
Abstract
BACKGROUND AND PURPOSE: A persistent foramen tympanicum, or foramen of Huschke, is an anatomic variation of the tympanic portion of the temporal bone due to a defect in normal ossification in the first 5 years of life. The foramen is located at the anteroinferior aspect of the external auditory canal (EAC), posteromedial to the temporomandibular joint (TMJ). We sought to define its prevalence, location, and size on high-resolution spiral CT (HRCT).
METHODS: We prospectively examined 102 consecutive HRCT studies of the temporal bone (204 ears). HRCT was performed by using 120 kV, 400 mAs, an ultra–high-resolution filter, 0.6-mm section thickness, 0.3-mm section increment, 728 × 728 matrix, and 160-mm field of view. We noted the size and location of the foramen tympanicum relative to the tympanic membrane and calculated its prevalence. Patients with focally decreased tympanic bone thickness of <1 mm at the anteroinferior EAC (between the 3- and 6-o’clock positions) were considered separately.
RESULTS: We found a foramen tympanicum was found in six (4.6%) of 130 ears. Mean axial diameter was 4.2 mm, and mean sagittal diameter was 3.6 mm. Focally reduced bone thickness in the same location was found in 45 (35%) ears, with a female preponderance (P = .003).
CONCLUSION: HRCT is sensitive for detection of the foramen tympanicum because of its thin sections, high spatial resolution, and multiplanar capabilities. Awareness of this anatomic entity may be useful in evaluating patients with transient otorrhea in whom no otologic cause (e.g., ear infection, TMJ disease) is identified.
The foramen tympanicum, also known as the foramen of Huschke, is an anatomic variation in the tympanic portion of the temporal (tympanic) bone. When present, it is located at the anteroinferior aspect of the external auditory canal (EAC), posteromedial to the temporomandibular joint (TMJ) (1, 2) (Fig 1). Focal reduction of tympanic bone thickness may also be observed in the same location (3) (Fig 2).

HRCT sections of the temporal bone through the inferior portion of the EAC. Images show the anteroinferior location of the foramen tympanicum, posterior to the TMJ (arrowhead).
A, Axial.
B, Sagittal.

Axial HRCT sections of the temporal bone in two patients through the same level at the inferior portion of the EAC.
A, Normal tympanic bone.
B, Focal anteroinferior reduction in tympanic bone thickness 2 mm lateral to the tympanic membrane (arrowhead).
A foramen tympanicum may predispose individuals to TMJ pathology (4), or it may be associated with salivary discharge into the EAC during mastication (5, 6). During TMJ arthroscopy, inadvertent passage of the arthroscope into the EAC and resultant otologic complications has also been reported (7, 8). Persistence of the foramen tympanicum may also predispose the person to the spread of infection or tumor from the EAC to the infratemporal fossa, and vice versa (1, 6, 9). The purpose of this study is to define the prevalence, precise location, and size of the foramen tympanicum by using high-resolution spiral CT (HRCT).
Methodsm
We prospectively evaluated 102 consecutive HRCT studies of the temporal bone (204 ears). Each study (MX 8000 quad; Philips Medical Systems, Eindhoven, the Netherlands) was performed by using the following parameters: 120 kV, 400 mAs, ultra–high-resolution filter, 0.6-mm section thickness, 0.3-mm section increment, 728 × 728 matrix, and 160-mm field of view. Therefore, the in-plane resolution was equivalent to 0.21 mm. We considered the bony foramen was present when its dimension was greater than twice the pixel size (0.42 mm). Axial and multiplanar reformatted images in sagittal and coronal planes were studied. Axial images were acquired in the orbitomeatal plane.
Patients with a history of ear surgery or temporal bone trauma or fracture and those younger than 5 years were excluded. We also excluded technically suboptimal HRCT scans. A senior neuroradiologist (K.M.-D.) and one in training radiologist (A.L.) independently analyzed the HRCT studies. We considered only anteroinferior bony dehiscences because they corresponded to the anatomic site of the foramen tympanicum where the developmental ossification prominences fuse (e.g., between the 3- and 6-o’clock positions). We identified the foramina on axial images and confirmed their existence on coronal and sagittal reformatted images. For every patient, we noted the presence of a foramen, its size, and its location in relation to the tympanic membrane. We measured the size of the foramen in the axial plane, as well as on the reconstructed coronal and sagittal planes. We measured its distance to the anterior insertion of the tympanic membrane to determine its precise location.
We calculated the prevalence of the persistent foramen tympanicum. Patients in whom the tympanic bone was less than 1 mm thick were considered separately. An additional open-mouth HRCT of the temporal bone was performed in one patient in whom a foramen tympanicum was detected. This was done to demonstrate dynamic soft-tissue herniation through the foramen that might explain the patient’s TMJ pain. We informed the patient of the clinical relevance and prospective nature of our study.
Results
Thirty-seven of the 102 HRCT studies were excluded from further evaluation: 31 because of previous temporal bone surgery, five because of previous temporal-bone trauma, and one because the scans were technically suboptimal. Studies in the remaining 65 patients (130 temporal bones) formed the basis of our investigation. The patients included were 32 male patients (mean age, 42 years; range, 11–73) and 33 female patients (mean 49 years; range, 7–92 years) with an overall mean age of 45 years (range, 7–92 years). Indications for HRCT were hearing loss (36 patients), chronic otitis (17 patients), infections (four patients), tumors (five patients), and miscellaneous (three patients).
We identified six (4.6%) of 130 ears with a persistent foramen tympanicum. This was found in four (6%; three female, one male) of 65 patients (1 mol/L) and was unilateral in two patients (two female; 0 mol/L) and bilateral in two (one female, one male; 1 mol/L). The shape of the foramina was considered oval because their dimensions in two planes were slightly different. Their mean size was 4.2 mm in the axial plane (range, 2.8–4.8 mm) and 3.6 mm in the sagittal plane (range, 2.2–5.3 mm). The tympanic membrane was always identified on these images, near the persistent tympanic foramen with a mean distance of 1.0 mm (range, 0–2.2 mm). One tympanic foramen was continuous with the tympanic sulcus.
HRCT scans in the one patient with a persistent foramen tympanicum who underwent the additional study showed was no herniation of soft tissue through the foramen.
Forty-five (35%) of 130 tympanic bones had decreased thickness (<1.0 mm) at the anteroinferior portion. The 45 affected tympanic bones were found in 27 (42%) of our 65 patients. Eighteen patients (28%; 12 female, six male) of the 65 had bilateral involvement (6 mol/L), whereas nine (14%; four female, five male) had unilateral involvement (5 mol/L).
Discussion
We previously observed two patients with pathologies related to a persistent foramen tympanicum who provided the impetus for our present investigation. The first was a 52-year-old woman who complained of clear discharge from her left EAC. Symptoms occurred only when she was eating; this suggested a salivary fistula. She had no history of trauma or tympanic bone surgery. High-resolution CT sialography of the left parotid gland was performed after catheterization of Stenson duct and the injection of 2 mL of iodinated contrast agent. HRCT scans of the temporal bone were obatined and reviewed in both bone and soft tissue windows. Submucosal and nodular enhancement in a large osseous defect of the tympanic bone was observed, suggesting ectopic salivary gland tissue (Fig 3). However, we detected no extravasation of contrast agent into the EAC during HRCT sialography. An open-mouth HRCT scan showed no change in the soft tissue swelling. The patient underwent successful surgical closure of the fistula.

Axial HRCT sialograms (soft tissue window) of the left parotid gland through the inferior portion of the EAC show (arrow) submucosal nodular enhancement in the foramen tympanicum, suggesting ectopic salivary-gland tissue.
The second patient was a 90-year-old woman who presented with right external otitis. She complained of a long history of chronic TMJ pain. Clinical examination revealed dome-shaped swelling on the right anteroinferior EAC wall. HRCT of the temporal bone demonstrated an anterior bony dehiscence of the right EAC, a soft-tissue mass extending from the TMJ into the EAC, and air pockets in the TMJ region (Fig 4A). Open-mouth HRCT showed anterior retraction of the mass into the TMJ region (Fig 4B). T1-weighted MR images (TE/TR, 500/15) obtained with and without gadolinium enhancement showed an enhancing, periarticular soft-tissue mass herniating through a foramen tympanicum into the EAC (Fig 4C). No treatment was performed because of the patient’s age.

Axial HRCT sections (bone window) of the temporal bone through the inferior portion of the EAC.
A, Closed-mouth view shows herniation of soft tissue herniation into the EAC 2 mm lateral to the tympanic membrane (arrowhead).
B, Open-mouth view show subcutaneous air pockets spreading along the TMJ (arrow). Slight retraction of the soft tissue material is noted when the mouth is open.
C, Contrast-enhanced T1-weighted MR image (TE/TR, 500 /15) through the inferior portion of the EAC shows enhancement of the herniating soft tissue (arrowhead).
The tympanic bone, which contributes to formation of the EAC and tympanic cavity, develops from a membranous ossification process (10, 11). Development of the tympanic bone explains the difference in orientation between infants and adults. The tympanic membrane is formed in utero by the connection of the first entoblastic and epiblastic pouches. At 9 weeks’ gestational age, four ossification centers develop around the tympanic membrane, fusing to form a U-shaped bone (7). This bone fuses with the squamous portion of the temporal bone during the 35th week of gestational age. Therefore, at birth, the entire tympanic bone is incompletely developed and forms a U shape. Two prominences, one anterior and one posterior to the U-shaped bone, arise and grow toward each other. These two points of ossification fuse at the age of 1 year, the first step of EAC development. The foramen tympanicum persists medial to the point of fusion. In most children, the foramen tympanicum gradually becomes smaller and completely closes before the age of 5 years, but it occasionally persists (1, 10) (Fig 5). Therefore, tympanic bone dehiscence present at the precise point of fusion of the two prominences should be considered an anatomic variant only after the age of 5 years (12).
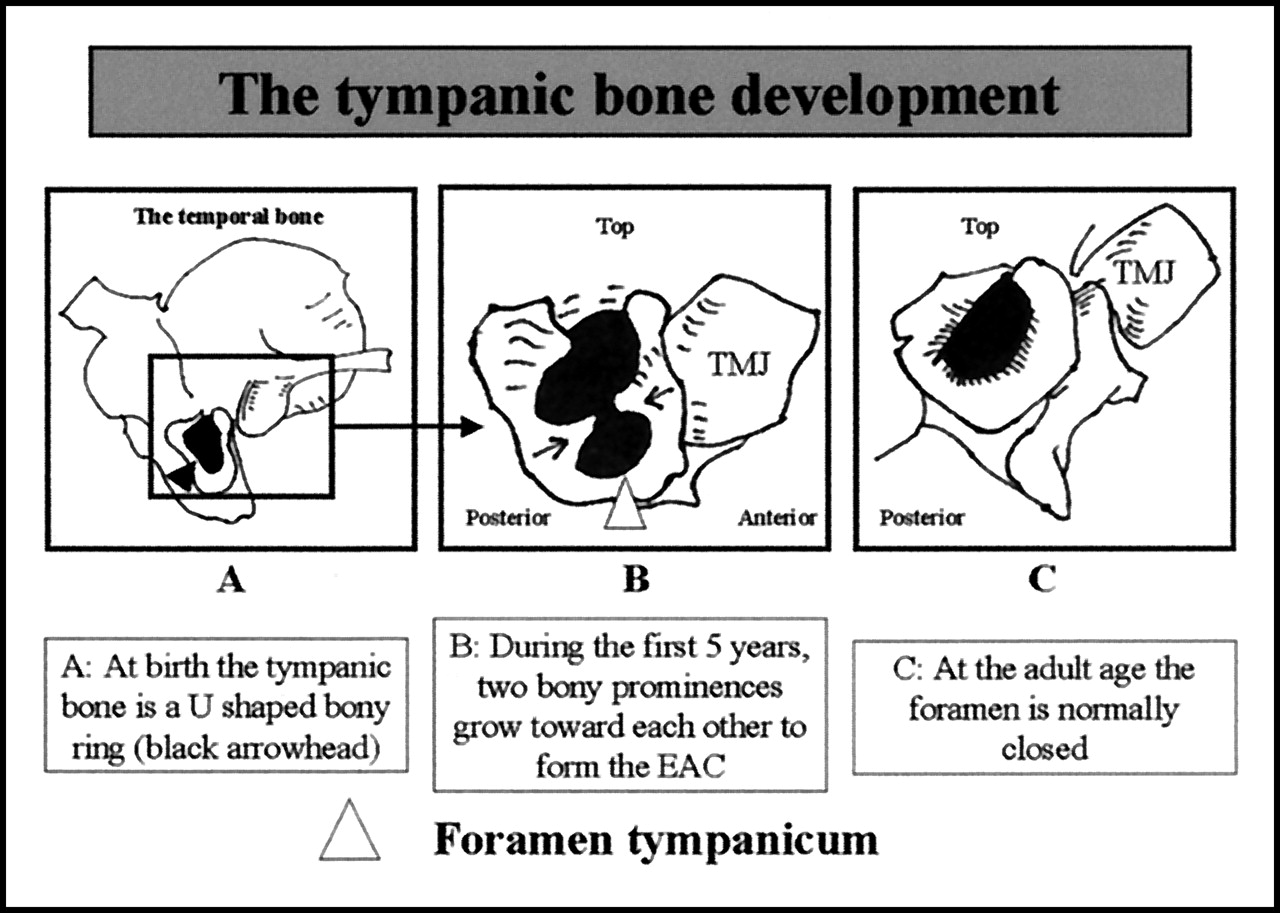
Schema illustrates normal postnatal development of the tympanic bone (used with permission from Anson BJ, Donaldson JA. Surgical Anatomy of the Temporal Bone. 3rd ed. Philadelphia: W. B. Saunders; 1981:122).
Many factors influence the ossification process of the tympanic bone after birth. Mechanical environment of the mandible against the tympanic bone is one factor to consider. The maxillofacial and tympanic bones grow after birth, primarily in response to pressure created by the actions of mastication, deglutition, and respiration (12, 13). Therefore, we can hypothesize that the tympanic foramen is an osseous developmental defect. The influence of the pressures sustained by the tympanic bone on the development of the TMJ is probably great. We also hypothesized that dehiscence of the tympanic bone is linked to abnormal development of the first branchial arch. However, anomalies of the first branchial arch end at the inferior part of the EAC at a different place of a persistent foramen tympanicum (14). Furthermore, the tympanic ring could have a role in ossification of the tympanic bone, as congenital cholesteatoma has been linked to abnormal development of the tympanic ring, which cannot stop the migration of the EAC ectodermal tissue into the middle ear (15). Therefore, an anomaly of the tympanic ring during embryogenesis could lead to an abnormal ossification of the tympanic bone and to a persistent foramen tympanicum. We also suggest that persistence of the foramen tympanicum may be linked to genetic factors promoting a focal anomaly of ossification (13).
The foramen tympanicum is a variant of ossification that transmits no neural or vascular structures. It is an osseous defect closed by a membranous structure. The term foramen is defined by a structure traversing it (16). Therefore, the foramen tympanicum is not a true foramen; is may be more appropriately termed a bony or osseous defect or dehiscence.
Wang et al (1) found a rate of persistent foramen tympanicum of 7.2% in an osteologic study (377 skulls), with some differences between the populations studied: rates were 6.7% in the skulls from China and 9.1% in skulls from Toronto (1). However, this study may have had a high rate of false-positives because of the manipulation of fragile bones. The investigators found that the foramen is very near the tympanic membrane, in agreement with our findings, and they also reported the same mean dimension of 3 mm (range, 1–6 mm).
To our knowledge, the sex distribution of the foramen tympanicum has not been studied. Among our four patients with a foramen tympanicum, three were female, but this sample was not a large enough for us to suggest a female preponderance for the foramen tympanicum. However, most patients with foramen tympanicum reported in the literature were female (Table). We also observed a female preponderance among our patients with focal reduction of tympanic-bone thickness (P = .003). Therefore, the female distribution of abnormal ossification might have been due to differences in growth and development of the mandible between male and female individuals.
Foramen tympanicum reported in the literature
Pathology associated with a foramen tympanicum is occasionally reported (Table). A foramen tympanicum may permit spontaneous herniation of soft tissue from the TMJ into the EAC, which can cause TMJ pain and dysfunction (2, 3, 17–19). These herniations are characteristic and fairly easy to identify because they usually retract out of the EAC with anterior translation of the TMJ that occurs during opening of the mouth (3, 4, 17–19). Therefore, soft-tissue protrusion into the EAC is usually visible only when the patient’s mouth is closed, and it may completely disappear when the mouth is opened. The origin of this herniation is unclear (3, 4, 19), but it has been reported as a complication of external otitis (9) and TMJ arthritis (17). Herniation of the posterior and deep insertions of the TMJ meniscus through the foramen tympanicum into the EAC has also been reported (18).
A foramen tympanicum may also facilitate ear injury during TMJ arthroscopy performed with an endoscope of less than 3 mm in diameter, which may penetrate into the EAC by traversing the persistent foramen (7, 8). Reported otologic complications are tympanic membrane rupture, dislocation of the incus, injury to the tympanic segment of the facial nerve, labyrinthine disruption, and ear infection (7). Other associated pathologies are related to otorrhea without any evident otologic causes. Both salivary-gland fistulas (4, 17) and synovial TMJ fistulas are reported (20). However, biochemical analysis of EAC discharges is often difficult because of small samples. Otorrhea usually begins with TMJ movement during mastication and is not specific to either salivary or TMJ fistulas, as mastication causes salivary gland secretions and TMJ movements facilitate synovial discharge into the EAC. The parotid gland can extend to the glenoid fossa behind the TMJ and lie near the osseous portion of the EAC (5). CT sialography of the parotid gland can lend credence to the hypothesis of a salivary fistula by demonstrating submucosal nodular enhancement in the foramen tympanicum, which may correspond to salivary gland tissue. However, extravasation of contrast agent into the EAC has not been observed during parotid CT sialography (20). The reported fistula connecting the EAC and the TMJ was not histologically confirmed (20). Similarly, infectious complications of the TMJ associated with synovial fistulas have not been reported. Last, the foramen tympanicum is a zone of reduced mechanical resistance that may predispose the person to infectious or tumoral spread from the EAC into the infratemporal fossa, and vice versa (1, 6, 9).
Focal reduction of tympanic bone thickness at the same location as a foramen tympanicum may weaken the tympanic bone, and patients may present with some of the same complications as those associated with a foramen tympanicum (7). In addition, persistence of the foramen tympanicum creates an anatomic communication between the EAC and the infratemporal fossa, similar to other known anatomic communications (17). Post-traumatic or postsurgical defects are usually not located in the same location. The anterior cartilaginous wall of the EAC contains small defects filled with connective tissue called Santorini fissures (17). The EAC nerve, a branch of the auriculotemporal nerve, may also create a communication between the EAC and the infratemporal fossa via a small millimetric canal located at the anteroinferior part of the tympanic bone.
Conclusion
The foramen tympanicum is well-demonstrated on HRCT and not uncommon, occurring in 4.5% of the ears in our cohort. This osseous defect may be due to abnormal mechanical forces during postnatal facial development and/or ossification abnormalities due to genetic factors. Variations in the tympanic bone may be associated with certain pathologic conditions and should be systematically excluded on all HRCT examinations regardless of the patients’ clinical symptoms. Because no neurovascular structures traverse the foramen tympanicum, it is not a true foramen, but rather, a defect of tympanic bone ossification. Therefore, according to modern concepts of anatomy, the foramen tympanicum, or the foramen of Huschke, seems to be a misnomer and should be called tympanic bone dehiscence.
Acknowledgments
We thank Thor Bessier, Stanford University, and Dupuch Sonia, Philips, San Jose, CA, for their help and suggestions on this article. We also thank the Dr Chng Soke Miang for her help.
Footnotes
Presented at the 42nd Annual Meeting of the American Society of Neuroradiology, Seattle, WA, June 5–11, 2004.
References
- Received May 25, 2004.
- Accepted after revision December 11, 2004.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}