
Abstract
Summary: A percutaneous technique for visualizing sacral nerve roots is described. A fiberscope was inserted into the subarachnoid space through a sheath that was inserted via a percutaneous lumbar puncture. The sacral nerve roots were identified with endoscopic visualization and x-ray fluoroscopy localization of the endoscope. These images were compared with those obtained from a videoscope, which revealed better imaging. Specific sacral nerve roots can be identified by using a combination of endoscopy and x-ray fluoroscopy. This technique may enable minimally invasive interventions such as lysis of adhesions, arachnoid cyst decompression, selective dorsal rhizotomy, and more selective and precise nerve stimulation electrode placement.
A percutaneous technique for visualizing and identifying sacral nerve roots based on combined fluoroscopic and endoscopic imaging is presented and the image quality of a fiberscope is compared with that of a videoscope. Previous studies have shown that percutaneous intraspinal navigation (PIN) is technically feasible (1) and that spinal endoscopy is capable of visualizing spinal cord anatomy (1–5). In these studies, the endoscope was inserted at the level of the lumbar spine and directed cephalad; therefore, the lumbosacral roots as they exit the canal were not identified. This technique may provide a minimally invasive technique for spinal interventions such as dorsal rhizotomy, selective neural stimulation, and potential future applications involving stem cell transplantation and thus may reduce the morbidity associated with laminectomy and open surgical exposure.
Description of the Technique
Two unembalmed male cadavers were obtained from our Institutional Willed Body Program and transported to our research angiography suite (Infinix VC-i, Toshiba, Tokyo, Japan) and placed in the prone position. Lumbar puncture with an 18-gauge single-wall puncture angiography needle was performed under fluoroscopic guidance at the L3–4 interspace in one of the cadavers. A 0.038-inch guidewire was introduced and directed caudally. The tract was serially dilated with 5F, 8F, 10F, and 12F dilators, and a 12F Cook arterial sheath was inserted in the subarachnoid space with its tip directed caudally. The subarachnoid space was inflated with an infusion of normal saline.
A 3.3-mm outer diameter (OD) Olympus (Tokyo, Japan) fiberscope with a 1.2 mm working channel was advanced over a guidewire through the sheath under x-ray fluoroscopy. The endoscope had a field of view of 120°, a depth of field of 3–50 mm, and tip deflection of 180° up to 130° down. The endoscope was advanced caudally under endoscopic navigation, and its position relative to the bony spine was determined with x-ray fluoroscopy in the posteroanterior (PA) and lateral projections. Endoscopic images were captured with a digital image capture device (Olympus OTV-S7V-B). Nerve roots were grasped and manipulated with 1-mm flexible forceps.
In the second cadaver, an L2 laminectomy was performed through a 4–5 cm midline incision. The dura was incised and a 5-mm OD Olympus videoscope was inserted into the intrathecal space and directed caudally. The videoscope had a 2.2-mm working channel, a field of view of 120°, a depth of field of 3–50 mm, and tip deflection of 210° up to 120° down (Fig 1).

Photograph of the 5 mm Olympus videoscope used for this study.
There was some difficulty in placing the 12F sheath in the first cadaver due to its size; however, the 3.3-mm OD fiberscope was able to be advanced with relative ease through the sheath to the termination of the thecal sac, though there was some difficulty in torquing the fiberscope. The sacral nerve roots and the filum terminale were visualized as they coursed caudally and as they exited the thecal sac (Fig 2 and Video Clip 1). The distal end of the fiberscope was easily identified on x-ray fluoroscopy and enabled confirmation on the fiberscope position (Figs. 3A and 4A). Visualization of anatomical structures improved as the fiberscope was advanced further caudally due primarily to the increased CSF-filled free space within the thecal sac as the nerve roots exited. Individual dorsal and ventral nerve roots, along with their surface features such as blood vessels, were readily distinguished. The ability to visualize and to navigate to specific nerve roots was greatly enhanced by the fiberscope’s tip deflection, which allowed a close-up look at individual nerve roots as they exited (Fig 3B and Video Clip 2). The tip deflection also allowed us to pan across the thecal sac, thus effectively increasing the fiberscope’s field of view. With X-ray fluoroscopy, the position of the fiberscope’s distal tip relative to the bony spine could be determined. This allowed us to identify which nerve root we were visualizing. The nerve roots were also grasped and manipulated with 1-mm forceps that were introduced through the working channel (Figs 4B, -C and Video Clip 3).

Still-frame image from the fiberscope of the terminal thecal sac.

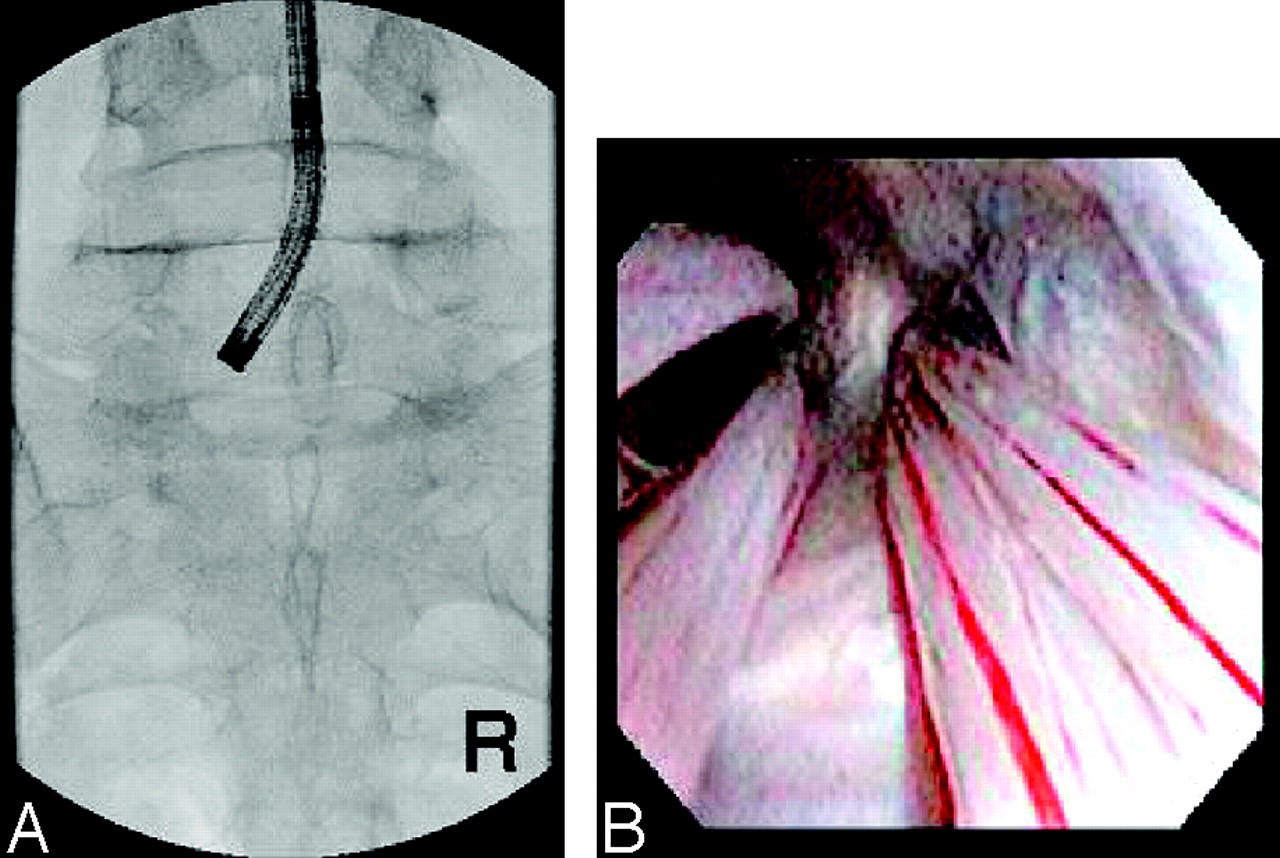
A, AP x-ray of the lumbar spine. The fiberscope, which is being directed to the left S1 nerve root, is seen.
B, Still-frame image from the fiberscope of the left S1 nerve root.

A, AP x-ray of the sacrum while a nerve root is being grasped and manipulated with flexible forceps.
B, Still-frame image from the fiberscope of a nerve root being grasped and manipulated with flexible forceps.
C, Still-frame image from the fiberscope of a nerve root being grasped and manipulated with flexible forceps.
The 5-mm videoscope was inserted into the intrathecal space under direct vision and advanced caudally with relative ease. The videoscope was easily identified under x-ray fluoroscopy and enabled the position of the videoscope to be determined (Figs 5A and 6A). The sacral nerve roots, filum terminale, and arachnoid trabeculations were visualized in fine detail. The videoscope provided a large field of view, which enabled most anatomical structures to be seen (Fig 5B and Video Clip 4). The tip of the videoscope could be easily deflected, and this enabled the videoscope to be navigated to specific structures to be visualized. The dorsal and ventral portions of the left S1 nerve root were visualized as they exited the thecal sac (Figs 6B–D) and multiple nerve roots are seen on Video Clip 5. Surface features such as small blood vessels were readily identified. The videoscope was easily torqued, which also aided in navigation. Individual nerve roots were easily grasped and manipulated with forceps (Figs 7A, -B and Video Clip 6).

A, AP x-ray of the lumbar spine and sacrum seen along the midline with the videoscope.
B, Still-frame image from the videoscope of several sacral nerve roots.
C, Still-frame image from the videoscope of several sacral nerve roots just before exiting the dura and the filum terminale (labeled with an asterisk).
D, Still-frame image from the videoscope at the terminal thecal sac. The filum terminale is labeled with an asterisk.
A, AP x-ray of the lumbar spine. The fiberscope, which is being directed to the left S1 nerve root, is seen.
B, Still-frame image from the fiberscope of the left S1 nerve root.

Still-frame images from the videoscope of a nerve root being grasped and manipulated with flexible forceps.
Discussion
Other authors have described methods and techniques for endoscopic visualization of intrathecal structures based solely on fiberscopes. Eguchi et al (2) reported the use of 3 fiberscopes (0.5-, 1.4-, and 2.2-mm OD) for the examination of the spinal cord and posterior fossa anatomy in 5 cadavers and in 7 patients. The fiberscopes were introduced into the subarachnoid space at the L4–5 level via a percutaneous approach and then were advanced rostrally. No attempt at visualizing the sacral nerve roots was noted, nor was there mention of using fluoroscopy along with endoscopy to identify specific nerve roots. The cauda equina, nerve roots, surface of the spinal cord, and blood vessels were visualized. Subsequent to the cadaver studies, Eguchi et al (3) used spinal cord endoscopy in 7 patients with various spinal disorders (spinal cord herniation through a dural defect, syringomyelia, spinal arachnoid cyst, and a spinal epidural cyst). A 0.5-mm OD fiberscope inside a 4F angiography catheter was inserted via a lumbar puncture at L4–5 and advanced cranially. No complications were noted; however, the need for improvements in manipulating the fiberscope was noted. Preoperative endoscopy provided useful morphologic information helpful in diagnosis and surgical planning. Intraoperative endoscopy enabled areas outside the operative field of view to be visualized as well as cord perfusion. No endoscopic interventions were employed.
Using a similar technique of insertion via a lumbar puncture and advancement cranially, Uchiyama et al (4) reported using a fiberscope to evaluate spinal cord pathology in 18 patients with either back pain and/or neurologic symptoms in which the diagnosis was uncertain. In 11 of the 18 cases abnormal findings such as adhesions or fibrous masses were identified. As in the case of Eguchi et al no endoscopic interventions were employed. No postprocedure nerve or spinal cord injuries were noted; however, there was 1 case of meningitis and 5 cases of postspinal headache.
Warnke et al (6–8) reported using endoscopy to visualize the structures in the lumbar intrathecal sac in both cadavers and in patients with spinal disorders. A 2.5-mm OD steerable fiberscope with 2 working channels was used to assess the etiology of back pain in 12 patients, 3 with MR findings (spinal arachnoid cyst, intraspinal meningocele, and prefixed filum terminale) and 9 with no radiographic explanation for the pain. The fiberscope was introduced at the L1–2 level through a minimally invasive open surgical incision that required a laminectomy. In the cases where the preprocedural diagnosis was known, the pathology was identified and was treated in 2 of the 3 cases (arachnoid cyst partial resection and transection of the prefixed filum terminale). Varying degrees of arachnoiditis around nerve rootlets were diagnosed in the 9 patients with back pain of unknown etiology. The inflamed arachnoid was dissected away, and 4 patients experienced complete pain relief that did not recur for 6 months. The other 5 patients experienced a 40% reduction in pain. All clinical cases were performed without evidence of postprocedural neurologic deficits. Six patients experienced postprocedural headaches.
The growth in minimally invasive spine surgery has been spurred by both technical advances and by its associated reduction in operative morbidity. However, minimally invasive techniques are primarily employed in extradural procedures, while intradural procedures such as dorsal root rhizotomy require open, multilevel laminectomies. The advances in endoscopic imaging and the capability of miniaturizing instruments enable intradural procedures to be potentially performed by using minimally invasive techniques.
With the fiberscope, nerve roots and other structures could be readily identified; however, with the videoscope the level of resolution was much greater (2, 3). This higher degree of resolution (seen in Figs 5B-D, Fig 6B, Figs 7A, -B and Video Clips 4–6) is directly related to the superior imaging of a videoscope relative to that of a fiberscope and enabled navigation and manipulation of structures to be performed with a greater degree of confidence. Also, the ability to deflect the tip of the endoscope and the ability to torque the endoscope were very critical in being able to successfully navigate within the subarachnoid space. Another benefit of the videoscope was its added robustness, because the images are transmitted via electrical wires versus fiberoptics. This gave the endoscope greater flexibility, which enabled the endoscope to make the roughly 90° turn immediately after entering the subarachnoid space. Also, the problem of breaking the optical fibers when trying to manipulate the endoscope, which we have found to be a significant problem, is avoided with the use of the videoscope.
The combined use of endoscopy and fluoroscopy proved to be very helpful in identifying specific structures and will be necessary in clinical applications. Similarity in appearance between nerve roots makes specification of levels difficult by using purely endoscopy, but it is easy when combined with fluoroscopic visualization at the level of the imaging apparatus. This multimodal imaging approach enabled specific nerve roots to be identified and thus provided a minimally invasive approach to current open surgical intradural procedures, such as selective dorsal rhizotomy.
Numerous conditions, including spasticity, lumbar and sacral neuralgia, and bladder and fecal incontinence, are related to spinal cord and lumbar and sacral nerve root pathology. Surgical approaches to these structures currently involve open surgery, including removal of varying amounts of spinal bone. In an effort to reduce the morbidity and mortality of these procedures, less invasive methods are being explored via this PIN technique. Specifically, implantable electrodes that can be delivered to portion of a nerve root via the working channel of the endoscope are being investigated. Also, nerve root ablation and fibrous tissue removal with a laser fiber introduced through the working channel are being explored. Further miniaturization of the videoscope should enable it to be introduced percutaneously. Additional studies are necessary to determine the safety and the techniques and devices necessary to perform specific intradural applications by using this approach. This approach is still in the experimental stages and is considered off-label use.
Footnotes
↵V The online version of this article contains supplemental videos at http://www.ajnr.org.
- Received March 25, 2005.
- Accepted after revision April 28, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}