
Abstract
SUMMARY: Patients with spinal muscular atrophy often have complete interlaminar osseous fusion, precluding lumbar puncture via the standard interlaminar approach. Recently, we have developed a new coaxial curved-needle variation of fluoroscopy-guided transforaminal lumbar puncture for intrathecal injections in this patient population. Between October 2017 and November 2018, fifty-nine consecutive transforaminal lumbar punctures using this technique were performed in 12 patients with spinal muscular atrophy for intrathecal nusinersen injection, with a 100% technical success rate and no C1–2 punctures required. One major complication occurred, consisting of a post–dural puncture headache, which required a therapeutic transforaminal epidural blood patch. Two minor complications occurred, both of which involved inadvertent puncture of a dorsal muscular arterial branch, without clinical sequelae. A fluoroscopy-guided curved-needle transforaminal approach is an effective technique for lumbar puncture in difficult cases, such as in this cohort of patients with spinal muscular atrophy and complete interlaminar osseous fusion undergoing intrathecal nusinersen injections.
ABBREVIATIONS:
- TFLP
- transforaminal lumbar puncture
- SMA
- spinal muscular atrophy
Recently, the US Food and Drug Administration approved nusinersen (Spinraza) as the first effective therapy for spinal muscular atrophy (SMA). The medication is administered intrathecally, with a standard treatment protocol that involves 3 loading doses separated by 2 weeks, a fourth injection at 1 month, and maintenance doses every 4 months.
Patients with SMA often have severe neuromuscular scoliosis with subsequent extensive posterior spinal fusion and, frequently, complete interlaminar osseous fusion, precluding lumbar puncture via the standard interlaminar approach.1 Fluoroscopically guided C1–2 puncture by a lateral approach is considered standard practice for intrathecal access when the posterior lumbar interlaminar approach is not possible. However, rare-but-serious risks are associated with this technique, including cervical cord puncture and vertebral artery injury.2,3
We have been performing fluoroscopy-guided transforaminal lumbar puncture (TFLP) at our institution since 2007 as an alternative to C1–2 puncture for lumbar punctures with difficult interlaminar access. The purpose of this study was to evaluate the effectiveness and safety of a novel coaxial curved-needle technique for fluoroscopy-guided TFLP in a cohort of patients with SMA and complete interlaminar osseous fusion undergoing lumbar puncture for intrathecal nusinersen injection.
Case Series
Case Selection.
Following local institutional review board approval and a waiver of informed consent, a retrospective review was performed of 59 consecutive fluoroscopy-guided TFLPs using a curved-needle technique for intrathecal nusinersen injection in 12 patients between October 2017 and November 2018. TFLPs performed for other indications or using a different technique were excluded.
Patients were identified as candidates for TFLP when there was a known history of posterior spinal fusion and evidence of interlaminar osseous fusion on available imaging, most commonly radiographs (62.5%, n = 7). Preprocedural planning CTs were performed in only 25% (n = 3) of patients, 2 of which were obtained before the study period, before development of our current technique when we previously used various straight-needle techniques. The other planning CT was obtained very early in the study period. Patients were evaluated for possible complications before discharge, at the subsequent procedural encounter, and during clinical follow-up.
Technical success, defined by a return of CSF and complete medication delivery, was evaluated. Immediate and delayed complications, fluoroscopy time, and radiation dose were also evaluated. Fluoroscopy time was recorded for all cases. Dose-area product and air kerma were recorded for 12 procedures, which we began prospectively recording late in the study period and could not be retrospectively recovered for earlier procedures. Effective dose was calculated using a conversion coefficient of 0.21 mSv (Gy × cm2)−1 and the formula: Effective Dose = Dose Conversion Coefficient × Dose-Area Product.4 A Student t test was used to compare mean fluoroscopy times between the first 30 TFLPs and the final 29 TFLPs to assess a learning curve effect. Complications were classified as major or minor according to Society of Interventional Radiology clinical practice guidelines.5
RESULTS
The 12 patients ranged from 11 to 37 years of age (mean, 21.5 years) with 62.5% (n = 7) females. All patients had spinal fusion extending from the upper thoracic spine to the sacrum. Fifty-nine TFLPs were performed (mean, 4.9 per patient; range, 3–6) with a 100% technical success rate. The mean fluoroscopy time was 3.8 minutes (range 0.2–15.8 minutes), and the mean fluoroscopy time was shorter for the final 29 TFLPs compared with the first 30 TFLPs (2.7 minutes versus 4.8 minutes, P < .01). The mean air kerma was 63.1 mGy (range, 20.8–154 mGy; n = 12), and the mean effective dose was 1.07 mSv (range, 0.29–2.7 mSv; n = 12). Right-sided neural foramina were used for access more commonly, L3–4 was the level most often used, and procedures were typically performed with the patient under general anesthesia, as determined by the anesthesiologist (Table 1). One major complication occurred, consisting of a post–dural puncture headache, which required inpatient hospital admission and a therapeutic transforaminal epidural blood patch. Two minor complications occurred, both of which involved inadvertent puncture of a dorsal muscular arterial branch during placement of the introducer needle. In both cases, positioning of the needle was assessed by contrast injection, which showed the intra-arterial tip position and no visible flow into the spinal canal. The needles were repositioned, the procedures were completed, and the patients were observed for an additional 6 hours without sequelae.
Procedural details
DISCUSSION
Technique
Equipment and Patient Positioning.
All TFLPs were performed using biplane fluoroscopy (Axiom Artis dBA; Siemens, Erlangen, Germany). Patient positioning was determined on the basis of lumbar curvature, taking into account the unilateral dorsal presentation of 1 neural foramen in cases of rotatory scoliosis. A right-transforaminal approach was preferred due to our standard practice of placing patients in the left-lateral decubitus position for lumbar punctures. If patient anatomy required a left-transforaminal approach (left neural foramen oriented more dorsally due to rotatory scoliosis), the patient was positioned semiprone (left side down) with the head turned to the right. In this position, a posterior oblique approach to the left neural foramen was essentially parallel to the fluoroscopy table. Procedures were performed with the patients under either general or local anesthesia according to patient and anesthesiologist preference. Conscious sedation administered by an RN was not used due to concerns for respiratory compromise in this patient population.
Procedural Technique
A coaxial technique with an inner curved needle was previously described for access to the L5–S1 disk for diskography,6 and we used a similar technique for access to the target neural foramen using a Pakter Curved Needle Set (Fig 1; Cook Medical, Bloomington, Indiana). For aiming of the introducer needle, the B-plane fluoroscopy arm (fluoroscopy plane parallel to the floor) was initially positioned in a posteroloateral oblique projection along the long axis of the pedicle inferior to the target neural foramen (approximately 15°–20° lateral from posteroanterior) (Fig 2A). For depth control, the A-plane fluoroscopy arm (fluoroscopy plane perpendicular to the floor) was positioned in a standard lateral projection, with attention paid to precise superimposition of the bilateral neural foramina at the target level (Fig 2C).
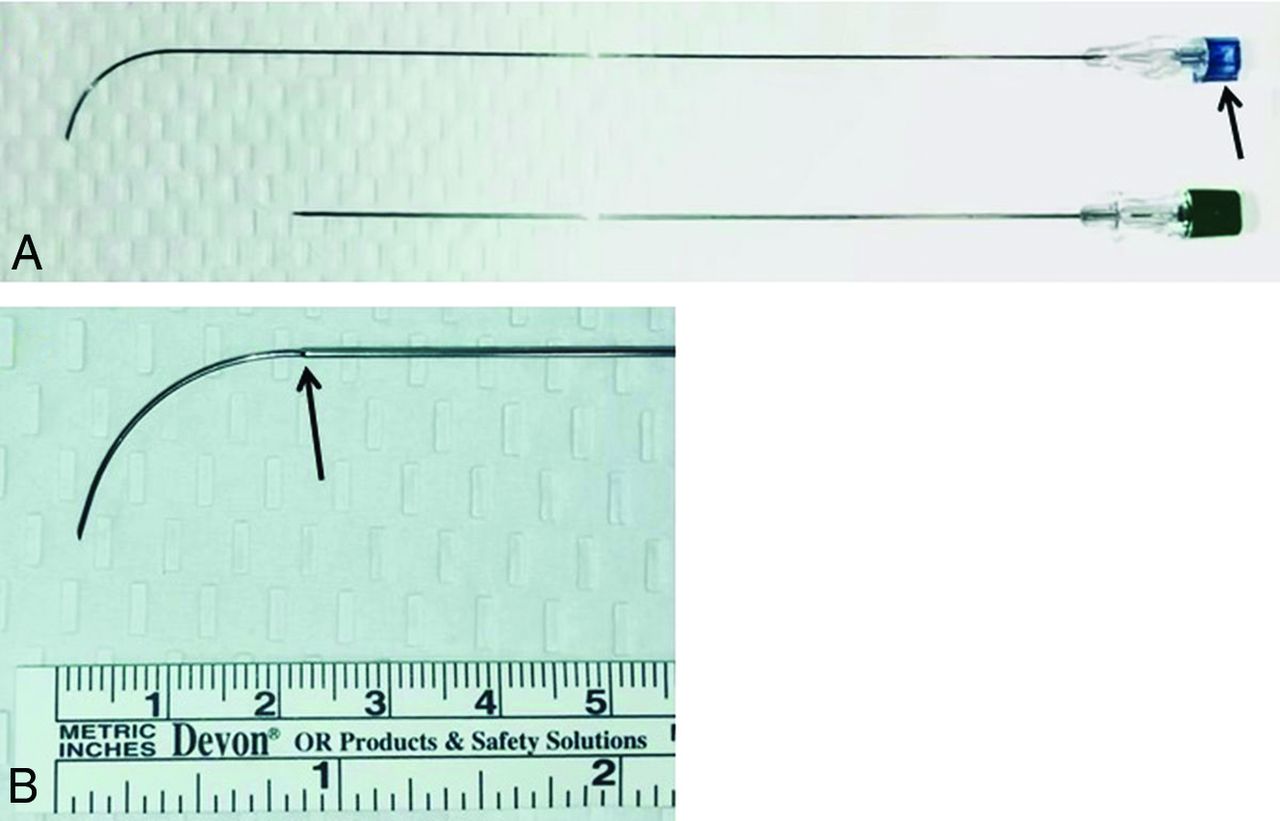
The Pakter Curved Needle Set. A, Unmagnified view of the outer 15-cm 21-ga introducer needle (bottom) and inner 20-cm 25-ga curved needle (top). The notch on the inner needle indicates the direction that the needle will curve as it exits the introducer needle (arrow). B, Magnified view of the curved inner needle exiting the introducer needle (arrow indicates introducer needle tip).

Spot radiographs demonstrating steps in TFLP using the curved Pakter needle. A, posterolateral oblique view along the long axis of the pedicle. A ring forceps indicates the skin entry site at the level of the disk (asterisks), just lateral to the pedicles (hashtags). B and C, posterolateral oblique and lateral views show the correct position of the outer guiding needle terminating just lateral to the posterior margin of the target neural foramen and projecting over the lateral disk margin on the posterolateral oblique view (arrow). D and E, posteroanterior and lateral views show the correct position of the outer needle (dashed arrow) and the inner curved needle (solid arrow), having passed through the target neural foramen and terminating within the thecal sac at L3–4.
Using the posterolateral oblique view, we marked the skin overlying the target site at the lateral aspect of the disk corresponding to the target neural foramen (Fig 2A). Next, the introducer needle was advanced with biplane fluoroscopic control from the skin-entry site toward the target site at the lateral disk margin (Fig 2B) until the needle tip depth reached the posterior margin of the target neural foramen on the lateral projection (Fig 2C). This was the final position of the introducer needle.
For medial aiming and depth control of the coaxial 25-ga curved needle, the B-plane fluoroscopic arm was adjusted from posterolateral oblique to true posteroanterior; the A-plane remained in the lateral projection. The coaxial 25-ga curved Pakter needle was then directed medially and passed through the introducer needle until both were tip-to-tip. Under live biplane fluoroscopic control, the curved needle was then advanced through the inferior neural foramen to the midline, puncturing the thecal sac (Figs 2D, -E); the puncture was confirmed by return of CSF. Five milliliters of CSF was removed, and 12 mg of nusinersen in 5- mL total volume was delivered intrathecally during 1–3 minutes.
Safety
The only noteworthy complication encountered (1.6%) was a post–dural puncture headache requiring a therapeutic transforaminal epidural blood patch. This is similar to the reported rate of blood patch both in this patient population7 and in a patient population8 without SMA via the standard interlaminar approach. Two minor complications (3.2%) also occurred, consisting of puncture of a dorsal branch of the lumbar artery during placement of the outer 21-ga needle. Branches of the lumbar artery are typically located superiorly within the neural foramen,9,10 but in both of our cases of arterial puncture, the needle tip was at the level of the mid-posterior foramen on the lateral view and approximately 1 cm lateral to the pedicle on the posteroanterior view (Fig 3). Although neither patient experienced an adverse event related to arterial puncture, serious hemorrhagic complications have been reported due to injury of the lumbar artery and its branches during percutaneous image-guided spine procedures, including vertebral body biopsy,11 vertebroplasty,12 and kyphoplasty13 and during transforaminal percutaneous endoscopic lumbar diskectomy.10,14

Lateral fluoroscopic images during TFLP. A, Final position of the introducer needle (arrow). Blood return was noted at the needle hub after removal of the stylet. B, Injection of a small volume of iodinated contrast medium demonstrates opacification of a dorsal branch of the lumbar artery (solid arrows) and contrast collecting within the soft tissues (dashed arrow).
Given the potential for serious hemorrhagic complications, puncture of branches of the lumbar artery should clearly be avoided, and we now target the inferior neural foramen to avoid the dorsal branch. Although this complication has not been previously described related to TFLP, it should be kept in mind by all who perform TFLPs. Our technique differs from typical straight-needle techniques in that the stylet of the outer needle is removed when the needle tip is extraforaminal. Other straight-needle techniques likely involve removal of the stylet only when the needle tip is intrathecal; therefore, injury of an extraforaminal artery could go undetected. No patient in our cohort experienced persistent radicular symptoms.
The transforaminal approach has been used for epidural injections for decades, with increased use of this technique in recent years. More recently, the transforaminal approach has been described for intrathecal access, most commonly for administration of nusinersen.15⇓⇓-18 Weaver et al18 used conebeam CT with fluoroscopic guidance overlay to perform TFLPs via a short, linear posterolateral approach in a similar patient population. In their description of their institutional protocol for intrathecal nusinersen administration in patients with SMA, Mousa et al16 also used a straight-needle TFLP technique when an interlaminar approach was deemed infeasible. In both of these studies, preprocedural lumbar spine CT was performed in all patients who had spinal hardware and osseous fusion, to assess possible interlaminar access and to determine a suitable target neural foramen if an interlaminar access was not possible. With a straight-needle transforaminal technique, cervical puncture may still be required in a small percentage of patients when retroperitoneal structures are in the expected path of the needle. With the curved-needle technique described here, retroperitoneal structures are widely avoided (Fig 4); therefore, preprocedural CT is not performed, and no cervical puncture has been necessary.

Axial CT obtained in the same patient depicted in Figure 2 near the time of procedure but for an unrelated indication annotated to depict approximate trajectory and ending points of the outer guiding needle and curved inner needle using curved needle technique. Dotted line indicates guiding needle trajectory. Circle indicates guiding needle termination. Solid line indicates curved needle trajectory. Square indicates curved needle termination. Dashed arrows indicate hypothetical right and left straight needle trajectories at this level in this patient. Insert: corresponding AP scout image dashed line indicates plane of imaging.
Table 2 summarizes available publications using TFLP, which have provided radiation dose information in comparison with the current study. A conversion factor of 0.018 mSv/mGy × cm was used to calculate the effective dose for studies using CT guidance.15,17⇓⇓⇓-21 Radiation doses in the current study are similar to the lowest doses in published literature for TFLP. However, the total radiation dose in the current study is likely lower because we do not perform a planning CT, whereas most other authors either explicitly stated that planning CTs were performed18 or described planning CT being used in some cases while not explicitly stating whether this was routine practice.15,17,21 The effective dose of a diagnostic lumbar spine CT is approximately 13 mSv.22 The mean effective dose for the 3 planning CTs in the present study was 12.5 mSv.
Comparison of radiation doses associated with TFLP in the present literature
The multiplicity of recent publications and techniques indicates the ongoing challenges with intrathecal access in this patient population. The fluoroscopy-guided curve-needle transforaminal technique described here provides an attractive alternative for access. Potential benefits include the absence of a need for a surgical procedure, absence of the need for a planning CT, a low procedural radiation dose, a high technical success rate, and a low complication rate. In addition, the needle trajectory with the curved-needle technique widely avoids retroperitoneal organs, which may not always be the case with straight-needle TFLP techniques. While we use biplane fluoroscopy, this technique can be performed on single-plane equipment with minimal modification by alternating the image intensifier between the projections. Finally, with the fluoroscopic landmarks described, even very difficult spines can be accessed by a variety of radiologists; for example, 8 radiology residents and 4 neuroradiology fellows successfully performed this technique in the reported cohort, providing evidence of its simplicity and reproducibility.
This case series has several limitations. The sample size is small and, therefore, is underpowered to detect rare complications. The sample size is even smaller when considering the number of cases in which the effective dose could be calculated. Furthermore, the cases in which the effective dose could be calculated were late in the study period, and earlier cases during the development of the technique may have had higher effective doses, particularly given the longer fluoroscopy times early in the study period. Although no patient experienced persistent radicular symptoms, occasionally patients did experience radicular symptoms during passage of the needle through the neural foramen. However, because this immediately resolved in all cases on removal of the needle, it was not always documented in the procedural notes; therefore, the true incidence is not known. The potential for unrecognized motor deficits related to nerve root injury does exist in this population due to baseline deficits related to SMA.
CONCLUSIONS
A fluoroscopy-guided curved-needle transforaminal approach is an effective technique for lumbar puncture in difficult cases, such as in this cohort of patients with spinal muscular atrophy with complete interlaminar osseous fusion undergoing intrathecal nusinersen injections. Our results suggest that this technique is safe, but the small sample size indicates that further evaluation is warranted. Additionally, the radiation dose to the patient may be decreased compared with previously described techniques, particularly if a preprocedural planning CT is avoided.
Footnotes
Disclosures: Brian C. Cristiano—UNRELATED: Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: sponsored travel to educational meetings unrelated to the present study; Penumbra and Stryker neuroendovascular courses. Daniel R. Hoss—UNRELATED: Payment for Lectures Including Service on Speakers Bureaus: Biogen, Comments: I have served as a consultant for Biogen, the maker of nusinersen, regarding intrathecal access in complex spines. I have also served as a speaker for Biogen regarding various aspects of nusinersen use in patients with spinal muscular atrophy; Payment for Development of Educational Presentations: Biogen, Comments: I developed an educational presentation for the Biogen staff regarding nusinersen administration in patients with spinal muscular atrophy with complex spines.
Paper previously presented at: Annual Meeting of the American Society of Spine Radiology, February 20–24, 2019; Miami, Florida. Our initial experience regarding transforaminal lumbar puncture using a different technique was presented at: Annual Meeting of the American Roentgen Ray Society, April 13–18, 2008; Washington, DC.
References
- Received July 29, 2019.
- Accepted after revision October 21, 2019.
- © 2020 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}