
Abstract
BACKGROUND AND PURPOSE:Comprehensive diagnostic criteria encompassing the varied clinical and radiographic manifestations of spontaneous intracranial hypotension are not available. Therefore, we propose a new set of diagnostic criteria.
MATERIALS AND METHODS: The diagnostic criteria are based on results of brain and spine imaging, clinical manifestations, results of lumbar puncture, and response to epidural blood patching. The diagnostic criteria include criterion A, the demonstration of extrathecal CSF on spinal imaging. If criterion A is not met, criterion B, which is cranial MR imaging findings of spontaneous intracranial hypotension, follows, with at least one of the following: 1) low opening pressure, 2) spinal meningeal diverticulum, or 3) improvement of symptoms after epidural blood patch. If criteria A and B are not met, there is criterion C, the presence of all of the following or at least 2 of the following if typical orthostatic headaches are present: 1) low opening pressure, 2) spinal meningeal diverticulum, and 3) improvement of symptoms after epidural blood patch. These criteria were applied to a group of 107 consecutive patients evaluated for spontaneous spinal CSF leaks and intracranial hypotension.
RESULTS: The diagnosis was confirmed in 94 patients, with use of criterion A in 78 patients, criterion B in 11 patients, and criterion C in 5 patients.
CONCLUSIONS:A new diagnostic scheme is presented reflecting the wide spectrum of clinical and radiographic manifestations of spontaneous spinal CSF leaks and intracranial hypotension.
Spontaneous intracranial hypotension is an increasingly recognized cause of new daily persistent headaches, particularly among young and middle-aged people, but an initial misdiagnosis remains common.1 Mechanical factors combine with an underlying structural dural disorder to cause the primary spontaneous spinal CSF leak.2,3 The prototypical patient with spontaneous intracranial hypotension presents with orthostatic headaches, has pachymeningeal enhancement on cranial MR imaging, and is treated with an epidural blood patch, as reflected by the revised 2004 diagnostic criteria according to the International Classification of Headache Disorders (ICHD-2).4 However, it has become well established that the spectrum of clinical as well as radiographic manifestations of spontaneous intracranial hypotension is unusually broad,1,5 and this is not reflected by the ICHD-2 criteria. We report a new set of diagnostic criteria for spontaneous spinal CSF leaks and spontaneous intracranial hypotension encompassing its varied clinical and radiographic manifestations. The intent of these criteria is to present a diagnostic scheme that can be used to more reliably diagnose spontaneous spinal CSF leaks and intracranial hypotension.
Methods
On the basis of our experience with spontaneous intracranial hypotension and a comprehensive review of the literature, the following diagnostic criteria were developed (Table 1; Figs. 1, 2).

Postmyelography CTs showing (A) bilateral cervicothoracic CSF leaks without an associated meningeal diverticulum; B, Left thoracic meningeal diverticulum with an associated CSF leak; and C, right thoracic meningeal diverticulum without an associated CSF leak.

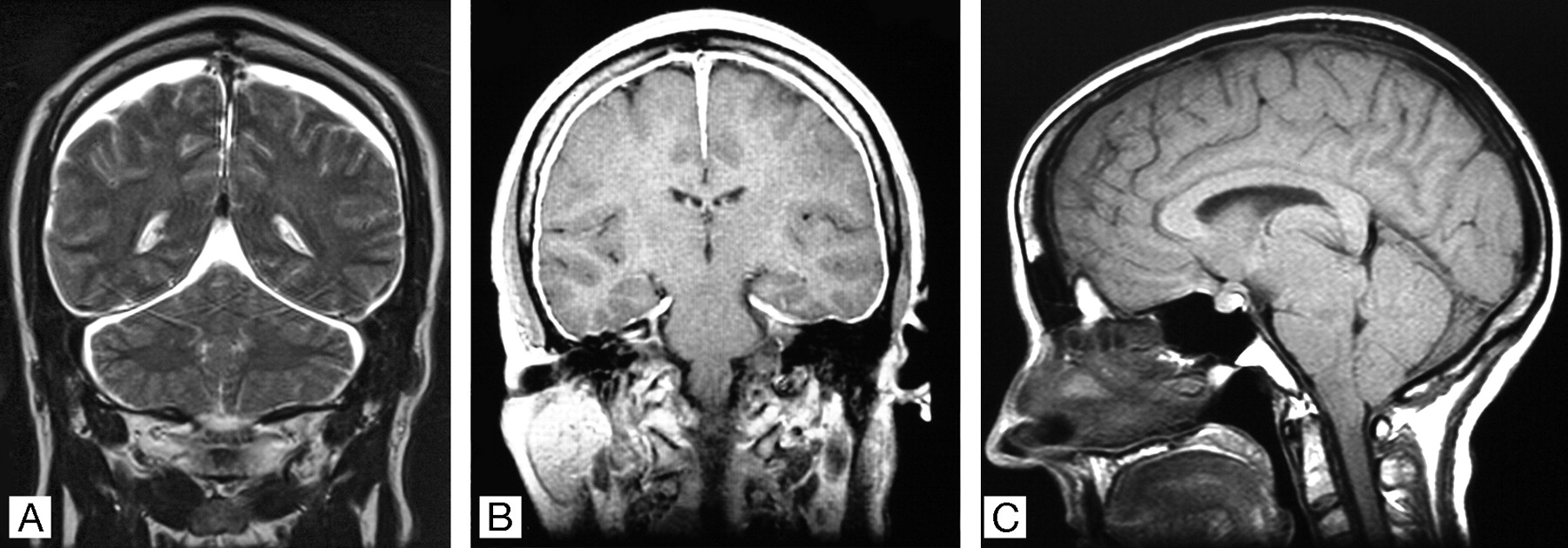
A, Brain MR images showing typical findings in spontaneous intracranial hypotension with a coronal T2-weighted image showing subdural fluid collections; B, a coronal gadolinium-enhanced T1-weighted image showing enhancement of the pachymeninges; and C, a T1-weighted sagittal image showing sagging of the brain.
Diagnostic criteria for spontaneous spinal CSF leak and intracranial hypotension
Criterion A.
The demonstration of a spinal CSF leak on spinal imaging. Imaging modalities may include CT myelography, MR imaging, MR myelography, or radionuclide cisternography and must demonstrate the presence of extrathecal CSF. Indirect evidence for a spinal CSF leak such as early appearance of contrast in the kidney on CT myelography or early uptake of isotope in the bladder and kidneys on radionuclide cisternography is not sufficient to make the diagnosis.
Criterion B, if criterion A not met.
Cranial MR imaging changes of spontaneous intracranial hypotension and at least one of the following: 1) low opening pressure, 2) spinal meningeal diverticulum, or 3) improvement of symptoms after epidural blood patch. A positive MR imaging result is defined as the presence of at least one of the 3 major MR imaging findings of spontaneous intracranial hypotension (ie, subdural fluid collections, enhancement of the pachymeninges, and sagging of the brain). Low opening pressure is defined as less than or equal to 60 mm of water with the patient in the lateral decubitus position. Spinal meningeal diverticula are defined as abnormal dilations of the nerve root sleeve (excluding the commonly observed small lumbosacral perineural cysts).
Criterion C, if criteria A and B not met.
The presence of all of the following or at least 2 of the following if typical orthostatic headaches are present: 1) low opening pressure, 2) spinal meningeal diverticulum, and 3) improvement of symptoms after epidural blood patch.
These diagnostic criteria were applied to a group of consecutive patients evaluated by us between January 1, 2001, and December 31, 2006, for spontaneous spinal CSF leaks and intracranial hypotension.
In our practice, epidural blood patching or conservative treatment consisting of bed rest, oral hydration, and oral caffeine is recommended after cranial MR imaging confirms the clinical suspicion of spontaneous intracranial hypotension. Spinal imaging is recommended if such treatments fail or if cranial MR imaging is normal.
Statistical Analysis
Analysis of variance (ANOVA) was used to compare groups.
Results
During the 6-year period of study, a total of 107 patients were evaluated for spontaneous spinal CSF leaks and intracranial hypotension. None of the patients had a history of lumbar puncture, penetrating spinal trauma, or spinal surgery or procedures. None of the patients had a history of CSF rhinorrhea or CSF otorrhea. A total of 37 patients resided within Los Angeles County, 20 patients resided outside of Los Angeles County but within California, and 50 resided outside of California.
Using the presently described diagnostic criteria, we confirmed the diagnosis in 94 patients and excluded the diagnosis in 13 patients. The mean age at onset of symptoms for these 94 patients (58 women and 36 men; ratio, 1.6:1) was 41.7 years (SD, 12.5 years). Among these 94 patients, all patients had undergone cranial MR imaging, 86 had undergone CT myelography, 4 had undergone spinal MR imaging or MR myelography only, 4 had no spinal imaging performed, 75 had an opening pressure recorded, and 88 had undergone 1 or more epidural blood patches. Clinical and radiographic data are summarized in Table 2. No significant differences were noted in the sex and age distribution among the different groups (P = .2484) or between those meeting and not meeting the diagnostic criteria (P = .6475). Overall, cranial MR imaging results were abnormal in 68 (72%) of 94 patients. Subdural fluid collection was noted in 34 (36%) patients, enhancement of the pachymeninges in 53 (56%) patients, and sagging of the brain in 48 (51%) patients. Spinal imaging showed a CSF leak in 78 (83%) patients and meningeal diverticula in 40 (43%) patients. Meningeal diverticula were located in the thoracic spine in 31 patients, in the cervical spine in 4 patients, and both in 5 patients (2 patients with Marfan syndrome also had lumbar dural ectasia and sacral meningeal diverticula). Opening pressure was low in 70 (93%) of 75 patients with a recorded opening pressure. There were 84 (95%) of 88 patients who responded favorably to an epidural blood patch.
Data on 107 patients evaluated for spontaneous spinal CSF leak and intracranial hypotension
Among the 94 patients who fulfilled the diagnostic criteria, 75 (80%) had a good outcome (ie, complete or near-complete resolution of symptoms), and 19 (20%) had a poor outcome (ie, no or minimal improvement of symptoms). In addition to epidural blood patching in 88 patients, 30 patients underwent percutaneous placement of a fibrin sealant, and 38 patients underwent surgical repair of a CSF leak. In those patients with meningeal diverticula but no demonstrable CSF leak, the largest diverticula were targeted when percutaneous placement of fibrin sealant or surgical treatment was undertaken.
A spinal CSF leak was demonstrated in 78 patients (criterion A) with use of CT myelography or intrathecal gadolinium-enhanced MR imaging (n = 74) or MR imaging or MR myelography only (n = 4). The mean age of the 48 women and 30 men was 40.6 years (SD, 12.5 years; range, 12–61 years). Among these 78 patients, cranial MR imaging was typical of spontaneous intracranial hypotension in 57 patients and normal in 21 patients, opening pressure was low in 60 of 64 patients with a recorded opening pressure, meningeal diverticula were demonstrated in 28 patients, and 72 of 75 patients responded to an epidural blood patch. Extrathecal CSF was confirmed in 31 of 33 patients who underwent surgery.
Eleven patients had an abnormal cranial MR imaging but did not meet criterion A. The mean age of the 7 women and 4 men was 49.2 years (SD, 12.3 years; range, 34–72 years). Four of these patients had no spinal imaging performed but had a low opening pressure (n = 2) or responded to an epidural blood patch (n = 2). Among the 7 patients who did undergo spinal imaging, 7 had meningeal diverticula, 5 of 6 had a low opening pressure, and 5 of 6 responded to an epidural blood patch. Extrathecal CSF was confirmed in both patients who underwent surgery.
Five patients had a normal cranial MR imaging and no demonstrable spinal CSF leak but had a low opening pressure, meningeal diverticula, and responded to an epidural blood patch or had typical orthostatic headaches, a low opening pressure, and responded to an epidural blood patch, thereby satisfying diagnostic criterion C. The mean age of the 3 women and 2 men was 42.8 years (SD, 6.6 years; range, 37–52 years). Extrathecal CSF was confirmed in all 3 patients who underwent surgery.
The diagnosis could not be confirmed in the remaining 13 patients, all of whom had cranial MR imaging, spinal imaging, and a recorded opening pressure. The mean age of the 9 women and 4 men was 43.5 years (SD, 20.3; range, 12–75 years). These patients all presented with headaches that had an orthostatic component. The final diagnosis was “chronic daily headache” or “posttraumatic headache” in most of these patients.
Discussion
Previously, the only set of diagnostic criteria for spontaneous spinal CSF leak and intracranial hypotension were those published by the ICDH-2.4 These ICDH-2 criteria are mainly clinical and rely on the positional features of the headache, the presence of selected associated symptoms, and resolution of symptoms after an epidural blood patch.4 However, it has become well established that the clinical spectrum of spontaneous intracranial hypotension is unusually varied.1,5 An orthostatic headache is the prototypical clinical manifestation of spontaneous intracranial hypotension, but unlike the ICDH-2 criteria, the headache does not invariably occur within 15 minutes of sitting or standing.1 Moreover, many different headache patterns have been reported in spontaneous intracranial hypotension, such as thunderclap headache, nonpositional headache, exertional headache, cough headache, “second-half-of-the-day” headache, and even paradoxic headaches that worsen when lying down, whereas rarely there is no history of headache.1,5–10 Several associated symptoms have been reported in spontaneous intracranial hypotension, occasionally predominating the clinical picture (eg, dementia,11 quadriplegia,10 or coma).12–14 The clinical spectrum has not yet been fully defined, and new manifestations continue to be added.10,15,16 The current set of diagnostic criteria allows for the wide and continuously expanding clinical and radiographic spectrum of the disease. The main clinical component of the diagnostic criteria is improvement of symptoms after epidural blood patching. The placement of an epidural blood patch is the most commonly used initial treatment technique for spontaneous intracranial hypotension, and most patients react favorably to an epidural blood patch, even if only temporarily.1,17,18 The improvement in symptoms after an epidural blood patch is not limited to positional headaches but also includes other types of headache, as well as the associated symptoms, including coma.6–14 However, most patients require 2 or more epidural blood patches, and improvement may be suboptimal. Resolution of symptoms within 72 hours of epidural blood patching, an obligatory criterion in the ICDH-2 criteria, is not the norm.
The demonstration of a spinal CSF leak (ie, the presence of extrathecal CSF) is sufficient to diagnose spontaneous intracranial hypotension, regardless of associated symptoms, imaging findings, or results of lumbar puncture and epidural blood patching. CT myelography is the study of choice to detect the CSF leak and is more reliable than radionuclide cisternography,1,19 but noninvasive imaging such as spinal MR imaging20 or MR myelography21 also may demonstrate evidence for extrathecal CSF.
Cranial MR imaging has revolutionized our understanding of spontaneous intracranial hypotension and is an important component of the current diagnostic criteria. Characteristic findings consist of subdural fluid collections, enhancement of the pachymeninges, engorgement of venous structures, pituitary hyperemia, and sagging of the brain (mnemonic, SEEPS).1 Of these 5 findings, only subdural fluid collections, enhancement of the pachymeninges, and sagging of the brain are reliably demonstrated on the initial MR imaging examination, whereas engorgement of venous structures and pituitary hyperemia are often not apparent until compared with a posttreatment MR imaging examination. A diagnosis of spontaneous intracranial hypotension with use of the current criteria can be made without any spinal imaging or lumbar puncture, in the common clinical scenario of a positive cranial MR imaging and symptoms responsive to epidural blood patching. Abnormal MR imaging results, particularly the enhancement of the pachymeninges, have been considered to be the sine qua non of spontaneous intracranial hypotension,22 but it has become well established that a sizeable minority of patients (28% in our study) have normal results on brain MR imaging.1,18 If a patient suspected of spontaneous intracranial hypotension has a normal brain MR imaging result and no CSF leak on spinal imaging, a confirmatory diagnosis can still be made with the diagnostic criteria on the basis of a low opening pressure, the presence of spinal meningeal diverticula, and resolution of symptoms after an epidural blood patch. Although this diagnostic category may seem to be less robust, surgical exploration of the spinal meningeal diverticula confirmed the presence of a CSF leak in all 3 such treated patients in this category. All meningeal diverticula were located in the thoracic or cervical spine and none in the lumbosacral spine (except for those with Marfan syndrome). Although some patients with confirmed spinal CSF leaks may have opening pressures that are consistently within the range of normal,19,23 opening pressure is low in most patients (93% in our study). Before the advent of modern imaging, low opening pressure was the only available confirmatory test.24,25
With use of the current set of diagnostic criteria, the diagnosis could not be confirmed in one eighth of patients suspected of a spontaneous spinal CSF leak. It can be postulated that, at least in some of these patients, intermittent or small CSF leaks exist below the level of detection of current imaging capabilities or that low CSF volume is because of inadequate CSF production.
Additional studies are required to determine the clinical applicability of the proposed criteria in different patient populations.
Conclusions
We report a new set of diagnostic criteria for spontaneous spinal CSF leaks and intracranial hypotension encompassing its varied clinical and radiographic manifestations.
References
- Received June 20, 2007.
- Accepted after revision November 11, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Diffuse Calvarial Hyperostosis and Spontaneous Intracranial Hypotension: A Case-Control Study
- Renal Excretion of Contrast on CT Myelography: A Specific Marker of CSF Leak
- A two-level large-volume epidural blood patch protocol for spontaneous intracranial hypotension: retrospective analysis of risk and benefit
- The Interpeduncular Angle: A Practical and Objective Marker for the Detection and Diagnosis of Intracranial Hypotension on Brain MRI
- Quantitative Measurement of CSF in Patients with Spontaneous Intracranial Hypotension
- False localizing sign of cervico-thoracic CSF leak in spontaneous intracranial hypotension
- Bariatric surgery as a possible risk factor for spontaneous intracranial hypotension
- Large-Volume Blood Patch to Multiple Sites in the Epidural Space through a Single-Catheter Access Site for Treatment of Spontaneous Intracranial Hypotension
- Spinal Meningeal Diverticula in Spontaneous Intracranial Hypotension: Analysis of Prevalence and Myelographic Appearance
- Distant Subdural and Epidural Hematomas: A Case Report
- CT-Guided Epidural Blood Patching of Directly Observed or Potential Leak Sites for the Targeted Treatment of Spontaneous Intracranial Hypotension
- An episode of cerebrospinal fluid leak syndrome involving a marathon runner
- Diffuse Pachymeningeal Enhancement and Subdural and Subarachnoid Space Opacification on Delayed Postcontrast Fluid-Attenuated Inversion Recovery Imaging in Spontaneous Intracranial Hypotension: Visualizing the Monro-Kellie Hypothesis
- Postpuncture CSF leakage: A potential pitfall of radionuclide cisternography