
Abstract
SUMMARY: Symptomatic Rathke cleft cysts (RCC) are reported in the sellar and suprasellar regions, but no case of sphenoidal RCC has been reported. We report a case of sphenoidal RCC in a 41-year-old man. The lesion was revealed by headaches and diplopia. Symptoms disappeared transiently after a spontaneous rhinorrhea but relapsed 4 months later. MR imaging showed a cystic sphenoidal lesion, isointense on T1-weighted images (WI) with peripheral gadolinium enhancement and hyperintense on T2 WI. The patient underwent surgery through a transrhinoseptal approach. The wall of the sphenoid sinus was paper-thin. The cyst contained a motor-oil-like fluid and communicated widely with the nasal fossa. Its wall was partially extracted. Symptoms and signs ceased after surgery. MR imaging performed 1 year later showed the disappearance of the sphenoidal cyst. Embryological origin of RCCs is discussed. The hypothesis of a continuum between the different epithelial cystic lesions of the sellar and parasellar region is discussed. Imaging has an important impact on the diagnosis; nevertheless, the specific characterization remains difficult.
Rathke cleft cysts (RCC) are typically described as benign epithelium-lined intrasellar cysts containing mucoid material. They are believed to originate from remnants of Rathke pouch.1 These cysts are frequently small and asymptomatic. They are encountered in 12%–33% of normal pituitary glands in routine autopsies.2 RCC are typically intrasellar or intrasellar and suprasellar, rarely limited to the suprasellar region.2–7 They may become large enough to cause symptoms by compression of the adjacent structures. No case of sphenoidal RCC has been reported.
Case Report
A 41-year-old man presented in August 2002 with progressive headaches, ptosis, and diplopia. In November 2002, he had a spontaneous rhinorrhea followed by complete resolution of the symptoms. In February 2003, the frontal headaches relapsed, associated this time with a progressive decrease in the visual acuity of the left eye.
On clinical examination in April 2003, the patient had an isolated loss of visual acuity to 1/10 in the left eye. Endocrinological assessment was normal. CT scan demonstrated the destruction of the sphenoidal region by a large, low-attenuation, sphenoidal cystic lesion without calcification.
MR imaging showed a cystic sphenoidal extradural lesion isointense on T1-weighted images (WI) with peripheral gadolinium enhancement and hyperintense on T2 WI (Fig. 1, A–C). Its maximum diameter was 4 cm. The radiologic differential diagnoses included craniopharyngioma and mucocele.
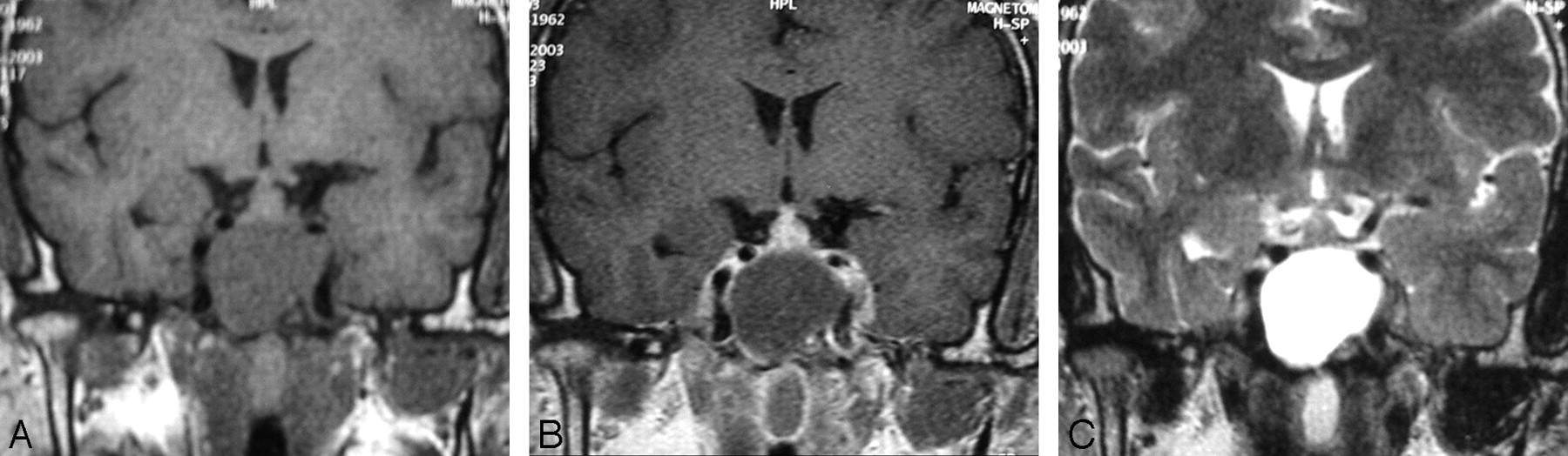
Coronal T1-weighted (A), T2-weighted (C), and postcontrast T1-weighted (B) MR images showing an intrasphenoidal cyst hypointense on T1-weighted images and hyperintense on T2-weighted images, causing destruction of the sella turcica and compression of the pituitary gland and optic chiasm. After gadolinium-diethylene-triaminepentaacetic acid administration, there is a slight enhancement of the outer border of the lesion.
The patient underwent surgery through a transrhinoseptal approach. The wall of the sphenoid sinus was paper-thin; a motor-oil- like fluid issued almost spontaneously. The cyst communicated widely with the nasal fossa, and its wall was partially extracted. The dura mater covering the sellar floor was unperforated. Pathological examination disclosed a columnar ciliated epithelium, which was consistent with an RCC.
The postoperative course was uneventful, symptoms and signs disappeared, and the patient developed no further neurologic symptoms. MR imaging performed 1 week after surgical operation showed partial evacuation of the cyst with a morphologically normal pituitary gland and stalk. MR imaging performed 1 year later (Fig. 2) revealed the disappearance of the sphenoidal cyst.
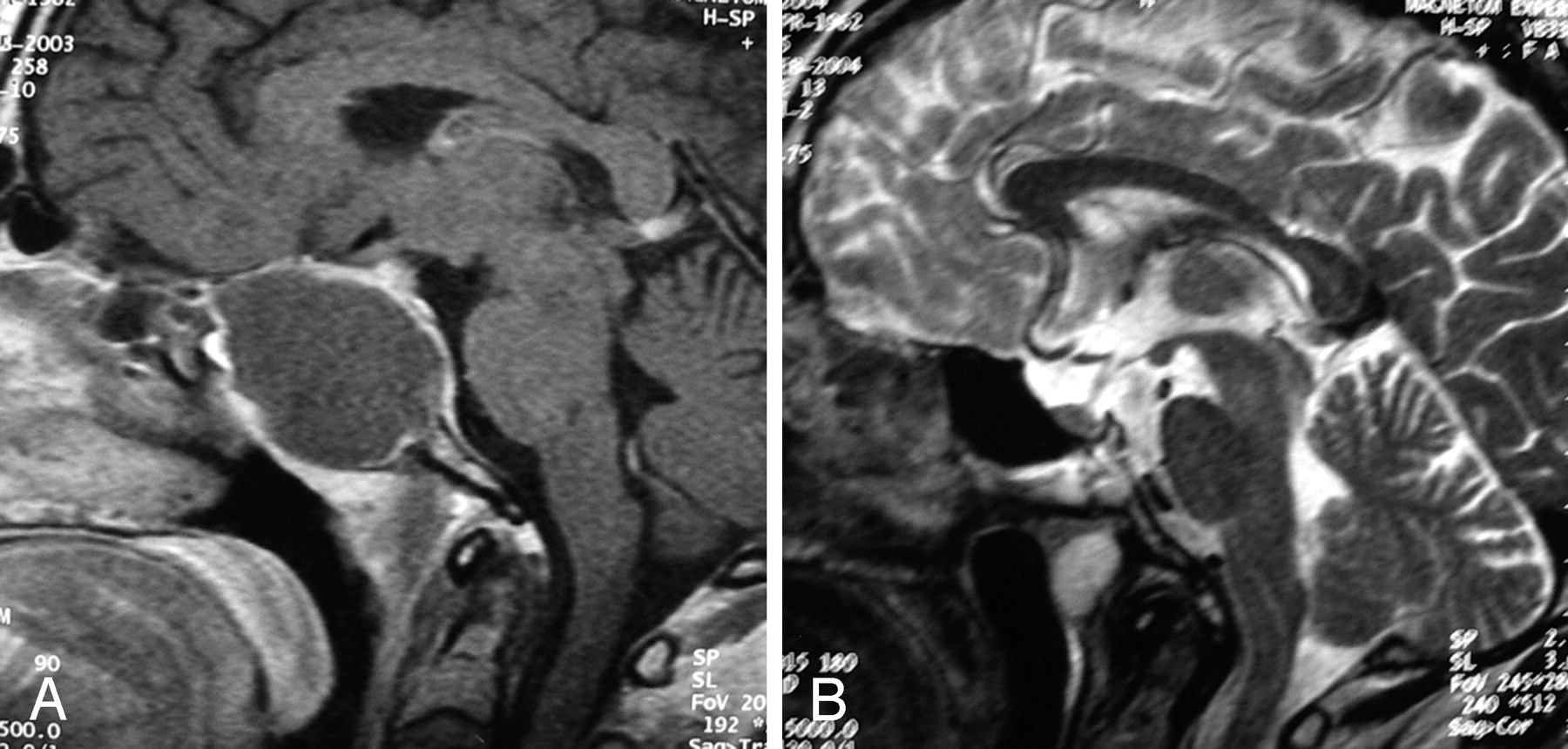
Sagittal MR gadolinium-diethylene-triaminepentaacetic acid T1-weighted images before (A) and T2-weighted images after (B) surgery showing a complete resection of the cyst.
Discussion
The sphenoidal, infrasellar origin of this RCC is supported by the absence of a suprasellar extension and by the entirely extradural location of the cyst. Ectopic sphenoidal8–10 or even clival craniopharyngioma11 have been reported, but no case of RCC has been reported in these locations.
The explanation of this location can be embryologic. Craniopharyngiomas and RCCs arise from remnants of the Rathke pouch.9,12 This pouch appears during the fourth gestational week and arises as a dorsal diverticulum from the stomodeum lined by epithelial cells of ectodermal origin. Near the same time, the infundibulum forms as a downgrowth of the neuroepithelium from the diencephalons.1 It migrates following the craniopharyngeal canal. By the 5th week, the Rathke pouch comes into contact with the infundibulum; these 2 structures give rise to the adenohypophysis and neurohypophysis, respectively.
According to Erdheim’s theory,13 a craniopharyngioma can arise from every part of the craniopharyngeal canal. This may also be true for RCC; in this case, the cyst derives from the canal enclosed in the bones of the cranial base, in contact with the walls of the pharynx.
Remnants of the craniopharyngeal canal can originate in a spectrum of cystic lesions ranging from simple RCCs to complex craniopharyngiomas.2 Harrison et al14 suggested that there is a continuum between epithelial cystic lesions of the sellar and parasellar region (craniopharyngiomas, RCCs, neuroepithelial cysts, epidermoid and dermoid cysts), which all appear to arise from the ectoderm. In some cases, they cannot be differentiated on the basis of clinical, biologic, and radiologic criteria. Even on histologic examination, there can be overlapping features. Russel and Rubinstein1 reported 2 dumbbell-shaped cysts with intrasellar components lined by cuboidal to columnar ciliated epithelium with an abrupt transition at the diaphragma sella to entirely squamous suprasellar tumors. These lesions demonstrated a histologic continuity of craniopharyngioma and RCC. In a series of 19 cases of sellar and suprasellar epithelial cystic lesions examined histologically, Harrison et al14 reported that 9 displayed significant overlapping histologic features with a solely intrasellar craniopharyngioma, which appeared to arise from an RCC with extensive squamous metaplasia.
Among the epithelial-lined cystic lesions of the sellar and parasellar region, craniopharyngiomas have the highest recurrence rates, exceeding 90% for partially resected lesions.15 At the opposite end of the spectrum lie RCCs, with a recurrence rate estimated at 5% by Voelker et al16 in their review of the literature.
Preoperative diagnosis of RCC is theoretically important, because the operative management may be limited to excision and biopsy of the cyst wall with drainage of the contents via a transsphenoidal route. CT usually shows a homogenous, low-attenuation, nonenhancing lesion.17,18 This nonspecific description matches with most of the sellar region lesions.
MR imaging allows better characterization, showing a cystic intrasellar or intrasellar and suprasellar lesion. The exclusive suprasellar location is very rare.18 The intrasphenoidal location has never been reported, which made the diagnosis difficult in our case. Moreover the maximum size of the cyst usually ranges between 6 and 26 mm in diameter.19,20 In our case, the diameter was 40 mm. Signal intensity varies widely21,22; it seems to depend on the composition of the cyst and the quantity of cholesterol, mucopolysaccharides, and proteins.23 The most constant finding is a high-intensity signal on T2 WI and an isointense or hyperintense signal on T1 WI.23 In the reported case, the cyst showed an isointense signal on T1 and hyperintense signal on T2 WI. After gadolinium-diethylene-triaminepentaacetic acid (Gd-DTPA) administration, the pituitary gland is enhanced but not the cyst, which makes it easy to identify. The position of the pituitary gland is usually around or under the cyst. In the latter situation, a very particular aspect may be realized: the sign of “the egg in a cup” that is very suggestive of RCC.23 Despite all these features, no certain diagnosis can be made, especially when there are uncommon finding as in the present observation. However, imaging gives an exact description of the position of the cyst, which better guides the surgeon and allows preservation of the normal pituitary tissue.
Even in the hands of experienced neurosurgeons, the diagnosis of RCC still remains doubtful, because of the variability of the cyst content; the most difficult diagnosis remains between RCC and craniopharyngioma.2
In a review of 155 cases of RCC, Voelker et al. concluded that the trans-sphenoidal approach is the procedure of choice for sellar and suprasellar RCC and that partial excision and drainage of the cyst is the recommended treatment for these lesions.16 It proved to be a safe and effective procedure.
On the basis of a series of 28 cases of sellar and suprasellar RCC, El Mahdy and Powall2 recommend letting the cyst wall open in the sphenoid sinus to avoid recollection and recurrent cyst formation. He used fascia lata and fat grafts only in cases in which the arachnoid membrane was breached and an important cerebrospinal fluid leak was detected.
Conclusion
The diagnosis of RCC should be suggested in case of cystic lesions of the parasellar region even inside the sphenoid bone. Clinical and radiologic features are not specific. The main differential diagnosis is craniopharyngioma. Both have the same embryologic origin, but RCCs are easier to treat and have a much better prognosis.
References
- Received May 4, 2005.
- Accepted after revision June 10, 2005.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}