
Abstract
BACKGROUND AND PURPOSE: Temporal lobe encephaloceles are increasingly identified and treated as epileptogenic foci. However, there is relatively scant research on the prevalence of asymptomatic encephaloceles. This study set out to describe the frequency of incidental temporal lobe encephaloceles and middle cranial fossa pits.
MATERIALS AND METHODS: A retrospective review was completed of high-resolution (≤0.5-mm section thickness) axial T2WI for internal auditory canal protocol imaging. The presence and laterality of middle cranial fossa pits (small bony defects containing CSF) and encephaloceles (brain parenchyma protrusion through osseous defects with or without bony remodeling) were recorded. Electronic medical records of patients with encephaloceles were searched for a history of seizure.
RESULTS: A total of 203 patients were included in the final cohort; 106 (52.2%) women. Forty-five (22.2%) patients had middle cranial fossa pits: 14 (31.1%) unilateral on the right, 17 (37.8%) unilateral on the left, and 14 (31.1%) bilateral. Ten (5.0%) patients had ≥1 encephalocele, none of whom had a documented history of seizure in the electronic medical record. No significant difference was noted in the frequency of pits or encephaloceles based on sex (P = .332 and P = .383, respectively) or age (P = .497 and P = .914, respectively).
CONCLUSIONS: Incidental middle cranial fossa pits are common findings, and their prevalence is not related to age or sex. Temporal lobe encephaloceles, though rarer, also exist occasionally among asymptomatic patients. Such findings have diagnostic implications for encephaloceles identified during imaging work-up for epilepsy.
ABBREVIATIONS:
- BHAG
- brain herniation into arachnoid granulations
- MCF
- middle cranial fossa
Both middle cranial fossa (MCF) pits and temporal lobe encephaloceles are subtypes of cephaloceles, intracranial content herniations through calvarial defects.1 MCF pits, focal bony dehiscences containing CSF but not brain parenchyma, likely represent arachnoid granulations protruding into the overlying bone; these may also be called “small meningoceles.”2 Temporal lobe encephaloceles, comparatively, are protrusions of brain through focal defects in the bone.3,4 The etiologies of pits and encephaloceles are unknown, though some have posited that increased CSF pressure or volume could play a role.2,5
Temporal lobe encephaloceles are associated with a number of processes, including otorrhea, hearing loss, and recurrent meningitis.6,7 Encephaloceles are also a known rare cause of epilepsy.3,4,8⇓–10 The first reported case led to complete seizure freedom following temporal lobectomy for a patient with an MCF encephalocele.11 Since then, several other authors have reported seizure freedom following partial temporal lobectomy or lesionectomy for symptomatic lesions.12⇓⇓–15 Nevertheless, surgical resection of encephaloceles for refractory epilepsy remains nuanced because it remains uncertain whether encephaloceles can be routinely considered epileptogenic.16
The location and small size of such abnormalities have led to under-recognition on MR imaging.4 However, as spatial resolution of MRI continues to advance, particularly with the emergence of high-field imaging systems, the identification of MCF pits and encephaloceles can be expected to increase with time.17,18 The clinical import and prevalence of pits and encephaloceles, therefore, deserve further investigation because both findings may be a source of diagnostic confusion and consternation. This study aimed to assess the prevalence of MCF encephaloceles and pits on high-resolution MR imaging in asymptomatic patients.
MATERIALS AND METHODS
Patient Selection
Institutional review board approval was obtained for this study. A retrospective review was completed of all internal auditory canal MR imaging examinations performed between January 1, 2017, and June 30, 2018. Included patients had the following: 1) MR imaging examination including a 0.5-mm axial T2 sampling perfection with application-optimized contrasts by using different flip angle evolutions (SPACE; Siemens, Erlangen, Germany) sequence or CISS or FIESTA images, and 2) imaging FOV that encompassed the osseous walls of the MCF bilaterally, requiring craniad coverage from the floor of the fossa to the floor of the sella or higher. Axial sequences were part of the dedicated internal auditory canal protocol used in our institution. Patients were excluded if images were of suboptimal quality (eg, degraded by motion artifacts).
Imaging and Clinical Review
Two neuroradiologists and a neuroradiology fellow reviewed MR images for the presence or absence of MCF “pits” (defined as extension of meninges and CSF through the inner table of the skull base, but not through the outer table, with or without bony remodeling) and the presence or absence of MCF “encephaloceles” (defined as extension of brain parenchyma through the aforementioned defect). Similar defects of the anterior and posterior cranial fossae were excluded from analysis. Lateralization (right versus left) was noted for encephaloceles and pits. For patients in whom ≥1 encephalocele was detected, a review of the electronic medical record was completed to assess a history of seizures. The body mass index of each patient was also assessed because elevated body mass indices are known to be associated with idiopathic intracranial hypertension; these were found via a retrospective review of the electronic medical record.
When a potential encephalocele was identified, the source thin axial T2 images were inspected in multiplanar reformatted images generated on a diagnostic radiology workstation running Visage Software, Version 7.1.12 (Visage Imaging, San Diego, California). Encephalocele was confirmed if the temporal lobe cortex extended into the inner table defect. Location of the encephalocele was assigned following the classification described by Wilkins, et al.19
Statistical Analysis
Association of the presence or absence of MCF pits or encephaloceles with sex was examined using a χ2 test. Differences in age by the presence or absence of MCF pits or encephaloceles was examined using t tests. Analyses were conducted using SAS (Version 9.4; SAS Institute, Cary, North Carolina).
RESULTS
Of the 204 patients who met the inclusion criteria for this study, one was excluded due to incomplete visualization of the MCF. Hence, 203 patients composed the patient cohort; 106 (52.2%) were women. The mean patient age was 53.4 ± 10.0 years.
Forty-five of 203 (22.2%) patients had MCF pits (Fig 1). Of the pits detected, 17/45 (37.8%) were unilateral on the left, 14/45 (31.1%) were unilateral on the right, and 14/45 (29.2%) were bilateral (Table 1).
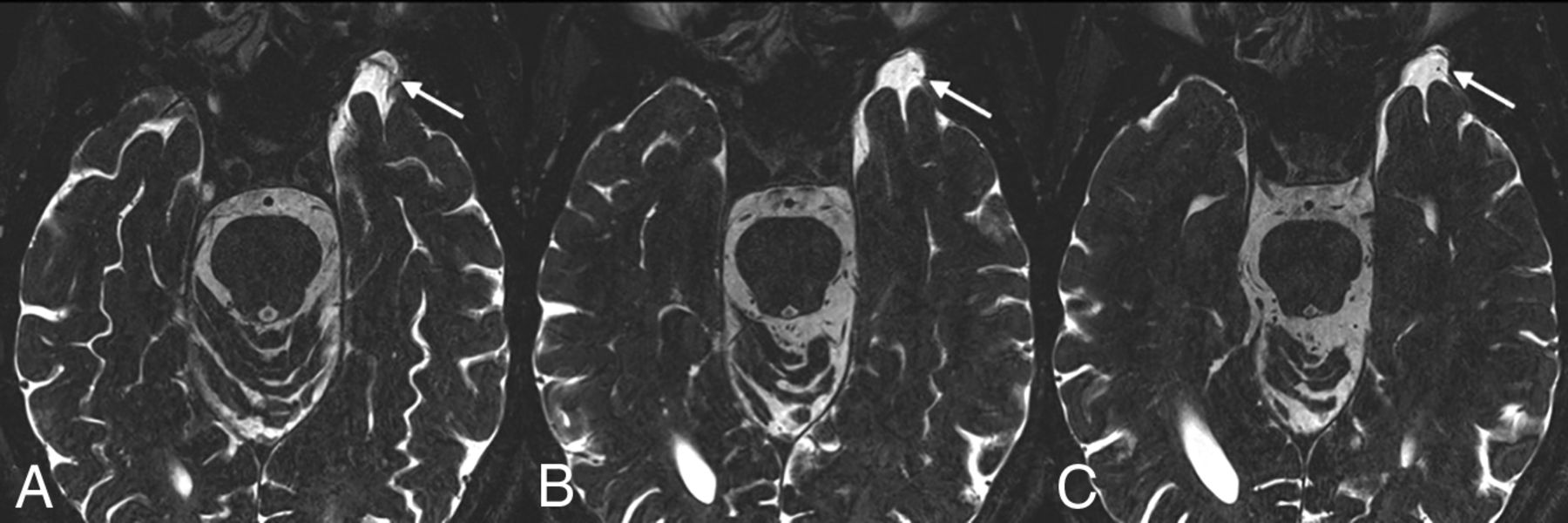
A 53-year-old man who presented with intermittent episodes of imbalance and left-greater-than-right sensorineural hearing loss. Axial T2 SPACE images (from inferior to superior, A–C) demonstrate a focal osseous defect in the greater wing of the left sphenoid bone containing CSF, consistent with an MCF pit (arrow). No herniation of brain parenchyma is present.
Number and frequency of MCF pits and encephaloceles based on lateralitya
Ten of 203 patients (5%) had 15 encephaloceles (Figs. 2 and 3). Nine of the 10 patients had single encephaloceles, 5 on the left. One patient had 6 encephaloceles, 3 on each side. Twelve encephaloceles were located in the greater wing of the sphenoid bone; the other 3, in the temporal bone. The greater sphenoid wing encephaloceles were most numerous in the anterior-inferior dural surface (10 of 12, 83%), with the remaining 2 located posteriorly, immediately lateral to the foramen spinosum and deep to the sphenoid spine. In the temporal bone, 2 of the 3 encephaloceles were located in the temporal squamosa immediately lateral to the sphenosquamosal suture; the third was located in the tegmen. Six of the 15 encephaloceles (40%) demonstrated gliosis or volume loss, compatible with encephalomalacia. The size of the observed encephaloceles ranged from 3 to 10 mm (mean, 6 mm). Six of 15 (40.0%) had some degree of associated encephalomalacia of the adjacent parenchyma. None of the patients with encephalocele had a history of seizures or epilepsy. None of the patients with encephaloceles had a known or suspected history of elevated intracranial pressure.

A 65-year-old man with a history of progressive bilateral sensorineural hearing loss. From superior to inferior (A–D), axial T2 SPACE images demonstrate a focal dehiscence of the medial right greater wing of the sphenoid (curved arrows in A and B). A small right temporal lobe encephalocele is seen protruding into the bony defect (straight arrows in B–D).

A 47-year-old woman who presented with a 2-month history of vertigo. From inferior to superior (A–D), images demonstrate a small incidental encephalocele protruding into the greater wing of the left sphenoid (arrows).
The prevalence of MCF pits in women was 26.4%, compared with 20.6% in men; no significant difference was noted in the prevalence of pits along sex lines (P = .332). Similarly, no significant difference was observed between the frequency of encephaloceles and sex (5.7% for women versus 3.1% for men, P = .383). Additionally, there was neither a significant difference in the mean age of patients with MCF pits (54.3 ± 8.7 years) compared with those without (53.2 ± 10.4 years, P = .497) nor a significant difference between the mean age of patients with encephaloceles (53.1 ± 10.1 years) compared with those without (53.5 ± 10.1 years, P = .914) (Table 2).
Comparisons of MCF pit and encephalocele frequency with age
No association was found between patient body mass index and the presence of dural pits (P = .267), nor was an association found between body mass index and encephaloceles (P = 1.000).
DISCUSSION
Most MCF pits likely arise from aberrant arachnoid granulations. Such aberrantly located arachnoid granulations expand into the calvaria but do not communicate with a venous sinus.20 Protrusion of parenchyma through these defects, commonly called brain herniation into arachnoid granulations (BHAG), is a well-documented imaging finding, though it is more often described in the posterior fossa and along the larger sinuses.5,20⇓–22 BHAG can be associated with abnormal signal of the herniated, or adjacent, parenchyma, though the findings rarely seem to be symptomatic.5 Some authors, such as Battal and Castillio,23 have sought to differentiate BHAG from classic temporal lobe encephaloceles. However, the distinction between the entities is somewhat opaque, raising the suspicion that encephaloceles and BHAG exist on a spectrum based on the severity of osseous thinning and/or remodeling. Thus, the current study will refer to brain herniation through any osseous defect as an encephalocele.
Spontaneous encephalocele is an extension of cerebral tissue and coverings into or through a defect in the skull not caused by trauma, inflammation, neoplasm, or surgical disruption. In our cohort, 14 of the encephaloceles involved the greater wing of the sphenoid bone or immediately adjacent temporal squamosal, lateral to the cranial base neural foramina (rotundum, ovale, and spinosum) and projected anteriorly or anterior-inferiorly through the inner table. A single encephalocele was located posteriorly and inferiorly in the tegmen tympani, lateral to the otic capsule and geniculate ganglion. Wilkins et al19 classified spontaneous temporal encephaloceles into 5 types, including anterior-inferior and posterior-inferior. The spontaneous anterior-inferior encephalocele is the type most commonly reported in the epilepsy literature associated with refractory temporal lobe epilepsy.24 The current study did not identify clinically occult encephaloceles of the other 3 types (anterior/spheno-orbital, anterior-medial/sphenoid sinus, or lateral/pterional). This absence may be an artifact of the volume of coverage, with the thin T2 images centered on the internal auditory canals typically not spanning the full height of the middle cranial fossa; however, in the authors’ experience, these latter types are rare in asymptomatic patients.
The identification and treatment of temporal lobe encephaloceles for refractory temporal lobe epilepsy have increased in recent years.25 The incidence of asymptomatic encephaloceles noted in the current study underscores the potential diagnostic dilemma encountered when a temporal lobe encephalocele is discovered—that is, should a temporal lobe encephalocele, identified on otherwise normal MR imaging findings of a patient with refractory epilepsy, be targeted as the potential epileptogenic focus? Alternatively, should an encephalocele ipsilateral to mesial temporal sclerosis be considered dual pathology? Future research may be useful to identify characteristics of encephaloceles that carry a higher risk of seizure foci, such as size, morphology, and abnormal signal. Until such data are gathered, radiologists and epileptologists may continue to take into account the clinical context as well data points from other modalities, including electroencephalography, PET MR imaging, SPECT, and magnetoencephalography.
To our knowledge, there have been no reported cases in which MCF pits were implicated as the direct cause of seizures. Still, pits are of conceivable clinical import: They are likely precursors of encephaloceles and could represent an early form of a spectrum of pathology that includes all cephaloceles, both pits and encephaloceles. Nevertheless, the incidence of such pits is likely underestimated on imaging; a study by Chen et al found many more middle cranial fossa arachnoid granulations on cadaveric dissections than were seen on NCCT.26 Future studies may be useful to investigate how frequently pits progress to BHAG and encephaloceles.
Our study is limited by its retrospective nature. In addition, because the detection of MCF pits and encephaloceles was based solely on axial images, it is possible that smaller abnormalities may not have been detected. Thus, it is likely that the rate of small MCF abnormalities is underestimated in this study. A more comprehensive review using coronal and sagittal sequences may have superior sensitivity for the detection MCF abnormalities. Finally, although electronic medical records of patients with encephaloceles were reviewed for a history of seizure, it is unknown whether the observed pits and encephaloceles were truly asymptomatic.
CONCLUSIONS
MCF pits are frequently observed incidental and presumably asymptomatic findings on high-resolution T2-weighted MR imaging. Temporal lobe encephaloceles, some with evident encephalomalacia, are also occasionally seen among asymptomatic patients. The incidence of such findings should be taken into account when identifying or treating such lesions as possible epileptogenic foci.
References
- Received June 20, 2019.
- Accepted after revision September 27, 2019.
- © 2019 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}