
Abstract
BACKGROUND AND PURPOSE: In the chronic phase after traumatic brain injury, DTI findings reflect WM integrity. DTI interpretation in the subacute phase is less straightforward. Microbleed evaluation with SWI is straightforward in both phases. We evaluated whether the microbleed concentration in the subacute phase is associated with the integrity of normal-appearing WM in the chronic phase.
MATERIALS AND METHODS: Sixty of 211 consecutive patients 18 years of age or older admitted to our emergency department ≤24 hours after moderate to severe traumatic brain injury matched the selection criteria. Standardized 3T SWI, DTI, and T1WI were obtained 3 and 26 weeks after traumatic brain injury in 31 patients and 24 healthy volunteers. At baseline, microbleed concentrations were calculated. At follow-up, mean diffusivity (MD) was calculated in the normal-appearing WM in reference to the healthy volunteers (MDz). Through linear regression, we evaluated the relation between microbleed concentration and MDz in predefined structures.
RESULTS: In the cerebral hemispheres, MDz at follow-up was independently associated with the microbleed concentration at baseline (left: B = 38.4 [95% CI 7.5–69.3], P = .017; right: B = 26.3 [95% CI 5.7–47.0], P = .014). No such relation was demonstrated in the central brain. MDz in the corpus callosum was independently associated with the microbleed concentration in the structures connected by WM tracts running through the corpus callosum (B = 20.0 [95% CI 24.8–75.2], P < .000). MDz in the central brain was independently associated with the microbleed concentration in the cerebral hemispheres (B = 25.7 [95% CI 3.9–47.5], P = .023).
CONCLUSIONS: SWI-assessed microbleeds in the subacute phase are associated with DTI-based WM integrity in the chronic phase. These associations are found both within regions and between functionally connected regions.
ABBREVIATIONS:
- B
- linear regression coefficient
- Bcmb-conc
- linear regression coefficient with microbleed concentration as independent variable
- Bcmb-nr
- linear regression coefficient with microbleed number as independent variable
- MD
- mean diffusivity
- MDz
- Z-score of mean diffusivity, normalized to the healthy control participants
- t1
- 3 (2–5) weeks after TBI
- t2
- 26 (25–28) weeks after TBI
- TAI
- traumatic axonal injury
- TBI
- traumatic brain injury
- FA
- fractional anisotropy
- MARS
- Microbleed Anatomical Rating Scale
- GCS
- Glasgow Coma Scale
The yearly incidence of traumatic brain injury (TBI) is around 300 per 100,000 persons.1,2 Almost three-quarters of patients with moderate to severe TBI have traumatic axonal injury (TAI).3 TAI is a major predictor of functional outcome,4,5 but it is mostly invisible on CT and conventional MR imaging.6,7
DTI provides direct information on WM integrity and axonal injury.5,8 However, DTI abnormalities are neither specific for TAI nor stable over time. Possibly because of the release of mass effect and edema and resorption of blood products, the effects of concomitant (non-TAI) injury on DTI are larger in the subacute than in the chronic phase (>3 months).4,9,10 Therefore, DTI findings are expected to reflect TAI more specifically in the chronic than in the subacute phase (1 week–3 months).4 Even in regions without concomitant injury, the effects of TAI on DTI are dynamic, possibly caused by degeneration and neuroplastic changes.6,11,12 These ongoing pathophysiological processes possibly contribute to the emerging evidence that DTI findings in the chronic phase are most closely associated with the eventual functional outcome.12,13
Although DTI provides valuable information, its acquisition, postprocessing, and interpretation in individual patients are demanding. SWI, with which microbleeds can be assessed with high sensitivity, is easier to interpret and implement in clinical practice. In contrast to DTI, SWI-detected traumatic microbleeds are more stable1 except in the hyperacute14,15 and the late chronic phases.16 Traumatic cerebral microbleeds are commonly interpreted as signs of TAI. However, the relation is not straightforward. On the one hand, nontraumatic microbleeds may be pre-existing. On the other hand, even if traumatic in origin, microbleeds represent traumatic vascular rather than axonal injury.17 Indeed, TAI is not invariably hemorrhagic.18 Additionally, microbleeds may secondarily develop after trauma through mechanisms unrelated to axonal injury, such as secondary ischemia.18
DTI is not only affected by pathophysiological changes but also by susceptibility.19 The important susceptibility-effect generated by microbleeds renders the interpretation of DTI findings at the location of microbleeds complex. In the chronic phase, mean diffusivity (MD) is the most robust marker of WM integrity.4,6 For these reasons, we evaluated MD in the normal-appearing WM.
Much TAI research focuses on the corpus callosum because it is commonly involved in TAI5,18,20 and it can reliably be evaluated with DTI,5,21 and TAI in the corpus callosum is related to clinical prognosis.6,20 The corpus callosum consists of densely packed WM tracts that structurally and functionally connect left- and right-sided brain structures.22 The integrity of the corpus callosum is associated with the integrity of the brain structures it connects.23 Therefore, microbleeds in brain structures that are connected through the corpus callosum may affect callosal DTI findings. Analogous to this, microbleeds in the cerebral hemispheres, which exert their function through WM tracts traveling through the deep brain structures and brain stem,24,25 may affect DTI findings in the WM of the latter.
Our purpose was to evaluate whether the microbleed concentration in the subacute phase is associated with the integrity of normal-appearing WM in the chronic phase. We investigated this relation within the cerebral hemispheres and the central brain and between regions that are functionally connected by WM tracts.
MATERIALS AND METHODS
We report a retrospective interpretation of prospectively collected data within an observational follow-up cohort study in consecutive patients with moderate to severe TBI and healthy volunteers, approved by Radboud university medical center institutional review board. All healthy volunteers and patients or their next of kin gave written informed consent.
Study Design and Research Questions
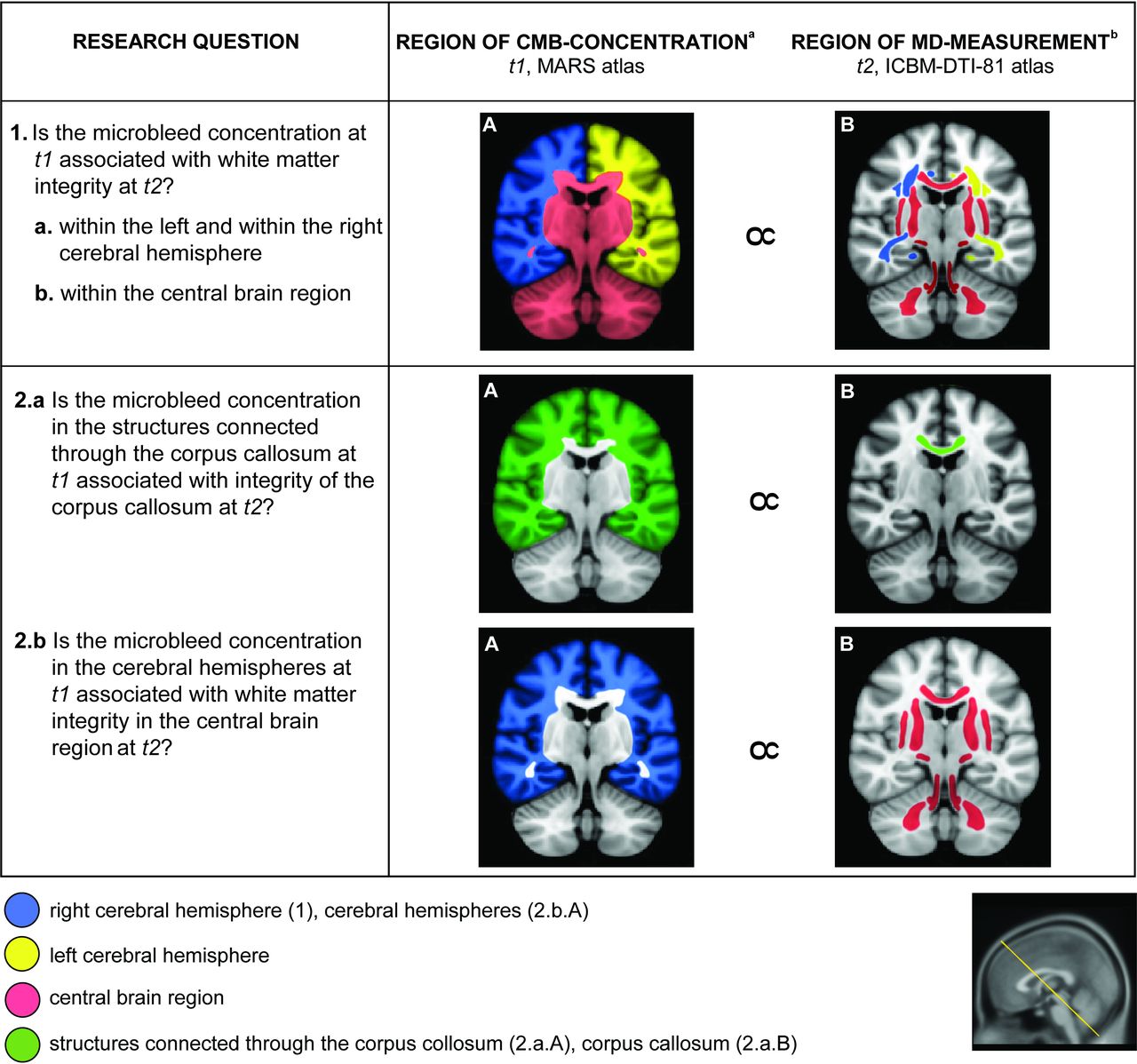
We evaluated whether the microbleed concentration (number of microbleeds per cm3) detected with SWI in the subacute phase of TBI is correlated with MD of normal-appearing WM in the chronic phase. MD was measured in the normal-appearing WM after the exclusion of abnormalities based on an SWI-based mask drawn for each patient. The research questions are specified in the Figure.

Study design and research questions. Images are oblique coronal sections of the Montreal Neurological Institute brain, illustrating the regions evaluated for each research question (image plane illustrated in the thumbnail image in the right lower corner). aNumber of microbleeds per cm3 brain tissue. bZ-score of mean diffusivity. t1 indicates Moment of SWI-acquisition, i.e. 3 (2–5) weeks after TBI; t2, Moment of DTI-acquisition, i.e. 26 (25–28) weeks after TBI; MARS atlas, Microbleed Anatomical Rating Scale atlas27; ICBM-DTI-81 atlas, the ICBM-DTI-81 white matter labels atlas designed by Mori S et al.28
Patient Selection and MR Acquisition
All 211 consecutive patients 18 years of age or older having sustained a moderate to severe TBI ≤24 hours before presenting at our level I trauma center emergency department were prospectively screened for the exclusion criteria specified in the Online Supplemental Data. Details of the patient selection process are described in the Online Supplemental Data. Finally, this yielded SWI, DTI, and T1WI data for 31 patients, obtained median 3 (interquartile range 2–5 [t1]) and median 26 (interquartile range 25–28 [t2]) weeks after TBI using a standardized trauma protocol on a single 3T MR imaging scanner (Magnetom Trio, Siemens). The Online Supplemental Data summarize the parameters of the relevant MR imaging sequences.
Patient characteristics are summarized in the Online Supplemental Data.
Healthy Volunteers
To increase generalizability and facilitate interpretation, we normalized the patients' MD values to those of 24 healthy volunteers, scanned on the same MR imaging scanner with equal acquisition parameters, and recruited as described in the Online Supplemental Data. The section “DTI Processing” below describes the normalization procedure.
Microbleed Anatomical Rating Scale Atlas
We manually segmented the standard brain in Montreal Neurological Institute space26 into the regions specified in the Microbleed Anatomical Rating Scale (MARS) scoring template.27 We defined the following compound regions: 1) cerebral hemispheres (left, right, and bilateral), 2) central brain region, and 3) structures connected through the corpus callosum. See the Online Supplemental Data for details and definitions of these compound regions.
Microbleed Evaluation
We detected microbleeds and allocated them to MARS regions as described in the Online Supplemental Data. As recommended,27 we performed our analyses on definite microbleeds only. Per patient, we calculated the microbleed concentration (cm−3) within each anatomic region as the number of microbleeds divided by the volume of the region under investigation on the T1-weighted scan at t1 (cm3).
Creation of Susceptibility Mask
To rule out bias caused by the effect of susceptibility on DTI findings,19 we created individual exclusion masks, eliminating from the DTI measurements any potential source of susceptibility related to trauma and its clinical management. See the Online Supplemental Data for details.
DTI Processing
We extracted MD values from the normal-appearing WM of the following compound regions: 1) cerebral hemispheres, 2) central brain region, and 3) corpus callosum based on the ICBM-DTI-81 WM labels atlas designed by Mori et al.28 Definitions of these compound regions and details of the DTI processing procedure are described in the Online Supplemental Data. Regional MDs were calculated for each patient and healthy volunteer as the averaged MD within each region, and the Z score of MD (MDz) of each region was calculated as:
 in which MDp is the patient's MD, MDv is the mean MD of the healthy volunteers, and SDMDv is the standard deviation of the healthy volunteers' MD.
in which MDp is the patient's MD, MDv is the mean MD of the healthy volunteers, and SDMDv is the standard deviation of the healthy volunteers' MD.
Blinding
The persons processing (T.v.d.H., B.P.) and interpreting the SWI data (A.v.d.E., B.M.G.) had no access to clinical information nor DTI results. V.P., who processed the DTI data, had no access to clinical information nor to microbleed counts.
Statistical Analysis
Data were analyzed by P.V. (statistician) and A.v.d.E. using SPSS 25 statistical software (IBM).
We used 2-sample t-tests to test differences in MDz between patients and healthy volunteers.
We used linear regression analyses to examine the relation between the microbleed concentration and MDz, as specified in the Figure. We adjusted for sex, age at the day of DTI, and time passed from TBI to DTI acquisition (Table, multivariable model). Because the severity of TBI is associated with both microbleeds17 and MD,3 it could confound the association between microbleeds and MD. Therefore, we adjusted the analyses for the Glasgow Coma Scale (GCS) score at the injury site (research question 2: Online Supplemental Data; research question 1: results described in the text). Because microbleed concentrations in different regions of the same brain may covary, the associations in research question 2 could be confounded by the microbleed concentration in the region of MD measurement. Therefore, we adjusted the analyses for the microbleed concentration in the region of MD measurement (Online Supplemental Data).
Association between microbleed concentrations at t1 and MDz at t2
To facilitate clinical implementation of our findings, in addition to the linear regression coefficients for microbleed concentration (Bcmb-conc), we also present the linear regression coefficients for microbleed number (Bcmb-nr). These 2 coefficients can be interpreted as follows: with each increase of the microbleed concentration by 1/cm3, MDz increases with Bcmb-conc, but with each additional microbleed, MDz increases with Bcmb-nr.
Differences with P < .05 were considered significant. Continuous variables are presented as median (interquartile range). Categoric variables are presented as number (%). Regression coefficients are presented as linear regression coefficient (95% CI).
For a detailed description of the statistical procedures, please refer to the Online Supplemental Data.
As discussed earlier, we chose MD as the DTI variable of interest. To facilitate comparison with other papers, we performed the same analyses with the more frequently reported fractional anisotropy (FA). Please refer to the Online Supplemental Data for the results.
RESULTS
At t1, the 31 patients had a total of 856 microbleeds (median 24 [interquartile range, 14–35] per patient), anatomically distributed as shown in Supplemental Online Table A4. MDz at t2 was higher in patients than in healthy volunteers (Supplemental Online Table A4).
Associations within Regions (Research Question 1)
Within both of the cerebral hemispheres, MDz at t2 was positively associated with the microbleed concentration at t1 (Table and Online Supplemental Data). This association was independent of sex, age, and time passed from TBI to DTI acquisition (Table). It was also independent of GCS score at the injury site (Bcmb-conc 30.3 [95% CI 11.5–49.1, P = .003] and 36.3 [95% CI 8.8–63.7, P = .011] for microbleed concentration in the right and left cerebral hemisphere, respectively, in bivariable linear regression corrected for GCS score). Within the central brain region, MDz was not associated with the microbleed concentration (Table and Online Supplemental Data).
Associations between Connected Regions (Research Question 2)
MDz in the corpus callosum at t2 was positively associated with the microbleed concentration in the structures connected through the corpus callosum at t1 (Table and Online Supplemental Data) even after correction for the microbleed concentration in the corpus callosum itself (Online Supplemental Data). The 95% CIs of Bcmb-conc in these 2 regions did not overlap (Online Supplemental Data).
MDz in the central brain region was positively associated with the microbleed concentration at t1 in the cerebral hemispheres (Table and Online Supplemental Data) even after correction for the microbleed concentration in the central brain region itself (Online Supplemental Data).
All of these associations were independent of GCS score, sex, age, and time passed from TBI to DTI acquisition (Table, Online Supplemental Data).
See the Online Supplemental Data for the results of the equivalent analyses with FA.
DISCUSSION
We have shown that as early as the subacute phase of TBI, microbleeds are predictors of the integrity of normal-appearing WM in the chronic phase. Microbleeds are not only predictive of WM integrity in the same region but also of WM integrity in functionally connected regions.
To our knowledge, this is the first study to address the association between microbleeds detected early with SWI and later DTI findings in normal-appearing WM in consecutive patients with moderate to severe TBI.
Our findings are based on more microbleeds than the 3 previous studies on the relation between traumatic microbleeds and DTI. Whereas our patients had a total of 856 microbleeds, occurring in 30 patients (1 patient had no microbleeds), the patients reported previously had only 97–138 microbleeds,29,30 occurring in 14 and 29 patients,29,30 or an unreported number of microbleeds, occurring in 8 patients.31 The relatively large amount of microbleeds allowed us to correct for possible interfering factors such as age, sex, GCS score, and time passed from TBI to DTI acquisition.
The interpretation of our results is facilitated by the use of microbleed concentrations and normalized MD values, which enhance uniformity between regions with different volumes and reference MD values. In contrast, previous groups quantified their microbleed data using dichotomized,31 ordinal,29 or absolute microbleed numbers in regions of varying volume30 and used absolute values of the DTI variables.29⇓-31
The inclusion of DTI findings inside the microbleeds29,31 by previous authors may have introduced possible confounding by the effects of susceptibility on DTI findings.19 Two of the previous studies detected microbleeds with a less sensitive technique.29,31 Previous authors evaluated SWI and DTI simultaneously at widely varying time points after TBI30 or defined less clearly the timing of microbleed detection.31 They defined their inclusion criteria less clearly30,31 or the severity of TBI differed from our patients.30
Relation between Microbleeds and WM Integrity within the Cerebral Hemispheres
Within both of the cerebral hemispheres, WM integrity in the chronic phase is predictive of the microbleed concentration in the subacute phase. This prediction is independent of GCS score, sex, age, and time passed from TBI to DTI acquisition. Although our data do not allow evaluation of the causality of this association, our findings support the assessment of microbleeds in daily practice because microbleeds are easier to evaluate in a clinical setting than DTI, especially in the subacute phase. The relation we found between microbleeds and WM integrity is consistent with autopsy studies showing that MR imaging–detected microbleeds are related to axonal necrosis,32 and anatomopathologic microbleeds are related to axonal injury.33
Compatible with our findings, the 2 previous longitudinal MR imaging studies found a lower FA in patients with microbleeds31 and inside callosal and cerebral hemispheric microbleeds.29 In contrast to the association we found between microbleeds and MD in the cerebral hemispheres, Toth et al30 found no such association within the subcortical WM. On the one hand, this suggests a relation between cortical microbleeds and integrity of the underlying WM. On the other hand, the apparent difference between their and our findings may partly rely on methodologic differences, such as the different and widely varying timing of their scans, the small number of microbleeds and of patients with microbleeds, and the wide range of trauma severity.30
Relation between Microbleeds and WM Integrity in Connected Regions
We have shown that microbleeds are predictive of WM abnormality in functionally connected regions: microbleeds in structures connected by WM tracts running through the corpus callosum are predictive of the integrity of the corpus callosum, and microbleeds in the cerebral hemispheres are predictive of the integrity of the central brain region.
Our findings suggest that the integrity of WM is not only determined by nearby primary traumatic lesions but can also be affected by distant traumatic lesions. Indeed, the distant relation described earlier is independent of the microbleeds in the corpus callosum and the central brain region themselves. The integrity of the corpus callosum is even more strongly predicted by microbleeds in the connected regions than by local microbleeds in the corpus callosum itself. Analogous to this, in the central brain, the size of the regression coefficients suggests a stronger association of abnormality with microbleeds in the cerebral hemispheres than with microbleeds in the central brain, though the difference is not statistically significant. The distant effect of microbleeds could be an expression of degradation within neural networks at distance of the primary injury,18 such as the thalamocortical and pontothalamocortical deafferentiation observed in patients with TBI.24 It could be mediated by the axons or vessels involved in the primary injury, either by functional deprivation of the corpus callosum and the central brain, respectively or by biochemical changes within the long axons or perivascular spaces.17
Consistent with our findings, Kumar et al31 found a decreased MD in the corpus callosum only in the patients with microbleeds, which were all outside the corpus callosum, and a normal MD in the patients without microbleeds. Like us, Toth et al30 found no local effect of microbleeds within the corpus callosum on callosal integrity. Unlike us, they found no association between microbleeds in the subcortical WM and integrity of the normal-appearing callosal tissue. The methodologic differences discussed earlier may have contributed to this lack of association.30
Limitations
A potential bias results from the manual delineation of the microbleeds and concomitant injury.
The limited number of patients did not allow us to assess the potential prognostic value of microbleed concentration or of MDz measurements.
Inherent to TBI research, the effects of injury severity and concomitant intracranial injury on MD are difficult to disentangle from the microbleeds' effects. To minimize these effects, we included GCS score in our analyses and measured MD outside any concomitant lesions using the susceptibility mask.
Implications and Future Perspectives
We have shown that as early as the subacute phase of TBI, microbleeds inform us on the expected integrity of normal-appearing WM in the chronic phase and that this relation differs between regions. The evidence of the prognostic value of DTI in the chronic phase is growing,6,13 but in the subacute phase, DTI has less robust prognostic value, possibly because of the more dynamic and heterogeneous pathophysiologic mechanisms influencing DTI findings in that phase.6,11 The evidence for the prognostic value of traumatic microbleeds is limited.17 Our findings encourage a shift in the search for the prognostic value of microbleeds to the use of their regional distribution and their concentration instead of their number and a shift of attention to early prognostication when microbleeds have the clear advantage of stability over DTI.
The different relations we found between microbleeds and MD and FA, respectively, may indicate that not only chronic encephalopathic degeneration34 but also earlier stages of distant effects of traumatic lesions develop in a centripetal way. The timing of DTI-evaluation in our study is at the border between the subacute and the chronic stage. At that transitional stage, the peripheral brain may already be entering the chronic stage, but the central brain is still in the subacute phase. This hypothesis should be tested in further studies.
CONCLUSIONS
Whereas DTI interpretation is complex in the subacute phase of TBI, microbleeds assessed with SWI in the subacute phase proved to be predictive of DTI abnormalities of the normal-appearing WM in the chronic phase. Associations are not only found within regions but also between functionally connected regions. The latter are independent of the local microbleed concentration and GCS score, indicating that microbleeds may exert effects at a distance.
ACKNOWLEDGMENTS
We thank TMJC Andriessen, psychologist at Saffier, Den Haag, for her contribution to the collection of data. We thank D Hasboun, PhD, neurologist and anatomist at Université Pierre et Marie Curie, Paris, for his support in selection and definition of functionally relevant compound regions of interest. We thank SC van de Leemput, data and information scientist at Radboudumc, Nijmegen, for providing the software we used for manual adjustments of the susceptibility mask. We also thank FL van der Panne, medical photographer at Erasmus MC, Rotterdam, and K Koschmieder, PhD, student traumatic imaging analysis at Radboudumc, for their help with figure design. Last, we thank Stichting Fonds Catharine van Tussenbroek for the travel grant that facilitated our international collaboration.
Footnotes
This is an investigator-initiated study supported by Trauma Regio Oost, Radboudumc, Nijmegen, and by Stichting Fonds Catharine van Tussenbroek (travel grant). The funding organizations did not participate in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, and approval of the manuscript; and the decision to submit the manuscript for publication.
Disclosures: Anke van der Eerden—RELATED: Grant: Trauma Regio Oost, Radboudumc, Nijmegen, The Netherlands, Comments: Investigator-initiated study supported by Trauma Regio Oost, Radboudumc, Nijmegen. The funding organization did not participate in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, and approval of the manuscript; and the decision to submit the manuscript for publication*; Support for Travel to Meetings for the Study or Other Purposes: Stichting Fonds Catharine van Tussenbroek, Comments: Partial reimbursement of travel expenses from Nijmegen to Paris to facilitate our collaboration. The funding organization did not participate in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, and approval of the manuscript; and the decision to submit the manuscript for publication; UNRELATED: Employment: Erasmus Medical Center, Comments: clinical neuroradiologist and head and neck radiologist. Louis Puybasset— UNRELATED: Stock/Stock Options: BrainTale co-founder. *Money paid to institution.
References
- Received September 29, 2020.
- Accepted after revision November 16, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.