
Abstract
BACKGROUND AND PURPOSE: Flow diversion is being increasingly used to treat bifurcation aneurysms. Empiric approaches have generally led to encouraging results, and a growing body of animal and ex vivo literature addresses the fate of target aneurysms and covered branches. Our prior investigations highlighted the dynamic nature of metal coverage provided by the Pipeline Embolization Device and suggested strategies for creating optimal single and multidevice constructs. We now address the geometric and hemodynamic aspects of jailing branch vessels and neighboring target aneurysms.
MATERIALS AND METHODS: Fundamental electric and fluid dynamics principles were applied to generate equations describing the relationships between changes in flow and the degree of vessel coverage in settings of variable collateral support to the jailed territory. Given the high complexity of baseline and posttreatment fluid dynamics, in vivo, we studied a simplified hypothetic system with minimum assumptions to generate the most conservative outcomes.
RESULTS: In the acute setting, Pipeline Embolization Devices modify flow in covered branches, principally dependent on the amount of coverage, the efficiency of collateral support, and intrinsic resistance of the covered parenchymal territory. Up to 30% metal coverage of any branch territory is very likely to be well-tolerated regardless of device or artery size or the availability of immediate collateral support, provided, however, that no acute thrombus forms to further reduce jailed territory perfusion.
CONCLUSIONS: Basic hemodynamic principles support the safety of branch coverage during aneurysm treatment with the Pipeline Embolization Device. Rational strategies to build bifurcation constructs are feasible.
ABBREVIATIONS:
- FD
- flow diverter
- PcomA
- posterior communicating artery
- PED
- Pipeline Embolization Device
Flow-diversion therapy, exemplified by the Pipeline Embolization Device (PED; Medtronic, Dublin, Ireland) in the United States >7 years after its FDA approval based on results of the Pipeline for Uncoilable or Failed Aneurysms (PUFS) trial,1 has revolutionized the treatment of brain aneurysms. Subsequently, PUFS results at 32 and 53 years demonstrated both the durability and, uniquely, increasing efficacy of treatment over time. However, in a widely known trend and a matter of increasing concern, most aneurysms now treated with the PED fall outside the population of adults with large or giant wide-neck intracranial aneurysms in the internal carotid artery from the petrous to the superior hypophyseal segments4⇓–6 for which the device is indicated. Among these outside-of-indication targets, most appear to be <10-mm aneurysms located in the same petrous-to-posterior communicating artery range. However, both in the United States and, more commonly, abroad, the PED and other flow diverters (FDs) are being used to treat more distal aneurysms, including those affecting the MCA bifurcation,7 anterior communicating artery,8 posterior communicating artery (PcomA) segments (including in the setting of “fetal PcomA”9), distal anterior cerebral artery,10 and others.6,11,12 While reasons for these trends are complex and multifactorial, published results have been generally encouraging,7,8,11,12 with a few groups reporting a high burden of ischemic complications.13,14
The mechanisms responsible for efficiency of flow diversion in aneurysm treatment have been well-described.15 Likewise, rational approaches to building both single- and multidevice16 constructs that maximize desired metal coverage of the aneurysm while minimizing coverage of adjacent perforator and other hazards have been outlined both by our group and others.17,18 The fates of some covered branches, such as the ophthalmic,19 anterior choroidal,20 and posterior communicating9 arteries have been extensively examined, highlighting the critical role of collateral support in determining the long-term patency of covered branches. The unifying message is that good collaterals frequently lead to progressive occlusion of jailed branches, both in humans and in specifically designed animal models.17⇓⇓–20 Unfortunately, quantifying the efficiency of collateral support at a given time point and estimating its subsequent change are extremely difficult. Likewise, the study of hemodynamic changes in aneurysms and adjacent covered branches is made difficult by the daunting complexity of in vivo fluid dynamics.21 Nevertheless, because flow diversion is being increasingly used, essentially on an empiric basis, in settings that require jailing branches of both substantial size and eloquence such as M2 segment divisions, some rational consideration of the immediate hemodynamic consequences of treatment is required.
To this end, we have considered a mathematic description of a simplified flow system based on an electric circuit analogy and fundamental fluid dynamics. The electric circuit analogy has a history of application in cerebrovascular pathology, including AVMs by Guglielmi22 and cervical carotid disease by Spencer and Reid.23 The disadvantage is that electric currents do not behave in ways fully analogous to even idealized fluids and that, ultimately, to study fluid flow, we have to rely on fluid equations. However, even the simplest fluid systems are affected by many variables related to the nature and flow dynamics of fluid and flow channel morphology. When applied to fluids of blood complexity, in systems of complex pulsatile flow, and further modified by various feedback mechanisms that biologic systems bring to play once homeostasis is modified by changes such as FD implantation, it is easy, indeed, to recognize our limits of understanding. It is important to appreciate these humbling limits. While computational and other advances may someday allow solutions to systems of such complexity, we thought that an alternative approach of describing a basic system with minimal assumptions, designed to produce the most conservative outcomes, would be useful in defining conservative limits of flow changes in states of branch coverage.
Materials and Methods
Electric circuits were modeled to illustrate the effects of jailing a branch vessel with variable metal coverage under conditions of variable collateral support to the compromised vascular territory. The efficiency of the collateral network or networks was defined relative to the primary supplying branch, as a ratio of collateral pathway to primary pathway flow resistance. Variable resistance of the parenchymal territory (classically defined according to the Ohm law as a ratio of territory perfusion pressure to its flow24,25) supplied by the covered branch was also considered. The relative change in the amount of flow to the downstream brain territory as a function of the % metal coverage was calculated for systems over a complete range of collateral support. Flow relationships were based on the conservative assumption of flow change proportionality to the second power of the channel cross-sectional area, in contrast to the linear relationship in electric circuits. Likewise, feedback effects of biologic systems, which act to minimize flow changes by mechanisms that include vasodilation and hypertension, were ignored to produce the simplest and most conservative outcomes.
The circuit analogy to the biologic system exemplified by a middle cerebral artery aneurysm is shown in Fig 1. The circuit consists of a primary pathway with resistance, r, and a secondary/collateral pathway or pathways with a sum total resistance, R, together supplying the brain parenchyma, which has its own resistance, Rbrain. In this circuit the total resistance is
 The effect of FD placement (for example from M1 to the inferior division of M2 in Fig 1) is to increase r (resistance in the covered superior division branch). The degree to which r increases corresponds to the second power of change in the cross-sectional area A of covered branch, expressed as
The effect of FD placement (for example from M1 to the inferior division of M2 in Fig 1) is to increase r (resistance in the covered superior division branch). The degree to which r increases corresponds to the second power of change in the cross-sectional area A of covered branch, expressed as
 where p is porosity, ranging from 0 to 1 (% Metal Coverage = 1/p × 100%). Thus, the change in r following FD placement is proportional to r/p2. Therefore, total resistance post–flow diverter placement is
where p is porosity, ranging from 0 to 1 (% Metal Coverage = 1/p × 100%). Thus, the change in r following FD placement is proportional to r/p2. Therefore, total resistance post–flow diverter placement is
 Because flow, I, is inversely related to resistance according to the Ohm law, I = V/R (V is voltage in electric circuits and fluid pressure, such as blood pressure, in fluid systems), for a constant V (no change in perfusion pressure), the fractional change, ΔI, in blood flow through the brain subserved by the jailed branch may be stated as
Because flow, I, is inversely related to resistance according to the Ohm law, I = V/R (V is voltage in electric circuits and fluid pressure, such as blood pressure, in fluid systems), for a constant V (no change in perfusion pressure), the fractional change, ΔI, in blood flow through the brain subserved by the jailed branch may be stated as
 This equation can be simplified if Rbrain = 0 (the most unforgiving and conservative assumption if we consider the effects of decreasing porosity on total blood flow)—the greater Rbrain becomes, the less change in total flow is affected by decreasing p. If Rbrain = 0, then I at point P after flow-diverter implantation of porosity p is
This equation can be simplified if Rbrain = 0 (the most unforgiving and conservative assumption if we consider the effects of decreasing porosity on total blood flow)—the greater Rbrain becomes, the less change in total flow is affected by decreasing p. If Rbrain = 0, then I at point P after flow-diverter implantation of porosity p is
 Thus, fractional flow change after device implantation compared with pre-FD deployment (p = 1) is
Thus, fractional flow change after device implantation compared with pre-FD deployment (p = 1) is
 Thus, ΔI is dependent on a ratio of r/R rather than absolute values of r and R.
Thus, ΔI is dependent on a ratio of r/R rather than absolute values of r and R.

Schematic illustration of the electric circuit analogy for a bifurcation aneurysm. In this MCA example, implantation of a flow diverter from M1 to the inferior division of M2 results in jailing of the superior division, which is the main source of supply to its brain territory, with a flow resistance r (the effect of implanting a flow diverter is to increase r by reducing the M2 cross-sectional area in proportion to the amount of metal coverage). The collateral circuit to the same brain territory, in this example the anterior cerebral artery–MCA leptomeningeal collaterals, is associated with a combined resistance R. The brain parenchyma supplied by this circuit has its own resistance, Rbrain. These constitute parallel circuits, with downstream resistance Rtotal at point P. FD treatment of any branch point aneurysm can be described by this model.
In the extreme example of no collateral (R = ∞),
 Therefore, when P = 1 (no FD), there is no change in I. When P = .5 (50% coverage), there is 0.52 = ¼ of baseline flow present.
Therefore, when P = 1 (no FD), there is no change in I. When P = .5 (50% coverage), there is 0.52 = ¼ of baseline flow present.
At the other extreme of perfect collateral with R → 0, ΔI = 1 (no flow change) regardless of p.
Most important, in this model, flow in the covered branch is independent of collateral status (as in any parallel circuit, flow in each parallel circuit component is independent and is only dictated by voltage and the individual resistance of the circuits).
Results
Figure 2 shows application of this model to 3 types of PcomA aneurysms that correspond to the above extremes of R = ∞ (fetal PcomA), R = 0 (no PcomA), and r = R (balanced PcomA and P1).

Schematic illustration of circuit model application to 3 types of PcomA aneurysms. A, Equally well-developed P1 and PcomA segments, where R = r. B, Fetal PcomA configuration where R≫r (negligible collateral support by a hypoplastic P1 segment). C, Dominant P1 segment with a hypoplastic PcomA segment, corresponding to R≪r.
Figure 3 shows various aneurysms and corresponding R:r relationships. In the hypothetic MCA aneurysm with more effective MCA–anterior cerebral artery leptomeningeal collaterals compared with MCA–posterior cerebral artery collaterals, the flow diverter is implanted in the inferior division to take advantage of more effective anterior cerebral artery–MCA collaterals. This approach is not rigid; in a nondominant hemisphere, it might be preferable to jail the inferior division regardless of its collateral status.

Schematic illustration of various branch aneurysms and associated primary and collateral pathway efficiencies, demonstrating the applicability of the parallel circuit model to different branch aneurysm configurations. In this figure, for example, MCA–posterior cerebral artery leptomeningeal collaterals are less efficient than MCA–anterior cerebral artery collaterals, prompting implantation of an FD into the inferior division, which has less collateral support. For an anterior communicating artery aneurysm with well-developed A1 and A2 segments bilaterally, an H-type FD treatment would correspond to a high value of R.
Figure 4 shows the relationship of fractional flow, ΔI, to % metal coverage for a variety of more-or-less effective collaterals. An extensive literature review of studies establishing human cerebral ischemia thresholds by Baron24 suggests that a 60% flow reduction (0.4 fractional flow) represents a reasonable ischemic threshold; a more conservative fraction can be adopted on the basis of the individual comfort level. On the x-axis, based on our prior work,26 implantation of a single PED, depending on the relative size of the device to the parent artery, results in a range of % metal coverage between ∼18% and 35%. Thus, according to Fig 4, placement of a single PED will not result in >50% reduction in branch flow and is, thus, unlikely to produce ischemia. For multiple overlapping PEDs, the resultant % metal coverage can also be acceptable; however, this approach requires attention to individual porosities. Tables of these relationships are available.16

Fractional flow change as function of % metal coverage following FD implantation for a range of collateral circuit efficiencies. The ratio of r:R represents a primary-to-collateral circuit relative resistance, with higher r:R values corresponding to increasingly efficient support. In the extreme example of R = 0, flow into the parenchymal territory remains unchanged regardless of metal coverage. At the other extreme of R = ∞ (no collaterals), flow falls to zero at 100% metal coverage. The classic ischemia threshold is set at 0.4 (60% flow reduction). A range of % device metal coverage for the single- and double-coverage PED is provided. According to this model, single-device coverage is extremely unlikely to precipitate ischemia unless followed by acute thrombosis.
The above model is highly conservative because it forbids a number of realistic and often highly effective in vivo adoptive changes,27 all of which are directed at minimizing ΔI following FD implantation. These include adaptive hypertension, vasodilation in both primary and collateral circuits (decrease in R, Rbrain, and r), and, most important, long-term increases in collateral efficiency (further drop in R). As explained above, it also assumes that in the jailed territory Rbrain = 0, which is the most unfavorable situation. For example, Fig 5 shows the effects of increasing Rbrain in a disposition with unfavorable collaterals (R:r = 10:1); here, increasing Rbrain results in progressively less change in flow, ΔI, for all values of % metal coverage. When collaterals are “good” (R:r = 2:1), increasing Rbrain allows the brain to tolerate significantly higher degrees of metal coverage. For all the above reasons, the practical limit of safe % metal coverage is likely to be >30%. Furthermore, on the basis of known PED size/coverage relationships,26 as well as of in vivo experience,28 single PED coverage is likely to remain below 30%.
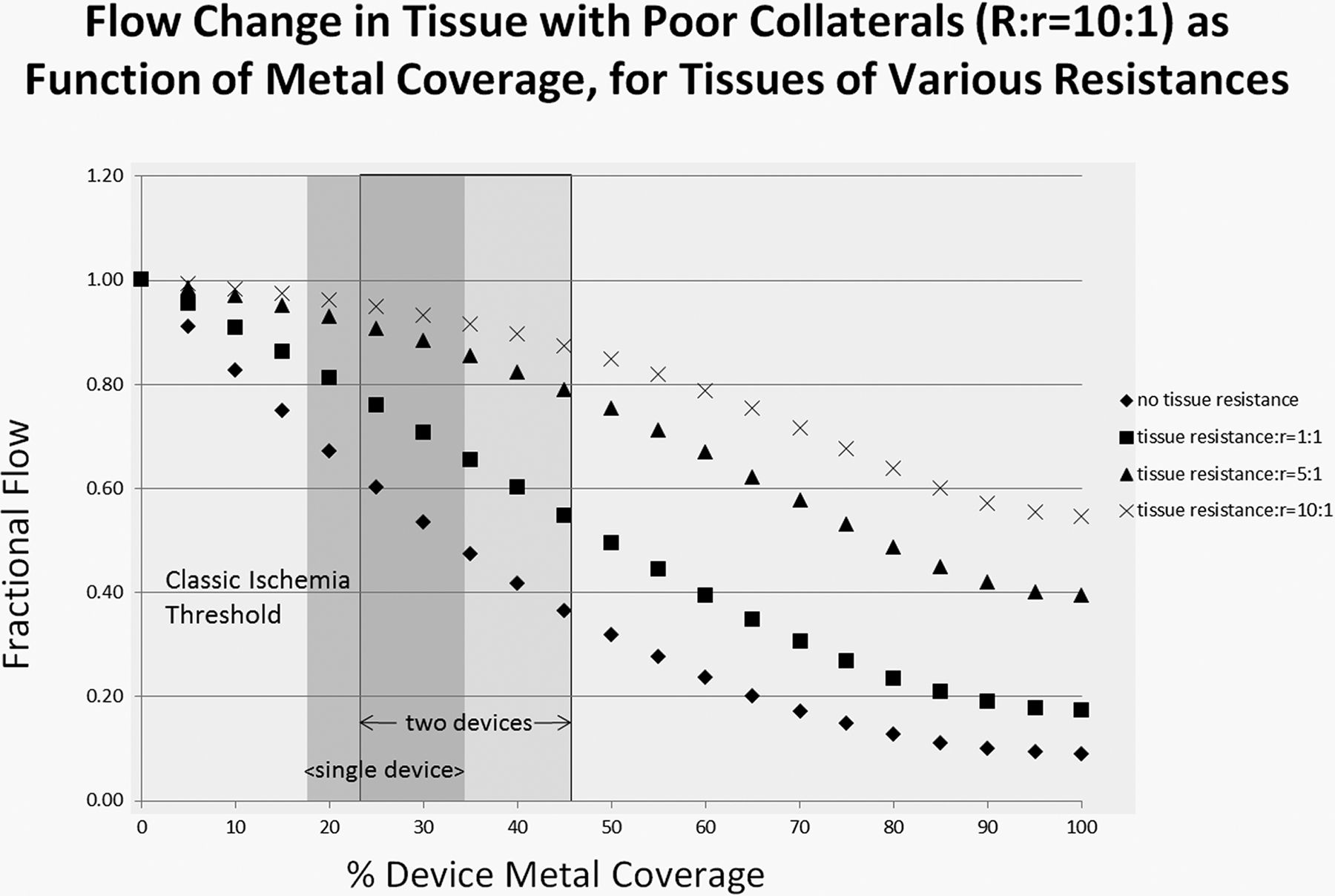
Fractional change in flow under conditions of varied brain parenchymal resistance for tissue with poor collaterals (R:r = 10:1). The actual value of brain resistance is both difficult to determine and variable but, under all circumstances, is greater than zero. It is probably comparable with large-artery flow resistance (tissue resistance: r = 1:1) according to Faraci and Heistad.25 These functions illustrate that jailing territories of higher parenchymal resistance leads to less change in perfusion than jailing territories of lower resistance.
Discussion
The above model is consistent with most published bifurcation aneurysm FD treatment experience.29 In the largest to date MCA experience by Iosif et al,7 the low incidence of ischemic complications was attributed by the authors to careful antiplatelet management and preferential use of a single, slightly oversized flow diverter to minimize metal coverage. Both conditions are consistent with our calculations. Beyond our rigid model, long-term biologic adaptations tend to promote growth of collaterals when available, leading to eventual occlusion of covered branches, which likely proceeds after the reduction in demand for flow through the branch is followed by gradual endothelial overgrowth; this progressive occlusion has been consistently found by multiple groups in various settings to be overwhelmingly asymptomatic.5,7,9,11,12,29,30 Furthermore, predictable enlargement of collaterals can be part of a staged treatment strategy. When collaterals are not readily available, as may be expected in a number of MCA bifurcation situations for example, covered branches tend to remain patent.27 What remains unpredictable, at least in our experience, is why, under conditions of continued branch patency, the associated aneurysm sometimes disappears and sometimes does not. There is evidence to suggest that collateral circulation continues to evolve well beyond the typical 12-month posttreatment efficacy benchmark, contributing to progressive occlusion of branch-associated aneurysms.30 Recent advances in the development of less thrombogenic implants such as the Pipeline Shield (Medtronic) may further improve the safety profile of bifurcation aneurysm treatment by establishing a less thrombogenic environment,31 though this hypothesis remains unproven.
The one critical condition on which patency of any covered branch depends is that flow-diverter implantation not precipitate acute thrombosis (further increase in r beyond r/p2 resulting from FD placement). This is an intuitive and inflexible condition that, in practice, demands strict antiplatelet monitoring. Indeed, reports of high ischemic complications in bifurcation aneurysm treatment with flow diverters illustrate proved instances of acute thrombosis-related occlusions.13
Study Limitations
Already acknowledged above are many limitations of our model, which favors simplicity and conservative assumptions. We have relied on well-established equations rather than creating a physical flow model to test our conclusions. The realities of in vivo fluid systems are infinitely more complex; however, we believe that these are also likely to be more forgiving. Indeed, animal model data support both continued patency and essentially unchanged flow rates in covered branches without adequate collateral support, a situation that requires significant adaptive changes.27 Quantifying efficiency of collateral support remains difficult. Parenchymal resistance, Rbrain, is both variable and difficult to estimate; however, to the extent that it is always greater than zero, increasing parenchymal resistance permits increasing metal coverage. One of the consequences of assuming Rbrain = 0 is likely unphysiologically high blood pressure drops across jailed branches. However, to the extent that this is an unforgiving consequence of our model, lesser pressure drops are likely to be better tolerated. We did not discuss the effects of global hypotension; the mathematics of this change in our model is straightforward, and global hypotension is an undesirable event anytime. The model ignores all aspects of implant and jailed branch geometry and nonzero thickness of the implant (braid diameter ∼ 30 μm). Both R and r are treated in a relative manner. Finally, our model only deals with branch coverage safety and does not address treatment efficacy. It is not directly related to a growing body of increasingly sophisticated computational flow dynamics knowledge. Finally, returning to our early point, treatment of bifurcation aneurysms currently remains outside PED indications, at least in the United States. We believe that its safety and efficacy in this setting should be subjected to a prospective controlled trial, guided by principles established in this and related articles, animal models, and already existing encouraging human experience.
Conclusions
Basic principles of fluid mechanics support the safety of Pipeline Embolization Device use in bifurcation aneurysms. Lack of acute thrombus formation is a key precondition. Therefore, careful attention to antiplatelet coverage is essential.
Footnotes
Disclosures: Maksim Shapiro—RELATED: Consultancy: Medtronic, Comments: I am a consultant and Pipeline Embolization Device proctor for Medtronic. Eytan Raz—UNRELATED: Consultancy: Medtronic; Royalties: Springer; Stock/Stock Options: Penumbra; Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: Medtronic, MicroVention. Peter K. Nelson—RELATED: Consulting Fee or Honorarium: Medtronic, Comments: Clinical proctor.
References
- Received June 10, 2018.
- Accepted after revision September 28, 2018.
- © 2018 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}