeneration.24
Cephalohematoma is a subperiosteal hemorrhage that results from tearing of delicate vessels that traverse through the bone into the scalp. It has been reported in 0.2%–3% of all births,25⇓–27 though most are small and resolve spontaneously. Cephalohematomas are confined to suture borders where the periosteum is tightly adherent to the membranous tissue of the sutures.28 The most common location is over the parietal bone followed by the occipital bone.26
Multiple risk factors have been associated with the development of cephalohematoma, including birth trauma, fetal scalp monitors, instrumentation, greater birth weight, and nulliparity.25,29,30 Cephalohematoma is a benign condition, which usually does not require specific therapy. Most cephalohematomas resolve within a few weeks to months, depending on their size.29,31 Many patients with typical history and clinical examination for cephalohematoma will not be imaged. On the infrequent occasion when the hematoma fails to resorb, progressive subpericranial osteogenesis results in a calcified cephalohematoma. The incidence of calcification has been reported to occur in 3%–5% of all cephalohematomas.32 In these cases, there is usually a history of a mass present since birth that is initially boggy and fluctuant and then gradually hardens, typical of an ossifying cephalohematoma.31 In this series, we found 3 cases of cephalohematoma, one in a neonate, another in a young infant, and the other, a partially calcified cephalohematoma, in a 10-year-old patient. All of the lesions were in the parietal area, which is consistent with findings in the literature.26
Neuroblastoma is the most common extracranial solid tumor. Metastatic involvement of the head and neck is common and manifests most often as osseous metastases with periosteal reactions involving the calvaria, orbit, or skull base33,34 and is also commonly seen both at presentation and at the time of tumor recurrence. One of the patients in this study had metastatic neuroblastoma involving the sphenoid bone. We are not aware of any report in the English literature describing FFLs in metastatic neuroblastoma to the skull.
The main limitation of our study is the relatively small number of patients, though there has been no focused study of osseous lesions of the skull with FFL, particularly in pediatric patients. Future larger studies may shed more light on the various etiologies of these lesions.
Conclusions
Radiologists should be aware that besides ABCs, there are other lesions in the pediatric skull that can demonstrate FFLs. In our series, LCH was the most common etiology followed by ABC. Cephalohematoma should also be considered in the appropriate clinical setting. As would be expected, MR imaging was more sensitive in detecting FFLs within the lesions.
REFERENCES
- Received May 10, 2013.
- Accepted after revision June 20, 2013.
- © 2014 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}