
Abstract
SUMMARY: “Encephalopathy” is a vague term that encompasses varying definitions, often with a nonspecific clinical presentation and numerous possible pathophysiologic causes. Hence, MR imaging plays a crucial role in the early diagnosis and treatment by identifying imaging patterns when there is limited clinical history in such patients with acute encephalopathy. The aim of this review was to aid in remembrance of etiologies of potentially reversible acute encephalopathic syndromes on MR imaging. The differential includes vascular (reversible cerebral vasoconstriction syndrome, transient global amnesia, disseminated intravascular coagulation, and thrombotic microangiopathy), infection (meningitis, encephalitis), toxic (posterior reversible encephalopathy syndrome, acute toxic leukoencephalopathy; carbon monoxide, alcohol-related, medication- and illicit drug-related toxic encephalopathies), autoimmune, metabolic (osmotic demyelination syndrome, uremic, acute hepatic encephalopathy), idiopathic/inflammatory (stroke-like migraine attacks after radiation therapy syndrome), neoplasm-related encephalopathy, and seizure-related encephalopathy.
ABBREVIATIONS:
- AHE
- acute hepatic encephalopathy
- ATL
- acute toxic leukoencephalopathy
- HIE
- hypoxic-ischemic encephalopathy
- ODS
- osmotic demyelination syndrome
- PRAES
- potentially reversible acute encephalopathy syndrome
- PRES
- posterior reversible encephalopathy syndrome
- PVWM
- periventricular white matter
- RCVS
- reversible cerebral vasoconstriction syndrome
- REACT
- reversible acute cerebellar toxicity
- RSL
- reversible splenial lesions
- SMART
- stroke-like migraine attacks after radiation therapy
- TMA
- thrombotic microangiopathy
- CO
- carbon monoxide
The term “encephalopathy” can seem vague with varying definitions. However, it can be broadly defined as degenerated function via various acquired disorders: metabolic disease; hematologic, endocrine, or autoimmune disorder; organ failure; inflammation; toxins; or infection.1 The clinical history varies and is typically nonspecific, but such presenting symptoms in patients with acute encephalopathy may include altered mentation, altered neurologic status, confusion, obtunded appearance, decreased level of consciousness, or coma, to name a few. Such reasons for examination should raise the concern for a potentially reversible acute encephalopathy syndrome (PRAES); thus, preliminary data have found that in such patients, nearly 75% have negative MR imaging findings, with only 25% of findings being positive for acute brain pathology.2 While the most common causes of PRAES overall are infarct-related, neurologists typically remove the term “encephalopathy” on discovering an infarct; also while hemorrhage, hydrocephalus, or trauma can present as acutely encephalopathic, their CT appearance is typically obvious.3 Thus, these entities are not included in this differential diagnosis of adult PRAES, which usually requires MR imaging for diagnosis.
This review describes a differential diagnosis for potentially recognizable PRAES on MR imaging in adults, being based predominately on their pathophysiologic etiology. It also describes potential mimics or a limited differential diagnosis for each of the presented disorders. The disorders listed in each category are provided in the Table and On-line Table. Notably, chronic encephalopathies such as from various noninfectious, neurodegenerative, or metabolic disorders are not covered this review.
Etiologies of potentially reversible acute encephalopathy syndromes
Vascular
Reversible Cerebral Vasoconstriction Syndrome.
Reversible cerebral vasoconstriction syndrome (RCVS) is a disorder of incompletely understood pathogenesis (though various underlying conditions or exposures have been described), being characterized clinically by thunderclap headaches with reversible narrowing of the cerebral arteries.4 The pathophysiology of this syndrome is thought to be related to sympathetic overactivity, irregular vascular tone, and disruption of the BBB.5 While conventional angiography is invasive but ultimately may be necessary to confirm this disorder, MR imaging with MRA is the preferred initial tool to depict the characteristic multiple areas of cerebral arterial vasoconstriction. Meanwhile, brain MR imaging can demonstrate complications or accompanying conditions, such as ischemic stroke (39%), subarachnoid hemorrhage (34%), lobar intracerebral hemorrhage (20%), or posterior reversible encephalopathy syndrome (PRES) (38%) (Fig 1).4 The symptoms usually improve within days to weeks following removal of the offending exposure.4 Of note, a scoring system (denoted RCVS2) incorporates the variables of recurrent or single thunderclap headache, carotid (intracranial) artery involvement, vasoconstrictive trigger, sex, and subarachnoid hemorrhage, with different points for each. A score of ≥5 has a high sensitivity and specificity for diagnosing RCVS, whereas a score of ≤2 excludes RCVS.6 Potential neuroimaging mimics of RCVS include vasculitis with multifocal arterial narrowing (though usually having irreversible multifocal infarcts), microemboli (typically irreversible insults lacking multifocal arterial narrowing), and infection-related encephalitis (may occasionally have arterial narrowing, but usually with avid enhancement).

Reversible cerebral vasoconstriction syndrome in a 21-year-old woman with a thunderclap headache, who thereafter became encephalopathic. SWI (A) shows a small hemorrhage (arrow). Catheter DSA via the left ICA (B) demonstrates multifocal areas of narrowing of the anterior cerebral artery and MCA segments (arrows).
Transient Global Amnesia.
Transient global amnesia is a reversible, clinical syndrome in which antero- or retrograde amnesia occurs and typically ends within 24 hours. A variety of events have been proposed to cause this entity, most of which are vascular in nature, but its exact etiology is as yet unknown.7,8 Characteristically, punctate reduced diffusion is noted unilaterally within one of the medial temporal lobes, usually in the hippocampus (Fig 2). The limited available literature on this entity states that the rate of DWI being positive varies from 11% to 84%; this varied detection rate on DWI may relate to several factors, including b-values, section thickness, and the timing of MR imaging, in which DWI performed at 24–48 hours post-symptom onset has been found to be more sensitive than an MR imaging performed within the first 24 hours.8,9 There are likely very few mimics of this condition, though in theory, microemboli or infectious insults of the medial temporal lobes could simulate this appearance.
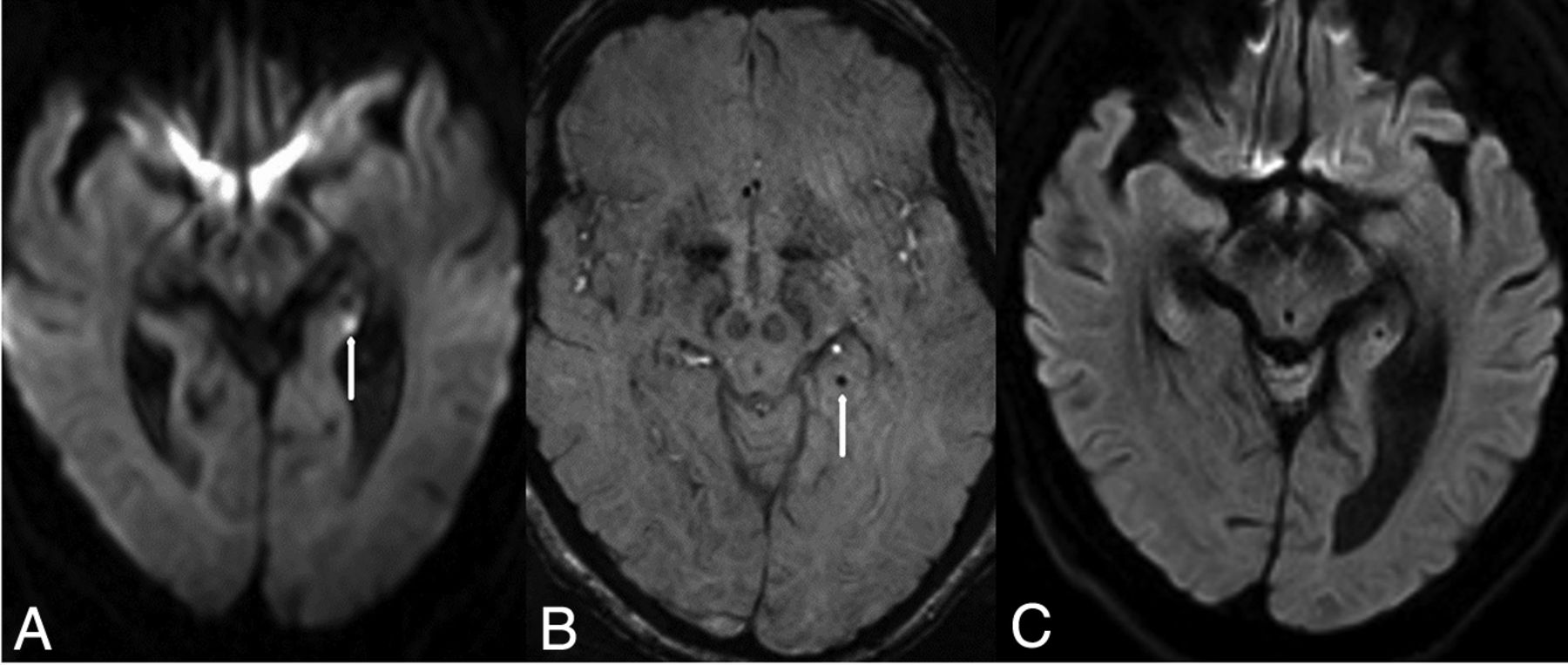
Transient global amnesia in a 60-year-old woman with a sudden onset of amnesia who had a punctate (2 mm) abnormality in the left hippocampus (arrow) on DWI (A), with corresponding hypointensity (arrow) on SWI (B). The symptoms and the punctate focus were resolved 2 days later, as noted on DWI (C).
Disseminated Intravascular Coagulation and Thrombotic Microangiopathic Encephalopathy.
Thrombotic microangiopathy (TMA) and disseminated intravascular coagulation are thrombotic entities involving diffuse microvascular occlusion. The pathophysiology of thrombotic thrombocytopenic purpura (a more common form of TMA) is thought to be due to an inability of a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13, a plasma metalloproteinase, to cleave von Willebrand Factor multimers.10 It may present with PRES (48%), while pure TMA can also be seen with diffuse microhemorrhages on SWI and small ischemic strokes (30%) (Fig 3). The imaging abnormalities can be reversible and may be limited to the time of symptomatology.10 Possible imaging mimics (with the appearance of diffuse microhemorrhages on SWI) include microhemorrhages that have developed many years post-radiation therapy, cerebral amyloidosis, treated metastatic disease (in which hemorrhagic lesions no longer enhance postcontrast), fat emboli, and diffuse axonal injury from remote trauma (usually accompanied by areas of cerebral atrophy).

Thrombotic microangiopathy in a 66-year-old woman with severe thrombocytopenia from chronic lymphocytic leukemia who presented with altered mentation. The initial MR imaging findings were negative (not shown). Ten days later, a punctate focus of reduced diffusion (arrow) was noted in the left posterior occipital lobe on DWI (A) with innumerable punctate foci on SWI related to TMA (B); however; there were no abnormalities on FLAIR or postcontrast T1WI (not shown). The symptoms resolved 3 days later.
Infection
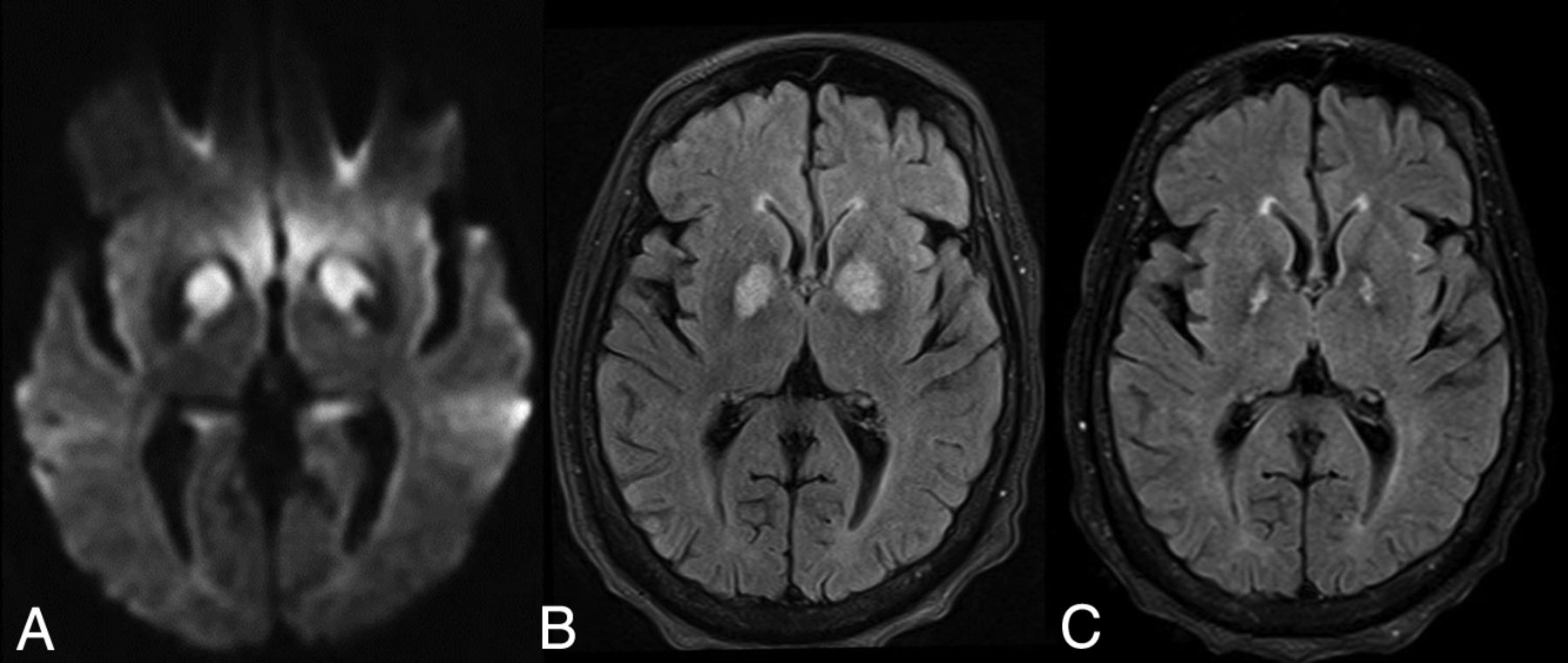
Regarding infectious meningitis, viral, fungal, and bacterial infections can initially present as encephalopathic with negative MR imaging findings. The route of invasion is either through the blood stream to the CNS due to high-grade bacteremia or via direct invasion through dural defects, or via local infections.11 Leptomeningeal enhancement is noted in up to 50%.12 While nonspecific hyperintensity may be noted within the cerebral sulci on FLAIR in meningitis, the diagnosis can be augmented by noting leptomeningeal enhancement on postcontrast T1WI or FLAIR; in particular, postcontrast FLAIR may be even more sensitive in detecting leptomeningeal disease, whether meningitis or carcinomatous.12⇓–14 In more advanced cases, DWI appears to be more sensitive than FLAIR in detecting the uncommon presence of concomitant cytotoxic edema of the cortices.15 Notably, the viral encephalitides have a multitude of appearances, in which herpes simplex virus is perhaps the most common, usually involving the temporal lobe and limbic structures. Also, various viral encephalitides have been described with basal ganglia, cortical, or thalamic abnormalities on T2WI/FLAIR; for example, in Powassan encephalitis, a tick-borne disease that can be found in the United States, there also may be scattered findings throughout the cerebellum (Fig 4).16 Regarding the presence of imaging mimics, possible mimics of leptomeningeal disease are myriad, depending on whether the neuroimaging appearance is solely nonspecific hyperintensity on noncontrast FLAIR (mimics such as subarachnoid hemorrhage, extraneous oxygen, retained gadolinium in the setting of renal insufficiency), leptomeningeal enhancement (which leptomeningeal carcinomatosis can simulate), parenchymal enhancement (mimics include primary brain tumor), or posterior fossa leptomeningeal enhancement (granulomatosis with polyangiitis, sarcoidosis, tuberculous meningitis).

Powassan viral encephalitis in a 43-year-old man with altered mentation, who had negative blood cultures for bacteremia, but positive immunoglobulin M for Powassan virus. On FLAIR (A), hemorrhages are noted of the thalami, right greater than left, also with right basal ganglia hyperintensity (arrow). Innumerable tiny foci are noted on FLAIR (B) within the cerebellar hemispheres and of the cerebellar vermis (arrow). Five months later, the symptoms and abnormal signal were almost resolved, as demonstrated on follow-up FLAIR (C and D). There was only mild residual signal in the posterior limb of right internal capsule (C, arrow).
Toxic
The term “toxic encephalopathy” encompasses a wide spectrum of encephalopathic syndromes, which may arise from exposures to substances such as chemotherapy, immunosuppressive therapy, environmental toxins, other medications, or illicit drug abuse. Such insults can involve multiple sites, including the basal ganglia, brain stem, cortices, periventricular white matter (PVWM), or the cerebellum.17,18 Notably, various toxic causes of basal ganglia injury have previously been described separately, which include carbon monoxide (CO), cyanide, opiate-induced, manganese, methanol, hepatic/hyperammonemic encephalopathy, and hydrogen sulfide.19
Posterior Reversible Encephalopathy Syndrome.
While PRES may arise from various toxic (such as medication or drug abuse) or nontoxic (such as hypertension, sepsis, or eclampsia) causes, it is listed as a toxic insult herein because the presumed pathophysiology in PRES involves endothelial toxicity or injury.20 PRES most commonly presents with seizures but can present as purely encephalopathic.20,21 It typically involves the parieto-occipital and posterior frontal cortices and subcortical WM but may extend to the PVWM, basal ganglia, brain stem, thalami, and other lobes less commonly, typically exhibiting vasogenic edema on FLAIR and DWI (Fig 5).20,21 Reduced diffusion occurs in about 10%–20%, (implying a cytotoxic component of irreversibility), and >1-cm-sized hemorrhages, in 10%–20%; such atypical findings may indicate a poorer prognosis.17,20,22 Notably, contrast enhancement is present in 37%–44% but likely has no clinical importance; thus, the use of gadolinium-based contrast is generally not considered necessary to diagnose this disorder.20,23 As noted within the discussion of RCVS, PRES may be on a spectrum that also includes RCVS. The most common mimic or differential diagnosis of PRES is hypoxic-ischemic injury due to the multifocal cortical edema on FLAIR; however, in hypoxic injury, typically the entirety of the cytotoxic edema has reduced diffusion within the cortices, while in PRES, only a minority of patients have cytotoxic edema, in which the areas of vasogenic edema far outspan focal regions of cytotoxic involvement when present. Also notable is that the presence of parenchymal or leptomeningeal enhancement on postcontrast T1WI may simulate meningitis-encephalitis or metastatic disease, but the reversibility and a typical posterior-predominant pattern usually exclude an infectious etiology.

PRES in a 72-year-old woman with esophageal cancer, treated with cisplatin, 5-fluorourocil, and radiation therapy. The patient presented with altered mental status. On FLAIR (A), there are cortical/subcortical posterior occipital abnormalities typical of mild PRES (arrows). The symptoms and FLAIR MR imaging findings resolved 1.5 months later (B).
Acute Toxic Leukoencephalopathy.
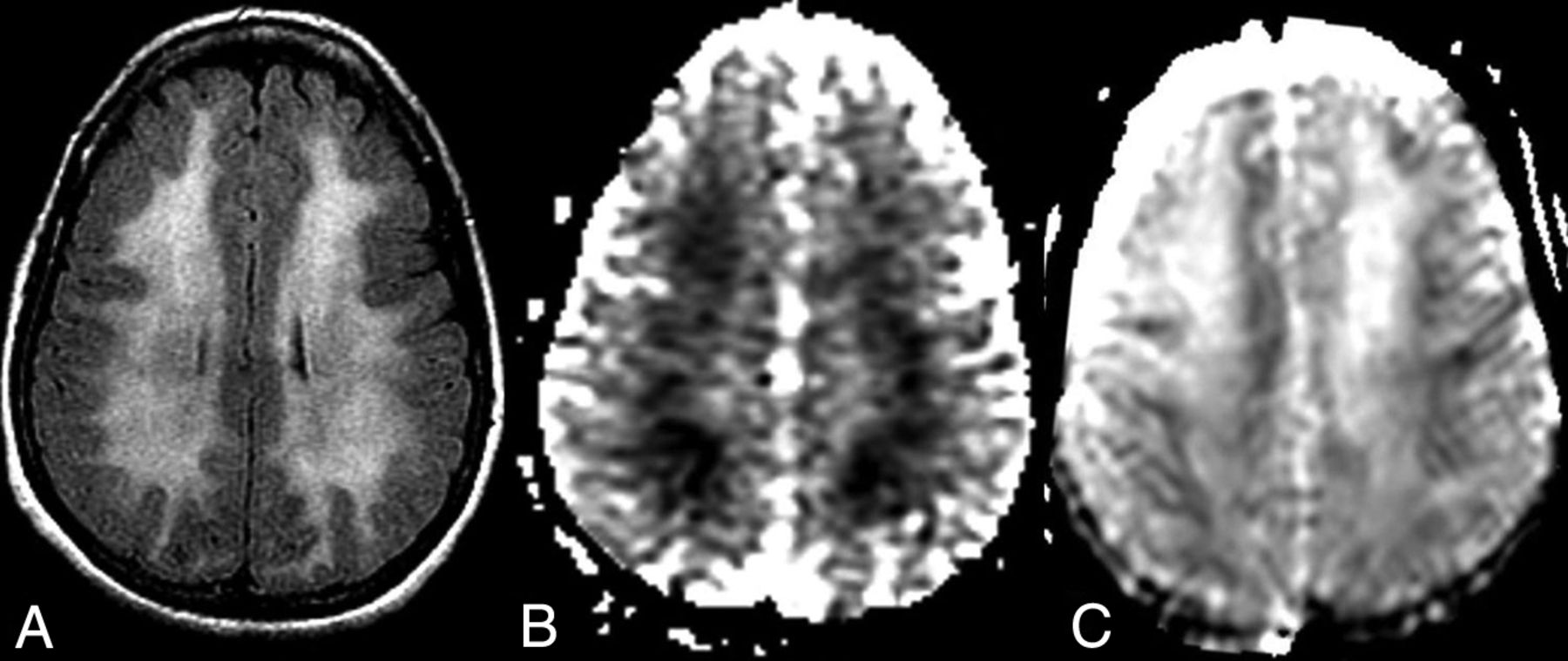
Acute toxic leukoencephalopathy (ATL) predominantly affects the PVWM and arises from exposures to various toxic substances such as chemotherapeutics (Fig 6), immunosuppressants, illicit drugs (Fig 7), other medications (such as antiepileptics or metronidazole), or environmental causes (eg, carbon monoxide [CO]).24 The etiology of noninfectious and nonmetabolic ATL can be easily remembered by the acronym “CHOICES,” which represents chemotherapeutic agents; heroin-induced (illicit usage), opioid medication–related overdose; immunosuppressant drugs; cocaine abuse; environmental causes (such as carbon monoxide or ethanol); and seizure-related splenial lesions (such as from antiepileptic drugs).25 The syndrome of a reversible splenial lesion (RSL) may be considered a subtype of ATL and is described later in this review.17,24 Notably, ATL is a less common cause of encephalopathy relative to PRES in patients receiving immunosuppression or chemotherapy; thus, ATL occasionally occurs simultaneously with PRES in 2% of patients with PRES, perhaps because both entities are thought to result from endothelial toxicity.20,26,27 Mimics of ATL are a subacute phase of hypoxic-ischemic encephalopathy (HIE) and CO toxicity because they all can present as reduced diffusion within the PVWM.28

Acute toxic leukoencephalopathy in a 57-year-old man receiving 5-fluorourocil for esophageal cancer who presented with altered mental status 5 days before the initial MR imaging. On that MR imaging, there was symmetric bilateral reduced diffusion of the PVWM on DWI (A) and an ADC map (B). Nineteen days later, the symptoms and MR imaging findings had nearly resolved, as demonstrated on an ADC map (C).
Opioid-related acute toxic encephalopathy in a 44-year-old woman with “chasing the dragon” from opioid inhalation who was found unresponsive. On FLAIR (A), there is a symmetric PVWM abnormality bilaterally, with corresponding reduced diffusion on an ADC map (B). Ten days later, the MR imaging demonstrated T2 shine through on the ADC map, with corresponding slowly improving mentation clinically (C).
Carbon Monoxide.
CO poisoning is an environmental cause of toxicity and results in >20,000 emergency department visits and 450 deaths annually.29 The pathophysiology of CO toxicity has 2 different generally described mechanisms. The first is the formation of carboxyhemoglobin, which reduces the oxygen-carrying capacity of the blood, thus inducing an anemic form of tissue hypoxia. The other pathway is toxic in nature, related to inhibition of the mitochondrial electron transport enzyme system, which activates polymorphonuclear leukocytes, thus causing brain lipid peroxidation.29,30 CO-related encephalopathy is important to recognize because it can be reversible, with varying sites of brain injury. On DWI and FLAIR in the acute phase, the most commonly involved areas are the lentiform nuclei, caudate nuclei, or PVWM (ie, presenting as a form of ATL); less commonly, the hippocampi are involved (Fig 8).29 Depending on the involved site, a mimic of CO toxicity can be opiate toxicity (which may also incur in basal ganglia, PVWM, or hippocampal injury); notably, other causes of PVWM injury include ATL (of which CO could be considered a cause) and the subacute phase of HIE (having PVWM-reduced diffusion in the later phase).28
CO toxicity in a confused 28-year-old man found obtunded above a garage, having elevated serum CO levels. As is typical of CO toxicity, reduced diffusion and hyperintense signal were noted within the bilateral globi pallidi on DWI (A) and FLAIR (B), respectively. One year later, atrophy of the globi pallidi was present on FLAIR (C).
Alcohol-Related Acute Encephalopathies.
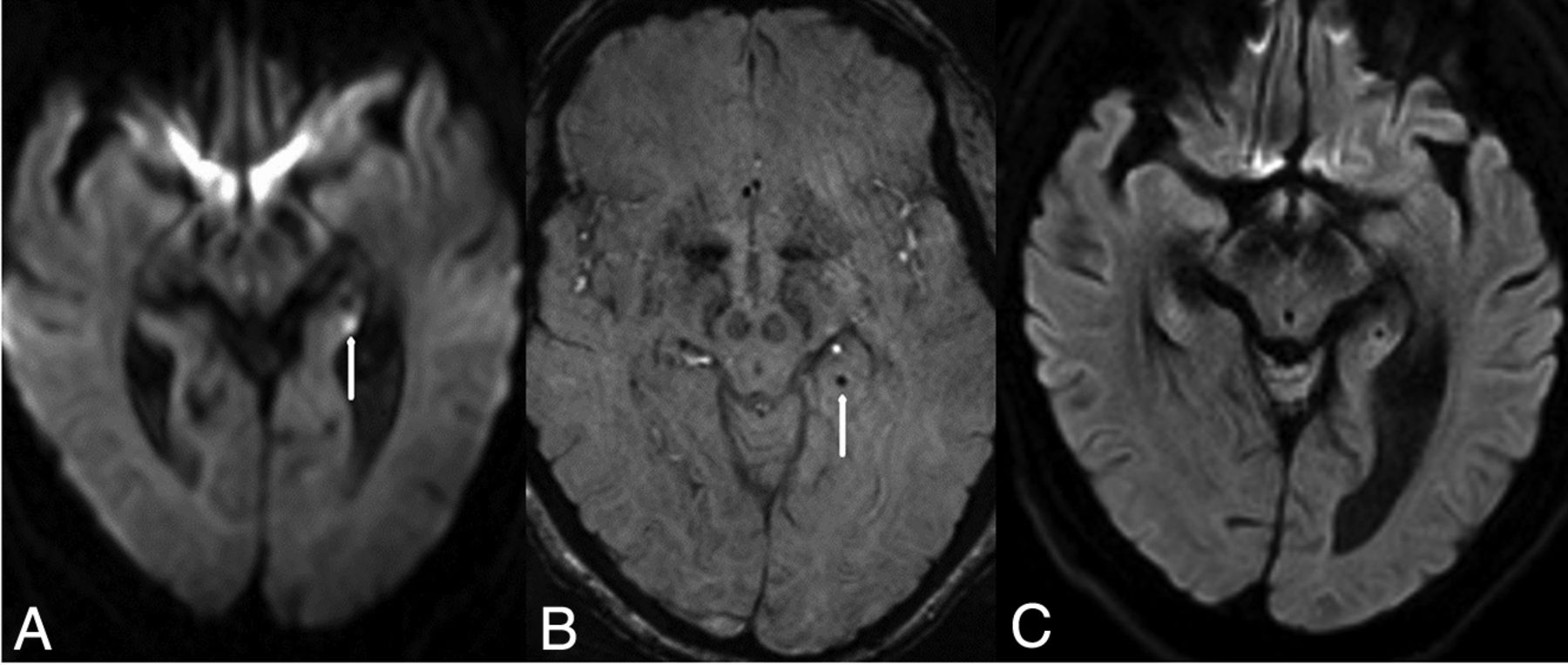
Alcohol-related acute encephalopathies are diseases that directly or indirectly occur in the setting of chronic alcohol abuse, including Marchiafava-Bignami disease, osmotic demyelination syndrome (ODS), and sometimes Wernicke encephalopathy. Wernicke encephalopathy is a neurologic emergency caused by thiamine deficiency (thiamine is needed for blood-brain barrier integrity), most commonly from alcohol abuse, though occasionally from starvation. It characteristically affects the dorsomedial thalami, mammillary bodies, tectal plate, periaqueductal gray matter, and surrounding the third ventricle symmetrically (Fig 9).31 Of note, Marchiafava-Bignami disease is not further elucidated herein because it is a relatively irreversible entity.31 ODS and acute hepatic encephalopathy (AHE) are described in detail in the following sections. Mimics can vary depending on site of involvement, which can be postischemic (for example, thalamic/hypothalamic or brain stem injury secondary to the artery of Percheron infarction, thalamogeniculate perforator infarction, or deep cerebral vein thrombosis) or infectious insults (such as related to rhombencephalitis or meningitis, which can cause abnormal parenchymal signal on FLAIR or DWI, or leptomeningeal enhancement).

Wernicke encephalopathy in a 47-year-old woman with altered mentation, who was not seen for several days, having been found unresponsive in her apartment. Reduced diffusion was noted of the mamillary bodies (arrow) and periaqueductal region (dotted arrow) on DWI (A), with thalamic abnormalities (arrows) on FLAIR (B). The symptoms and DWI findings resolved 1 week later (C).
Other Medication-Related and Illicit Drug–Related Toxic Encephalopathies.
As above, PRES, ATL, and RSL are medication-related toxic PRAESs that have been increasingly described during the past 2 decades.17 A newly recognized pattern of medication-related encephalopathy is reversible acute cerebellar toxicity (REACT), which lacks supratentorial involvement. REACT has been rarely described but has been found to arise from exposure to several chemotherapeutic or opioid agents; the diffusion reduction is characterized by being localized to the cerebellar cortices on DWI and ADC maps (Fig 10).32,33

REACT syndrome in a 53-year-old woman with encephalopathy on 5-fluorouracil who had reduced diffusion within the cerebellum on diffusion-weighted MR imaging (A, arrows). This resolved 12 days later on DWI (B).
RSL can be described as a subtype of ATL because their appearance and etiology can overlap; such etiologies include antiepileptic drugs, infections, chemotherapeutics, immunosuppressants, or certain uncommon metabolic conditions. RSL presents as focally reduced diffusion in the callosal splenium, with or without a corresponding abnormality on FLAIR, which typically resolves within days (Fig 11).17,34

Reversible splenial lesion in a 35-year-old man on antiepileptic medications for seizures who presented with mildly altered mental status, having a lesion on DWI (A, arrow). The symptoms and DWI findings had completely resolved in 5 days (B).
While selective serotonin reuptake inhibitors are traditionally considered safe medications, a few case reports have been described of reversible neurotoxicity in overdoses; in such instances, pallidal, PVWM, or callosal injury are variably seen (Fig 12).35

Sertraline overdose in a 22-year-old man with T2 shine through in the insula (A, dotted arrows) and bilateral internal capsules on DWI (A, arrows), with high signal of the subcortical and deep temporo-parietal WM on FLAIR (B, arrows). Five days later, the MR imaging findings had resolved, as noted on DWI (C) and FLAIR (D).
Metronidazole-induced encephalopathy is a rare toxic encephalopathy. The cerebellar dentate nuclei are the typical site of involvement, followed by the midbrain, callosal splenium, pons, medulla, hemispheric subcortical WM, and the basal ganglia.32
Autoimmune Encephalitis
Autoimmune encephalitis involves immune-mediated inflammation of the brain, with a number of subgroups based on the site to which the antibody is reacting, with varying prognoses; these can be classified as classic paraneoplastic with antibodies to intracellular antigens (eg, anti-Hu with a poor prognosis), autoantibodies to cell-surface receptors or their associated proteins (eg, anti-N-methyl-D-aspartate receptor subtype with a better prognosis), intermediate types of disorders with autoantibodies to intracellular synaptic proteins (eg, anti-glutamic acid decarboxylase with variable prognoses), and other types of systemic disorders in which there is not a uniformly understood antigen and of varying prognoses related to the underlying condition (eg, lupus, Graves disease, Hashimoto disease).36 On MR imaging, these disorders usually (but not always) involve the limbic system; the cortices or WM may also be variably involved. A majority of patients have negative MR imaging findings, but when visible, autoimmune encephalitis usually involves the limbic system, particularly the mesial temporal lobes.36,37 Cortical edema on FLAIR is noted in affected areas, often lacking reduced diffusion or contrast enhancement; less commonly, cerebellar, thalamic, brain stem, and spinal cord involvement have also been described (Fig 13).36,37 Regarding potential mimics, the basal ganglia involvement in autoimmune encephalitis helps to distinguish it from infectious encephalitis (such as herpes simplex virus), which typically spares the basal ganglia and usually enhances on postcontrast T1WI following gadolinium administration; notably, human herpesvirus 6 can also involve the medial temporal lobe as a form of limbic encephalitis in immunosuppressed individuals.

Autoimmune encephalitis in a 23-year-old man with a history of acute lymphoblastic leukemia treated with chemotherapy 2 years prior. He presented with worsening headache and speech changes. There was hyperintense signal within the left hippocampus on FLAIR (A, arrow), which did not have reduced diffusion and did not enhance on postcontrast T1WI (not shown) because the infectious work-up findings were also negative. The hippocampal abnormality resolved 1 year later on follow-up FLAIR (B).
Metabolic
Osmotic Demyelination Syndrome.
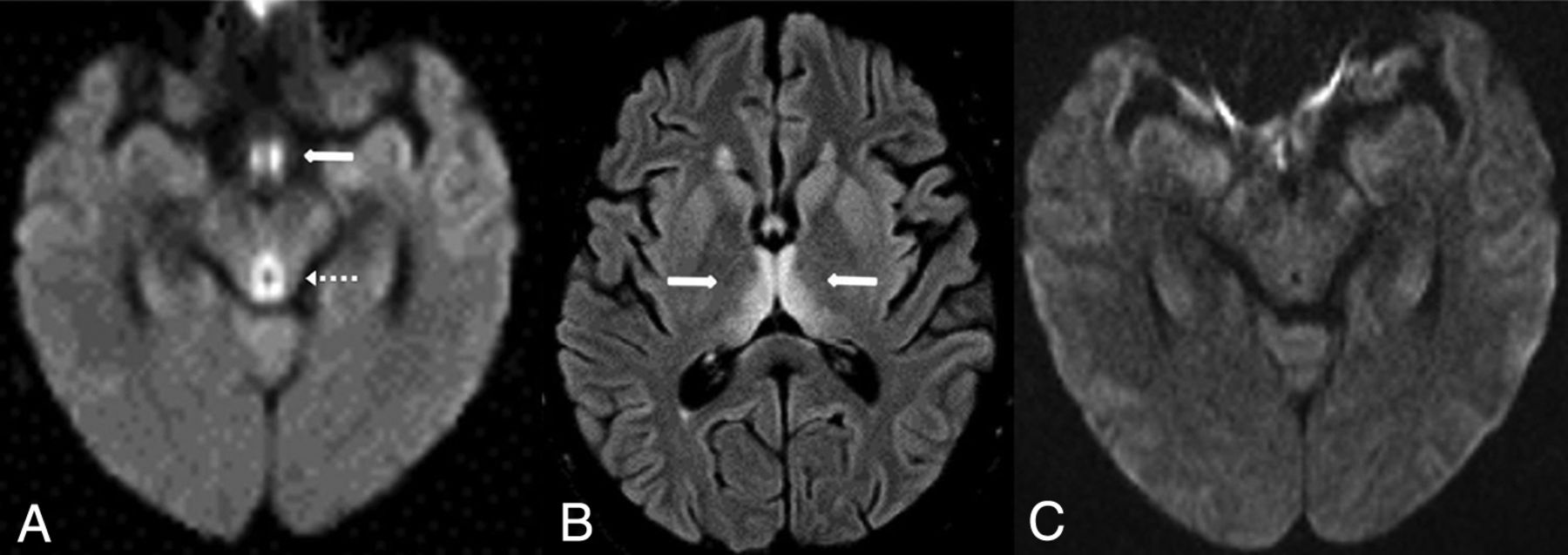
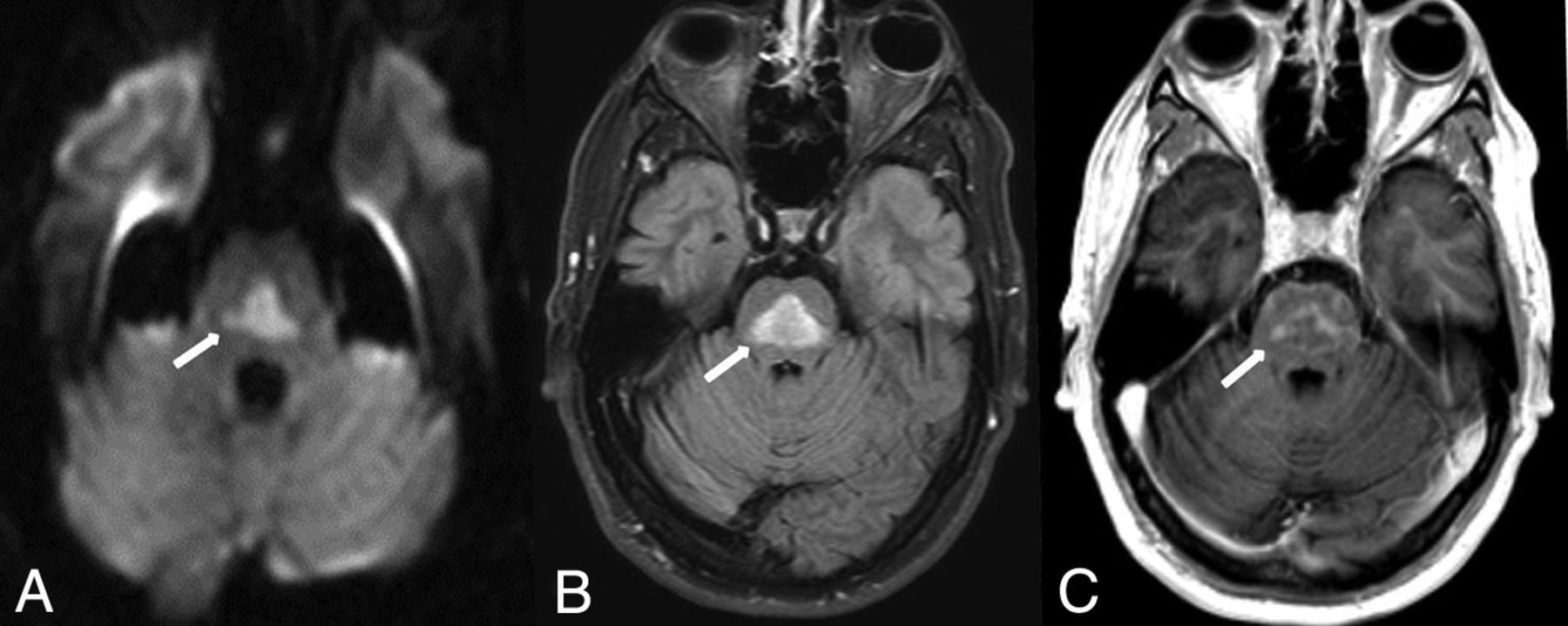
ODS can be fatal, resulting from the destruction of myelin sheaths in oligodendrocytes due to rapid osmotic shifts (usually with rapid corrections in serum sodium or, less commonly, potassium); predisposing conditions include end-stage renal disease, hepatic insufficiency, transplantation, and malignancies.38 ODS is partially reversible with immediate intervention. Two characteristic patterns of involvement exist but may overlap in imaging appearance: extrapontine myelinolysis and central pontine myelinolysis. The central pontine variant affects the pons (Fig 14), while the extrapontine version involves the basal ganglia, thalami, hippocampi, and/or the PVWM; hence, both variants can occur simultaneously. Reduced diffusion on DWI is the earliest finding, which appears within 24 hours of the clinical symptom onset; contrast enhancement may be present in involved regions in the subacute phase.38 Neuroimaging mimics of this condition include other entities with contrast enhancement or reduced diffusion in the pons, from either postischemic (such as small infarcts in the distribution of pontine perforating vessels) or postinfectious etiologies (such as rhombencephalitis, though usually accompanied by pontine swelling).
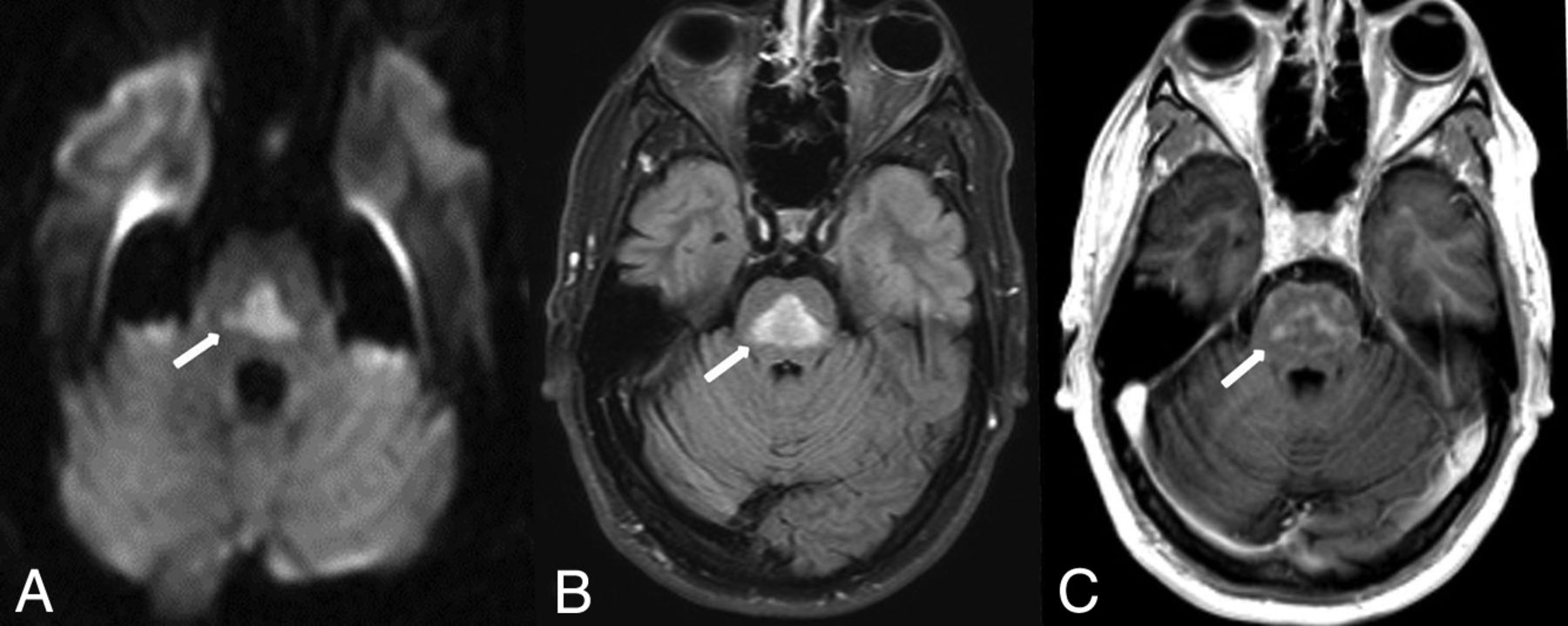
Pontine-type ODS in a 45-year-old man who presented with acute confusion due to a correction of the serum sodium (Na+) level from 101 mEq/L during 1 day. There was characteristic pontine reduced diffusion on DWI (A, arrow) and FLAIR (B, arrow). Postcontrast T1WI demonstrated mild enhancement, consistent with the subacute phase of ODS (C, arrow).
Uremic Encephalopathy.
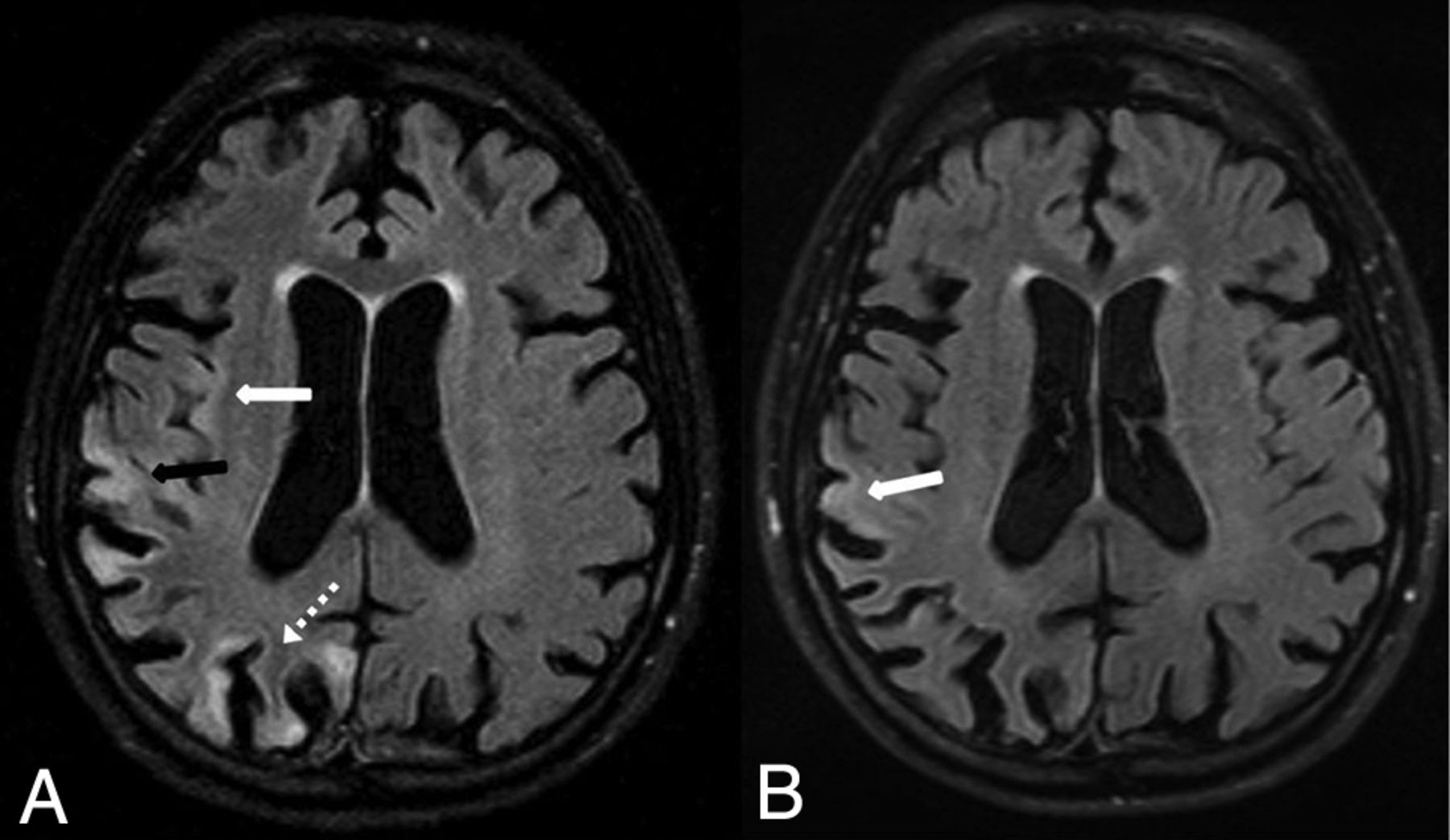
Uremic encephalopathy is a reversible metabolic disorder that occurs in incompletely treated end-stage renal disease.17,39 The pathophysiology of this entity is uncertain, but many contributing factors have been described, such as hormonal disturbances, oxidative stress, accumulation of metabolites, imbalance in excitatory and inhibitory neurotransmitters, and disturbances of intermediary metabolism.40 The MR imaging appearance is varied and scantly described and can also overlap with the appearance of either AHEs in milder cases (insular edema) and with ATL (PVWM edema) in the more severe form. It can appear as T2WI/FLAIR hyperintensity in the basal ganglia or can have cortical/subcortical involvement (predominantly the parieto-occipital lobes), insular edema, or PVWM involvement (Fig 15). Preliminary effort focuses on whether the MR imaging findings correlate with the serum blood urea nitrogen level. On DWI, reduced diffusion is variably present, but the involved regions lack contrast enhancement.39 The basal ganglia lentiform fork sign has been described but may be nonspecific because it has also been reported in the setting of metabolic acidosis.41 Hence, further work is needed to describe the various appearances of this disorder. Mimics of this syndrome depend on the sites involved on MR imaging: Insular or cortical edema can simulate hepatic/hyperammonemic encephalopathy (usually excluded by lack of an elevated serum ammonia level), while the basal ganglia edema in this syndrome can simulate postanoxic injury (particularly if reduced diffusion is present).28,42

Two different appearances of uremic encephalopathy. A and B, A 54-year-old man with chronic kidney disease, altered mental status, and an acute rise in the blood urea nitrogen level (range, 45–114 mg/dL during the 10 days prior). Reduced diffusion was present within the bilateral insular cortices, as shown on FLAIR (A, arrows). By 40 days later, the insular abnormalities had resolved on FLAIR (B). C–E, A different 18-year-old male patient (previously healthy) with altered mental status from more severe uremic encephalopathy. The patient was later found to be in end-stage acute renal failure (blood urea nitrogen level range, 90-114 mg/dL during the 2 days before MR imaging). The initial MR imaging demonstrated reduced diffusion on DWI (C, arrows) within the posterior PVWM, but without abnormality on FLAIR (D). One month later, the symptoms and DWI MR imaging findings (E) had resolved, without abnormalities on FLAIR (F).
Acute Hepatic (or Hyperammonemic) Encephalopathy.
AHE is a potentially reversible entity that usually occurs in the setting of end-stage liver disease. The pathophysiology is thought to be related to increased hepatic resistance that forces toxic substances into the systemic circulation via portosystemic shunts. Subsequently, ammonia is taken up by the brain and has been shown to be toxic to both astrocytes and neurons; besides acute toxicity, such ammonia deposition ultimately can lead to irreversible structural changes in astrocytes in the setting of a chronic exposure.43 In such chronic hepatic insufficiency, bilateral pallidal hyperintensity on T1WI is a typical finding, reflecting the chronic accumulation of manganese from failed hepatobiliary excretion; such T1 hyperintensity can variably present with mild PVWM T2 abnormalities that can improve post-transplantation.42 However, in the acute phase, the most commonly involved areas in milder cases of AHE are the PVWM, internal capsules, thalami, insula, or the corticospinal tracts, which can overlap in appearance with both uremic encephalopathy and ATL (Fig 16).42 These are variably present on DWI or FLAIR and may not be apparent on both sequences. The clinical and imaging findings of AHE are typically reversible with therapy. In more severe cases (having extremely elevated serum ammonia levels), there may be basal ganglia or diffuse cortical injury, being associated with poorer outcomes.42,44

AHE in a 34-year-old woman with acute liver failure from acetaminophen overdose, having severe serum ammonia level elevation (206 μg/dL), with characteristic insular (dotted arrows) and thalamic involvement (arrows) on FLAIR (A) and T2WI (B). By 3 weeks later, the signal abnormalities and symptoms had resolved, but there was mild resultant insular atrophy (C).
Mimics of AHE on brain MR imaging include uremia (similarly, the patient may have cortical or insular edema, but it is excluded by a normal serum ammonia level) and HIE (the patient may have cortical edema with reduced diffusion that is more profound than AHE and irreversible, with a normal serum ammonia level). Other less common entities that have diffuse cortical edema are also considerations, including PRES, RCVS, mitochondrial cytopathies, prolonged seizures, Creutzfeldt-Jakob disease, and hypoglycemic encephalopathy.45
Idiopathic/Inflammatory: SMART Syndrome
Stroke-like migraine attacks after radiation therapy (SMART) syndrome is an acronym that implies reversible symptoms occurring years after radiation therapy; these episodes typically occur >5–10 years post-cranial irradiation.46 The characteristic appearance is transient cortical hyperintensity on T2WI/FLAIR (without reduced diffusion), focal gyral edema, and the classic finding of reversible gyral enhancement of the affected cortex, usually being unilateral (Fig 17).46,47 To solidify the diagnosis, SWI can help detect the numerous radiation-induced cavernous hemangiomas that are typically present; there is usually reversible gyral enhancement on postcontrast MR imaging that resolves within several days.47,48 Neuroimaging mimics on postcontrast imaging include primary brain neoplasm and infection (meningitis), both excluded by the resolution of the abnormal enhancement after several days of purely supportive therapy.

SMART syndrome in a 56-year-old man with acute headaches and confusion, who had a history of radiation therapy >40 years ago for a pineal tumor. Unilateral, gyriform temporo-occipital enhancement was noted on postcontrast T1WI (A), with numerous microhemorrhages on SWI (B). The symptoms resolved 4 days later, along with resolution of the abnormal enhancement on postcontrast T1WI (C).
Neoplasm-Related Encephalopathy (Leptomeningeal Carcinomatosis)
Leptomeningeal carcinomatosis involves the pia mater, arachnoid, and subarachnoid space. The most common types to metastasize to this space are breast, lung cancer, and melanoma.49 Because the initial presentation of such patients with leptomeningeal disease can be encephalopathic, the radiologist should keep this entity in mind as a part of the differential diagnosis in a patient with acute encephalopathy. The most common MR imaging findings are contrast enhancement within the sulci (on T1WI or FLAIR) along the convexities, tentorium, or basal cisterns (Fig 18). Of note, infection is also in the differential for this appearance, which is the most common imaging mimic and can be differentiated by lumbar puncture.49,50 Other mimics include tuberculosis if the enhancement is along the basal cisterns or posterior fossa (excluded by diagnostic lumbar puncture or serum testing), and similarly sarcoidosis and granulomatosis with polyangiitis.

Leptomeningeal carcinomatosis in a 60-year-old man with an acute presentation of altered mental status and seizure. The initial MR imaging demonstrated leptomeningeal hyperintense signal and enhancement on pre- (A, arrows) and postcontrast FLAIR (B, arrows), diagnosed as metastatic melanoma later via direct biopsy. The imaging findings were completely resolved 3 months later, as demonstrated on pre- (C) and postcontrast FLAIR (D).
Seizure-Related Encephalopathy
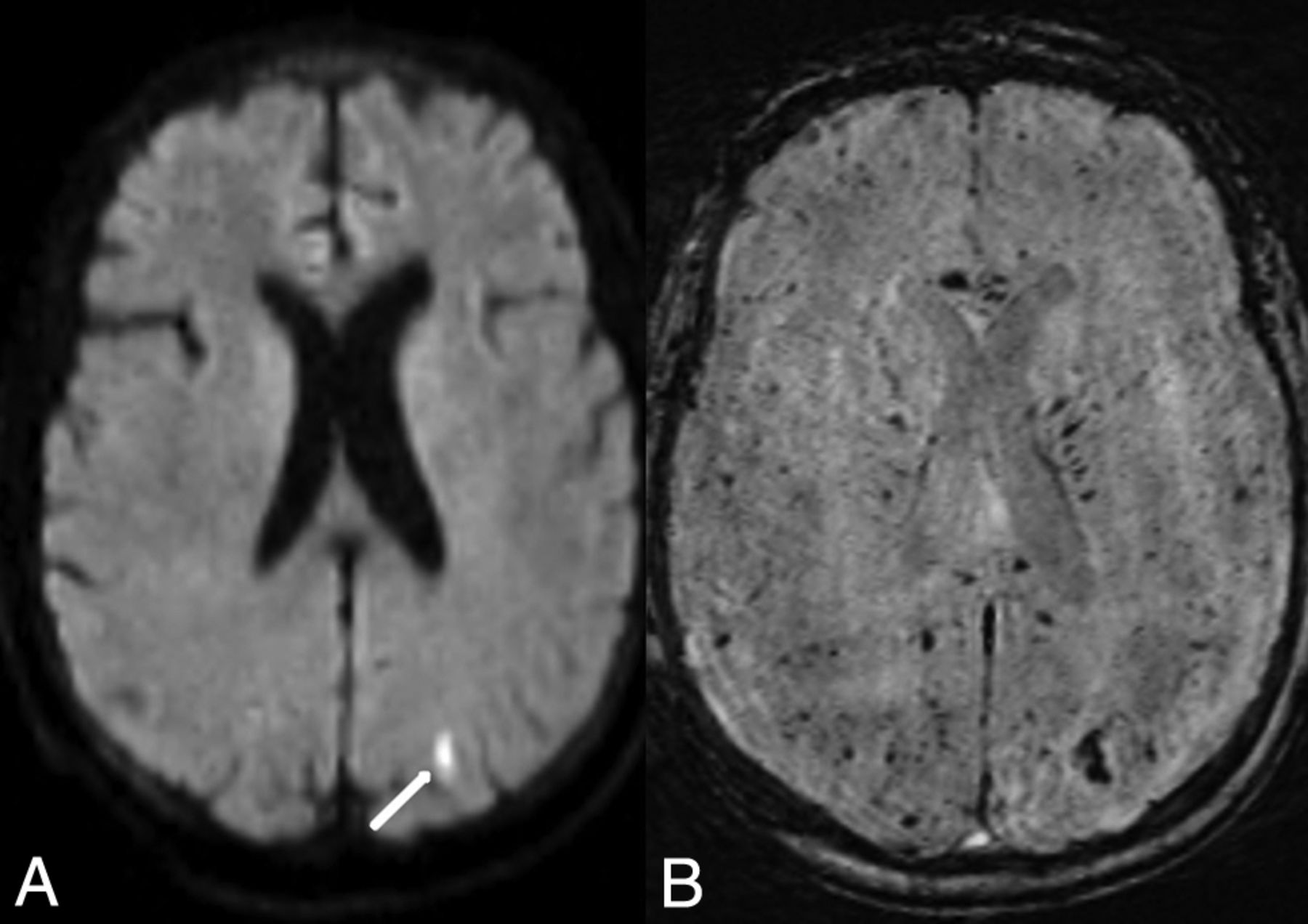
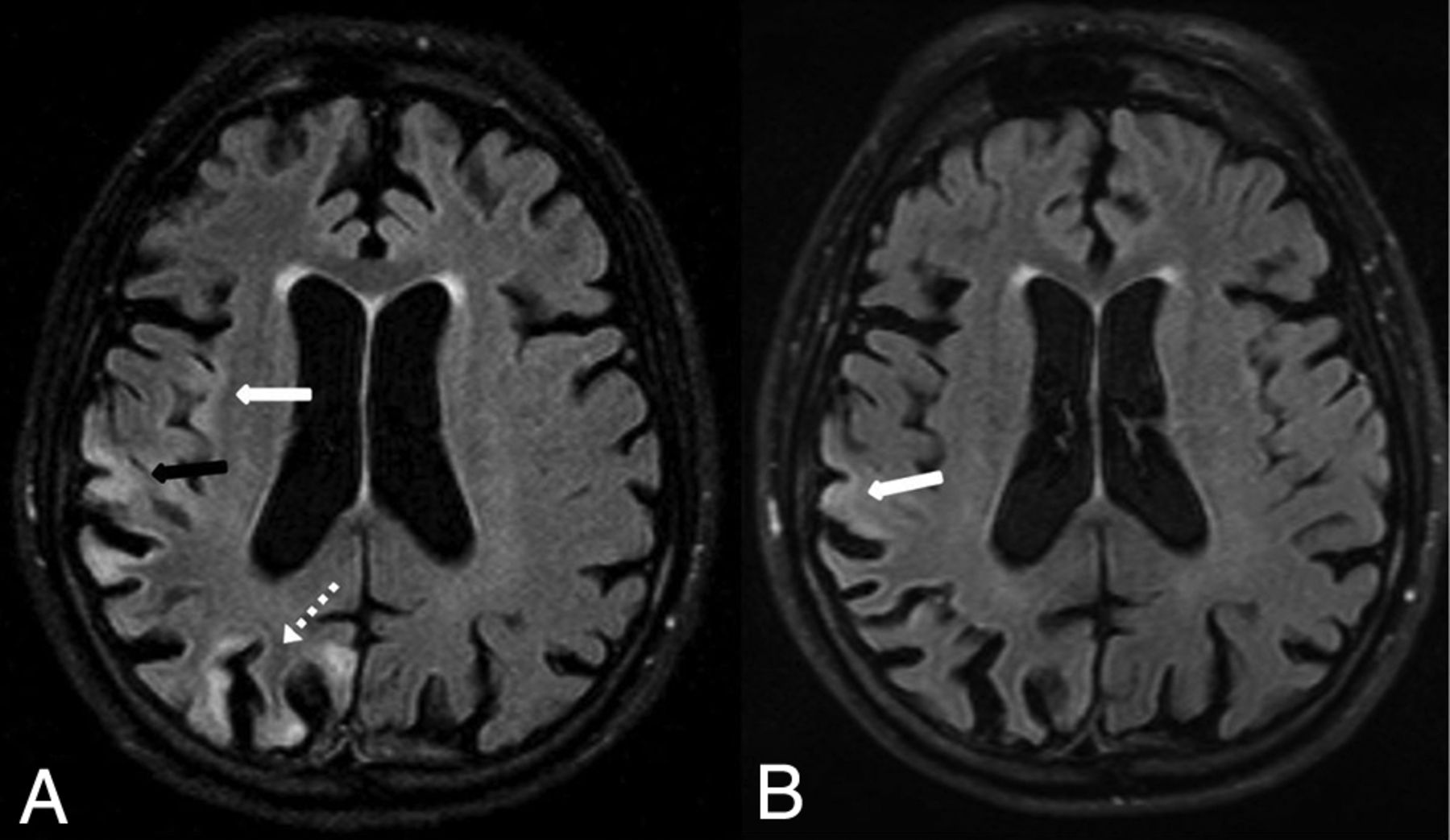
A postictal state or prolonged seizures can cause potentially reversible brain MR imaging abnormalities on both DWI and FLAIR MR imaging. The underlying mechanism of such abnormalities is thought to be related to increased neuronal activity and its associated metabolic and vascular responses.51 While a well-known location is the hippocampus, other areas of potential involvement (usually unilateral) include the cortices and subcortical WM, callosal splenium, and, less commonly, the basal ganglia, thalami, and cerebellum. Each of these regions is potentially reversible, depending on the length of the seizure because continually prolonged seizures (status epilepticus) can result in irreversible cortical injury (Fig 19).52 Neuroimaging mimics of multifocal cortical edema include RCVS, mitochondrial (cytopathy/encephalopathy), encephalitis (infectious meningoencephalitis), hypoglycemia, AHE (excluded by a normal serum ammonia), HIE (in contrast, it is usually irreversible and typically bilateral), Creutzfeldt-Jakob disease (usually cognitive decline from weeks to months and may involve the basal ganglia), uremia (usually with an elevated blood urea nitrogen level), and PRES (usually bilateral with multiple posterior-dominant regions of involvement).45
Status epilepticus in a 58-year-old man with reduced diffusion (not shown) and high signal on FLAIR (A) within the right parietal (A, black arrow), occipital (A, dotted arrow), and insular cortices (A, white arrow). By 12 days later, the findings were mostly resolved except for mild residual hyperintensity within the right parietal cortex, as demonstrated on follow-up FLAIR (B, arrow).
CONCLUSIONS
This article reviews potentially reversible acute encephalopathic syndromes that are potentially recognizable on MR imaging, with their etiologies, differential diagnoses, and neuroimaging mimics. Prompt recognition of the characteristic MR imaging findings in these reversible syndromes enables early diagnosis and therapy. In particular, because the initial or presenting clinical history of an “encephalopathy” can be noncontributory, the involvement of particular regions on FLAIR or DWI may aid the radiologist in promptly narrowing the differential diagnosis, which can affect the clinical outcome.
Footnotes
Disclosures: Alexander M. McKinney—UNRELATED: Board Membership: Veeva Systems Inc, Comments: President and CEO of VEEV Systems Inc, a company that develops informatics solutions; Patents (Planned, Pending or Issued): President and CEO of Veeva Systems Inc, a company that develops informatics solutions.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received October 28, 2019.
- Accepted after revision April 26, 2020.
- © 2020 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.