
Abstract
Summary: We correlated MR images with histologic findings in two autopsy-proven cases of chronic hepatic encephalopathy. Cortical hyperintensities on T2-weighted images histologically revealed pseudolaminar spongy degeneration in the deep layers of the cerebral cortices and hyperintensities in the cerebral white matters showed tissue rarefaction associated with loss of myelin and axons but without reactive astrocytosis. Both lesions were considered to be caused by chronic hepatic encephalopathy.
Hepatic encephalopathy is a complication of hepatic failure or portosystemic shunt surgery. Clinical features include confusion, which is often associated with a flapping tremor, drowsiness, stupor, and coma. Repeated episodes of hepatic encephalopathy may lead to neuropsychiatric disturbances, dysarthria, ataxia, and choreoathetosis (1). Pathologically, brain edema without inflammatory infiltration is characteristic of an acute stage, whereas Alzheimer type II astrocytes, which have large pale nuclei with marginated chromatin and scanty cytoplasm, in the gray matter and pseudolaminar spongy degeneration in the deep layers of the cerebral cortices are characteristic findings in the chronic stage (2). The Alzheimer type II astrocytes are largely due to hyperammonemia, which is probably also directly or indirectly responsible for neuronal damage, although the pathogenesis of hepatic encephalopathy is not fully elucidated (3, 4).
Hyperintensities in the bilateral globi pallidi on T1-weighted images have been established as a characteristic finding on MR images in chronic hepatic encephalopathy (5). MR spectroscopy has been available for detecting specific biochemical alterations, which consist of the increase in cerebral glutamine and glutamamate (Glx) and the decrease in myoinositol (mI) and choline (Cho) metabolites in chronic hepatic encephalopathy (6). A few MR imaging studies have described brain swelling and diffuse cortical lesions in acute hepatic encephalopathy (7, 8). There has so far been no report studying the correlation of MR images with histologic findings in patients with chronic hepatic encephalopathy. We studied MR-pathologic correlations with a focus on hyperintensities on the antemortem and postmortem T2-weighted images and their histologic findings in two autopsy-proven cases of chronic hepatic encephalopathy.
Case 1
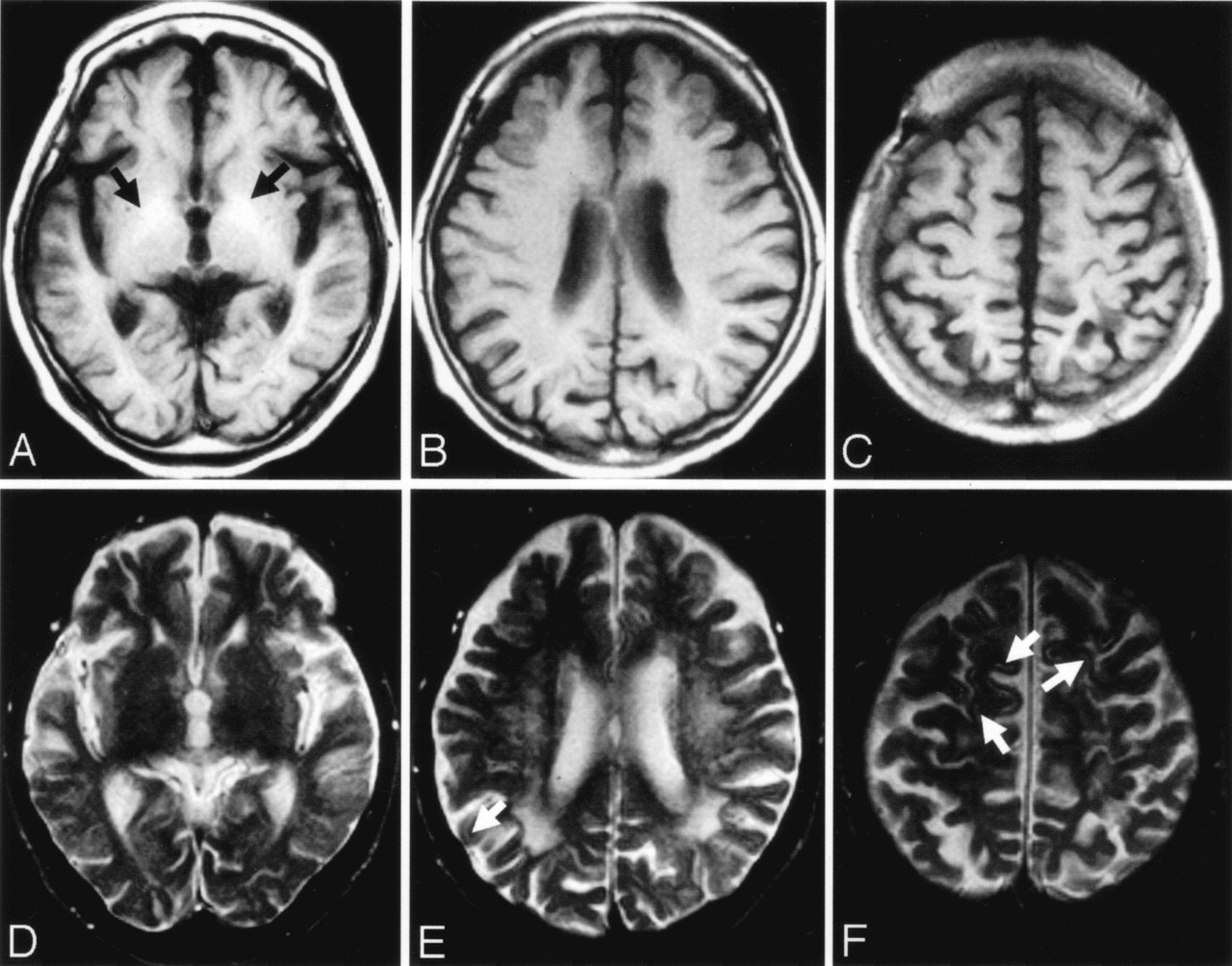
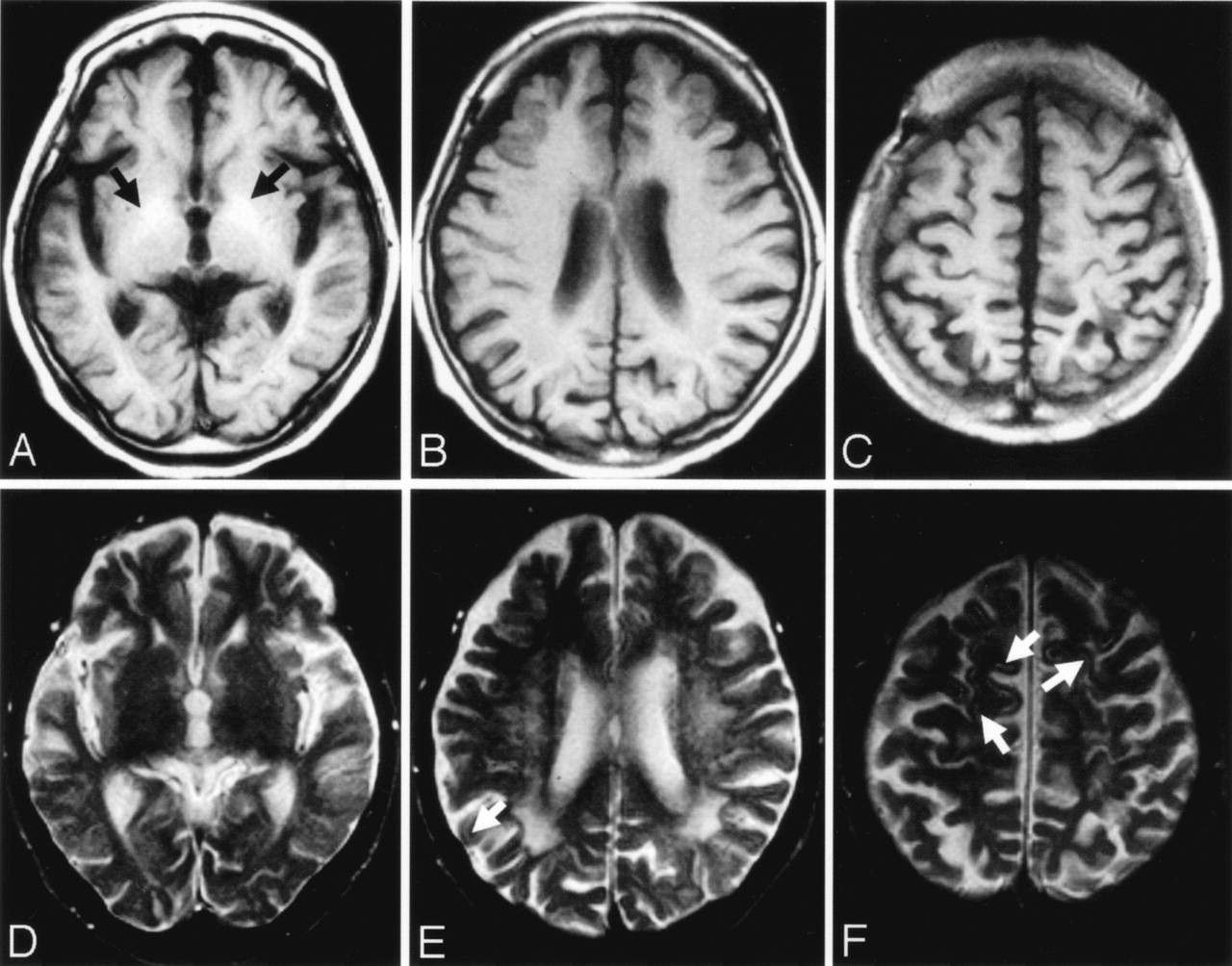
The patient was a 75-year-old woman. Family history was unremarkable for neuropsychiatric disease. At the age of 56 years, she suffered atonic seizure, gait instability, and intention tremor. At ages 66 and 72 years, she developed disturbance of consciousness and was admitted to the hospital, but her symptoms soon subsided without treatment. MR images obtained when the patient was 72 years of age showed hyperintensities in the bilateral globi pallidi on T1-weighted images and slight hyperintensities in some cerebral cortices, as well as confluent and diffuse hyperintensities in the deep and subcortical cerebral white matter on T2-weighted images (Fig 1A–F). Seven months later, she was readmitted to the hospital because of disorientation. Laboratory examinations showed marked hyperammonemia (227 μg/dL; normal range, 30–60 μg/dL). Electroencephalography (EEG) revealed triphasic wave. Her condition was diagnosed as chronic hepatic encephalopathy. Over the next 3 years, she had repeated disturbance of consciousness and disorientation, and she responded less positively to treatment. She died of respiratory failure at the age of 75 years. The total duration from the onset of hepatic encephalopathy to her death was 19 years.
Case 1.
A–C, Axial T1-weighted MR images obtained 2 days after admission. T1-weighted image (A) shows hyperintensities in the globus pallidus on both sides (arrows). T1-weighted images show no definite signal intensity changes in the cerebral cortices (A–C).
D–F, T2-weighted MR images obtained 2 days after admission. Signal intensity abnormalities are difficult to discern on T2-weighted image (D). T2-weighted images (E and F) show focal, faint hyperintensities in the cerebral cortices (arrows). Confluent and diffuse T2 hyperintensities are seen in the deep and subcortical cerebral white matters (E).
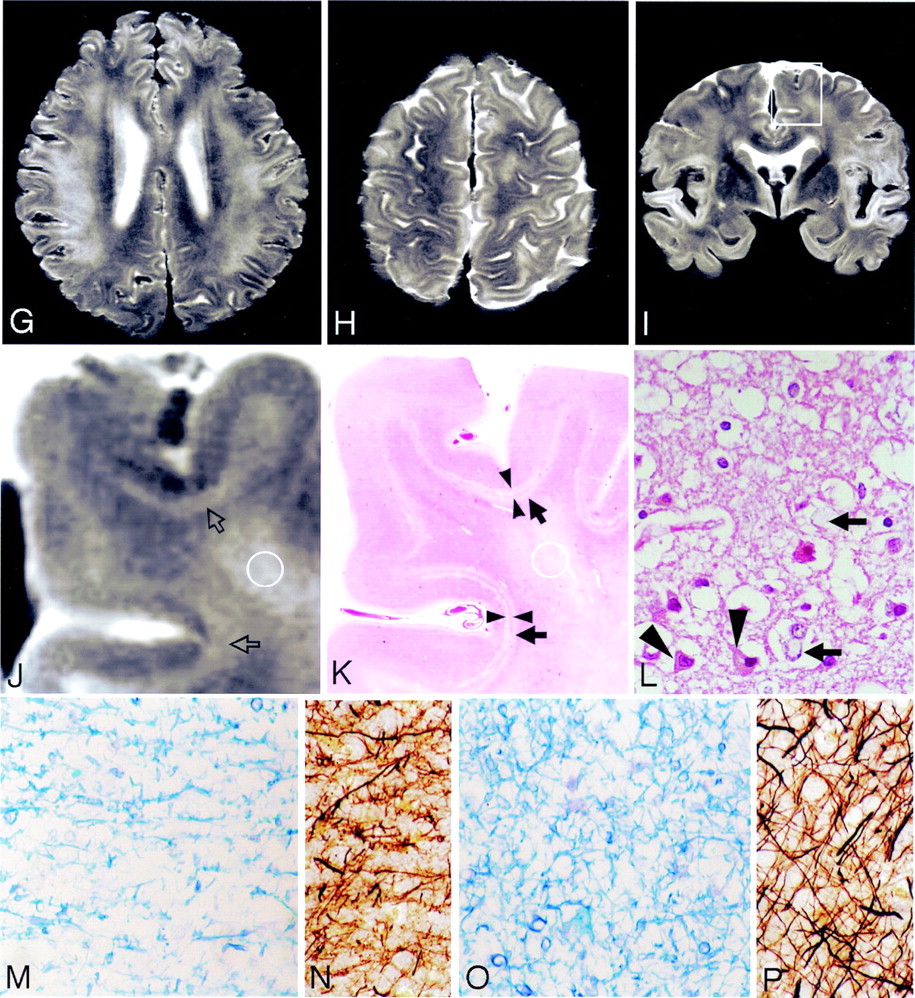
G and H, Postmortem axial T2-weighted MR images show deep cortical and subcortical laminar hyperintensities in the entire cerebral hemisphere. Diffuse T2 hypertensities are seen in the deep and subcortical cerebral white matters (G).
I and J, Coronal T2-weighted MR images show deep cortical and subcortical laminar hyperintensities in the entire cerebral hemisphere. Hyperintensities are also seen in the deep and subcortical white matters (J). Boxed area in panel I shows hyperintensities in the deep layers of the cerebral cortices and subcortical white matters (open arrows) as well as deep cerebral white matter. The boundary between deep layers of the cerebral cortex and subcortical white matter is not clear.
K, The hematoxylin and eosin stained section corresponding to panel J shows laminar pallor of the deep layers of the cerebral cortex (arrowheads) and laminar pallor of the underlying U-fibers (arrows), as well as moderate pallor of the deep cerebral white matter. (Hematoxylin and eosin stain ×100.)
L, Histologic findings of the arrowhead area in panel K shows spongy changes of the neuropil, pyknotic, and shrunken neurons (arrowheads) and Alzheimer type II astrocytes (arrows), which have large pale nuclei with marginated chromatin and scanty cytoplasms. (Hematoxylin and eosin stain ×100.)
M and N, Histologic findings of the U-fibers (K, arrows) show tissue rarefaction and severe loss of myelin (M) and axons (N). (M, Klüver-Barrera stain ×100; N, Bielschowsky stain ×100.)
O and P, Histologic findings of the circled area in panels J and K reveals moderate loss of myelin (O) and axons (P). (O, Klüver-Barrera stain ×100; P, Bielschowsky stain ×100.)
Autopsy was limited to the brain and liver. The liver, weighing 650 g after fixation, revealed fatty cirrhosis. The brain, weighing 1100 g after fixation, showed slight cerebral atrophy. Histologic examination showed numerous Alzheimer type II astrocytes in the cerebral cortices, putamen, caudate nucleus, globus pallidus, thalamus, and cerebellar dentate nucleus as well as in the substantia nigra and inferior olivary nucleus. Pseudolaminar spongy degeneration was found in the deep layers of cerebral cortices and the underlying U-fibers. Neurons were pyknotic and shrunken in the cerebral cortices, but those in the Ammon’s horns were well preserved. There was tissue rarefaction with moderate loss of myelin and axons, but without reactive astrocytosis and no arterio- and arteriolosclerosis in the cerebral white matters.
MR images of the formalin-fixed brains (postmortem MR images) were obtained by using a 1.5T system. The fixed brains were positioned in a standard way in the head coil and axial and coronal fast spin-echo T2-weighted images (TR/TE, 3500/96; thickness/gap, 4/1) were obtained. Postmortem T2-weighted MR images showed deep cortical and subcortical laminar hyperintensities in the entire cerebral hemisphere (Fig 1G–I). Hyperintensities were also seen in the deep and subcortical white matters (Fig 1G–I). The laminar hyperintensities in the deep cortical layers and subcortical white matter on the postmortem coronal T2-weighted images showed laminar pallor of the deep layers of the cerebral cortices and the underlying U-fibers on histologic sections (Fig 1J, K). Histologic findings of the laminar pallor in the deep cortical layers revealed pseudolaminar spongy degeneration, pyknotic and shrunken neurons, and Alzheimer type II astrocytes associated with neutrophil rarefaction in the deep layers of the cerebral cortices (Fig 1L). Histologic findings of the laminar pallor of the underlying U-fibers showed loss of myelin and axons without reactive astrocytosis (Fig 1M, N). The hyperintensities in the deep and subcortical cerebral white matters on the postmortem T2-weighted images revealed histologically mild to moderate loss of myelin and axons without reactive astrocytosis (Fig 1O, P).
Case 2
The patient was a 58-year-old woman who received a blood transfusion during a caesarean section at 23 years of age. At age 52 years, her condition was diagnosed as liver cirrhosis. Four years later, she was admitted to the hospital because of mental confusion and a flapping tremor. Laboratory examinations revealed hyperammonemia (164 μg/dL). MR images showed hyperintensities in the bilateral globi pallidi on T1-weighted images and confluent hyperintensities in the deep and subcortical cerebral white matters on T2-weighted images, but no definite signal intensity changes in the cerebral cortices. Chronic hepatic encephalopathy was the diagnosis and the patient was treated with branched-chain amino acids and lactulose, and her symptoms soon subsided. Over the next 2 years, mental confusion occurred repeatedly and her condition gradually deteriorated. She had several general convulsions and died of hepatic coma. The total duration from the onset of the hepatic encephalopathy to her death was 2 years.
Autopsy revealed mixed macro- and micronodular cirrhosis (480 g) associated with hepatocellular carcinoma in her liver. The brain showed mild diffuse swelling and weighted 1220 g after fixation. Histologic examination showed numerous Alzheimer type II astrocytes in the cerebral cortices, putamen, caudate nucleus, globus pallidus, claustrum, thalamus, and cerebellar dentate nucleus, as well as in the substantia nigra. Pseudolaminar spongy degeneration was seen in the deep layers of the bilateral frontal cortices. There was mild to moderate loss of myelin and axons without arterio- and arteriolosclerosis, infiltration of inflammatory cells, and reactive astrocytosis in the cerebral white matters.
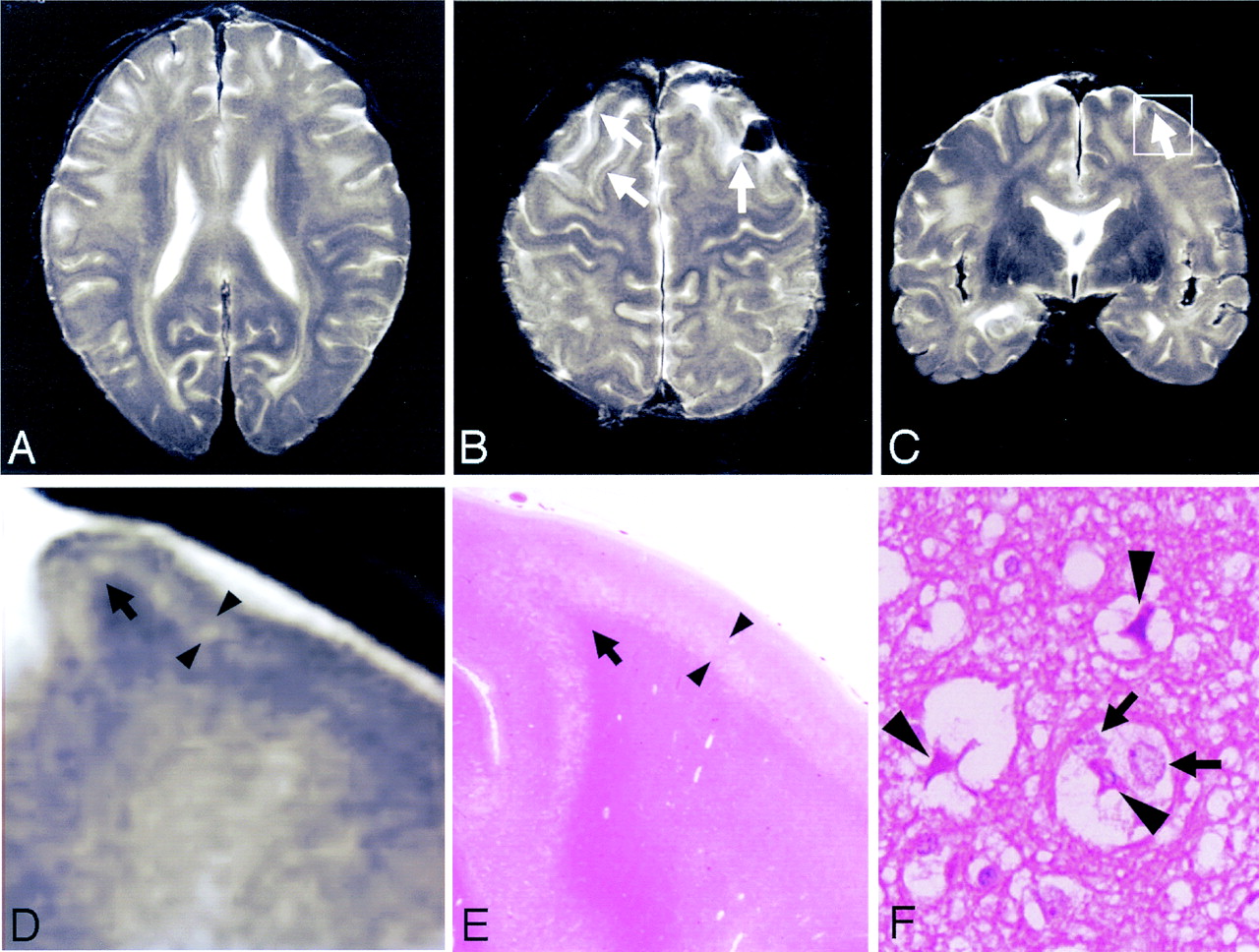
Postmortem T2-weighted MR images showed cortical laminar hyperintensities in the frontal lobes (Fig 2A–C). Hyperintensities were also seen in the deep and subcortical white matters but were more widespread in case one than in case two (Fig 2A–C). The laminar hyperintensities in the deep layers of the cerebral cortices on the postmortem coronal T2-weighted images showed laminar pallor of the deep layers of the cerebral cortices on histologic sections, whereas U-fibers were well preserved on both MR images and histologic sections (Fig 2D, E). Histologic findings of the laminar pallor in the deep cortical layers revealed pseudolaminar spongy degeneration, pyknotic and shrunken neurons, and Alzheimer type II astrocytes associated with neuropil rarefaction in the deep layers of the cerebral cortices (Fig 2F). The hyperintensities in the deep and subcortical cerebral white matters on the postmortem T2-weighted images revealed histologically mild to moderate loss of myelin and axons without reactive astrocytosis. The histologic features were of the same in nature in both cases but were more severe and widespread in case 1, in agreement with the postmortem MR images.

Case 2.
A–C, Postmortem axial (A and B) and coronal (C) T2-weighted MR images show cortical laminar hyperintensities in the frontal lobes (B and C, arrows). Hyperintensities are also seen in the deep and subcortical white matters.
D, Boxed area in panel C shows laminar hyperintensities in the deep layers of the cerebral cortex (arrowheads).
E, The hematoxylin and eosin-stained section corresponding to panel D shows laminar pallor of the deep layers of the cerebral cortex (arrowheads). U-fibers are well preserved in this case (D and E, arrows).
F, Histologic findings of the arrowhead area panel E shows spongy changes of the neuropil, pyknotic, and shrunken neurons (arrowheads) and Alzheimer type II astrocytes (arrows). (Hematoxylin and eosin ×100.)
Discussion
In the present cases, the antemortem T2-weighted images obtained 3 years before death in case 1 showed slight laminar hyperintensities in limited frontal and parietal cortices but were more extensive on the postmortem T2-weighted images. The laminar hyperintensities on the postmortem MR images histologically corresponded to pseudolaminar spongy degeneration associated with numerous Alzheimer type II astrocytes in the deep layers of the cerebral cortices in both cases and also corresponded to loss of myelin and axons in the underlying U-fibers in case 1. These histologic findings are characteristic of chronic hepatic encephalopathy (2). It is well known that similar cortical laminar T2 hyperintensities are also present in cases of hypoxic-ischemic brain damage (9, 10). In hypoxic-ischemic encephalopathy, however, they are frequently located in the boundary zones of the cerebral cortices, reflecting hemodynamic factors, whereas in chronic hepatic encephalopathy, they are most striking in the superior parietal and posterior frontal convexities (2). A few MR imaging studies have reported that the extent of cortical laminar T2 hyperintensities in cases of acute hepatic encephalopathy does not accord with the territories of arterial perfusion (7, 8). In our cases, the cortical laminar T2 hyperintensities were located partially in the bilateral frontal lobes in case 2 and entirely in the cerebral hemispheres in case 1. Thus, both the extent and histologic findings support the view that the cortical lesions were caused by chronic hepatic encephalopathy.
T2 hyperintensities in the cerebral white matters found in our cases, histologically showing mild to moderate loss of myelin and axons are not always found in chronic hepatic encephalopathy. Chronic hypoxic-ischemic lesions, such as those in the white matter of Binswanger disease, produce similar MR images. In our cases, however, there were neither arterio- and arteriolosclerosis nor reactive astrocytosis, which are always found in chronic hypoxic-ischemic lesions. There have been few MR imaging studies describing the occurrence of T2 hyperintensities in the cerebral white matters in patients with chronic hepatic encephalopathy (11). It has also been reported that T2 hyperintensities in the cerebral white matter found in 11 patients with liver cirrhosis normalized after successful liver transplantation, suggesting that they may reflect mild edema (12). Furthermore, it has been reported that typical brain metabolic changes in eight patients with liver cirrhosis, decreased mI/creatine (Cr) and Cho/Cr ratios and an elevated Glx/Cr ratio, normalized after liver transplantation on MR spectra (6). In our cases, the cerebral white matter lesions were more widespread in the later stage of the illness and in case 1 with a 19-year clinical course, and arterio- and arteriolosclerosis were not found. These findings suggest that the white matter lesions are also caused by chronic hepatic encephalopathy and may be associated with edematous changes.
Conclusion
Focal or extensive laminar T2 hyperintensities in patients with chronic hepatic encephalopathy reflect pseudolaminar spongy degeneration involving the deep layers of the cerebral cortices and occasionally involving the underlying U-fibers. T2 hyperintensities in the cerebral white matter reflect loss of myelin and axons, which may be due to longstanding edema caused by chronic hepatic encephalopathy.
Acknowledgments
We wish to thank to Drs. Hajime Miyata and Makoto Ostuka for their valuable discussion.
References
- Received April 3, 2004.
- Accepted after revision June 1, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Multimodality MR Imaging Findings of Low-Grade Brain Edema in Hepatic Encephalopathy
- Brain Magnetic Resonance Imaging Findings in Young Patients with Hepatosplenic Schistosomiasis Mansoni without Overt Symptoms
- Acute Hepatic Encephalopathy: Diffusion-Weighted and Fluid-Attenuated Inversion Recovery Findings, and Correlation with Plasma Ammonia Level and Clinical Outcome