
Abstract
BACKGROUND AND PURPOSE: In the early 1980s, diagnosing periventricular leukomalacia (PVL) in neonates by using cranial sonography was possible for the first time. Our purpose was to investigate the possibility of diagnosing PVL in the acute stage by using MR imaging. We evaluated early MR features of hypoxic-ischemic brain injury in neonates with periventricular densities (flares) on cranial sonograms to determine the added value of MR imaging over sonography alone for early diagnosis of brain damage.
METHODS: In a prospective study, infants who showed flares and/or cysts on sonograms underwent MR imaging during the (sub)acute stage.
RESULTS: Fifty infants were classified according to the highest sonographic grade up to the day of MR imaging: 23 infants had sonographic grade 1 (flares < 1 week), 15 had sonographic grade 2 (flares ≥ 1 week), four had sonographic grade 3 (small localized cysts), and eight had sonographic grade 4 (extensive periventricular cysts); none had sonographic grade 5 (multicystic leukomalacia) on the day of MR imaging. Overall, the additional information provided by MR imaging (over sonography alone) consisted of the depiction of hemorrhagic lesions in 64% of the infants. Extent and severity of the hemorrhages varied from isolated punctate lesions to extensive hemorrhages throughout the white matter; the latter were followed by cystic degeneration at autopsy in two infants. In nine of the 12 infants with cystic PVL, MR images showed more numerous or more extensive cysts. In addition, in two infants, MR images showed cysts not present on sonograms. In 32% of the infants, MR imaging provided no additional information; in these children, all but one had flares on sonograms whereas MR images showed no abnormalities or a zone of mild periventricular signal change.
CONCLUSION: MR imaging can depict the precise site and extent of hypoxic-ischemic brain injury at an earlier stage and allows a wider differentiation of lesions as compared with sonography alone. Hemorrhagic PVL is considered to be rare, but was present in 64% of our study population.
In the early 1980s, Hill et al (1) showed for the first time the possibility of diagnosing periventricular leukomalacia (PVL) in the neonatal period by using cranial sonography. Since that time, more information has become available about the sequence of events as they appear on sonograms. In the acute phase, an increased echogenicity of the periventricular white matter can be noted, appearing within 24 to 48 hours after a hypoxic-ischemic incident. The affected periventricular white matter is usually as bright as or brighter than the choroid plexus, in contrast to a normal periventricular halo, which is less bright than the choroid plexus. Two to 4 weeks later, cysts can appear in the hyperechogenic areas. Finally, the cysts resolve, with development of ventricular enlargement. The spectrum of leukomalacia diagnosed with sonography was described by De Vries et al (2). However convenient in use, sonography also has its limitations. It has been documented that sonography depicts between 28% and 80% of histologically evident PVL (3–5). One of the problems is the difficulty in differentiating between a normal periventricular halo and prolonged flares (so-called PVL grade 1). Furthermore, it may be difficult to assess the severity of echogenicity. Several investigators have pointed to the intra- and interobserver disagreement, which has been substantial in some studies (6, 7).
MR imaging has been applied widely to evaluate late sequelae of neonatal hypoxic-ischemic brain injury. Well-known injury patterns are basal ganglia necrosis, multicystic encephalopathy, central corticosubcortical damage, and, the most common type, PVL (8–13). Late MR findings of PVL are white matter loss, ventricular dilatation, and abnormally increased signal in the periventricular region on T2-weighted images (9). During the last few years, the usefulness of MR imaging in the early stages of hypoxic-ischemic brain injury has been demonstrated (11, 12, 14–26). Only a few studies have compared neonatal MR imaging with sonography (27–32) or neonatal MR imaging with autopsy findings (33).
The aim of the present study was to delineate early MR features of hypoxic-ischemic brain injury in neonates with periventricular densities on sonograms and to determine the added value of MR imaging as compared with sonography alone. This study is part of an ongoing project with prolonged clinical and MR follow-up. Here we present preliminary neuroradiologic observations. Until long-term clinical outcome is determined, the significance of the impact of MR imaging as compared with sonography alone cannot be judged.
Methods
Infants
Infants admitted to the neonatal intensive- or high-care unit of our hospital between February 1995 and November 1997 were included in the study if areas of increased echogenicity (also called densities or flares), with or without cysts, were seen bilaterally in the periventricular white matter in two sonographic planes. Additional germinal matrix hemorrhages, intraventricular hemorrhages, and lesions of the basal ganglia or thalamus were allowed. All other forms of sonographic abnormalities, such as hydrocephalus, congenital malformations, and unilateral infarctions, were excluded. Other exclusion criteria were any signs of systemic disease with potential negative influence on neurologic development, and retinopathy grade 3 or more according to the International Classification of Retinopathy of Prematurity (34). Informed consent was obtained from the parents, and the study was approved by the institutional review board of our hospital.
Fifty-three neonates were initially included in the study. Three of them were excluded from this particular part of the study, because sonography was not performed within 24 hours of neonatal MR imaging. The gestational age (GA) at birth of the remaining 50 infants was 31.3 weeks ± 2.6 (mean ± SD), with an age range of 27 to 37 5/7 weeks: 48 infants were born prematurely (< 37 weeks) and two infants were born at term. Mean birth weight was 1550 g ± 470, with a range of 765 to 4040 g.
Sonography
Cerebral sonography was performed within the first 48 hours of life and repeated at least twice a week from birth until discharge or transfer to another hospital, within 24 hours of the day of MR examination, and at 40 weeks' postconceptional age (PCA). The mean number of sonographic examinations per infant was 10 ± 5.6. Seventeen infants had additional germinal matrix hemorrhages and nine infants had additional basal ganglia or thalamus lesions on sonograms. The examinations were performed by the same experienced sonographer, using an Aloka 2000 scanner with a multifrequency (7.5 to 10 MHz) transducer. Scanning was performed in coronal and parasagittal planes through the anterior fontanel. Sequential sections were obtained according to Levene et al (35). Sonograms were independently reviewed by two of the authors; in cases of initial disagreement, a consensus was reached.
Sonograms were scored twice. The first score described sonographic findings up to the day of MR imaging; the second score was the definitive score after the final sonographic examination at term. The sonographic grading system was adapted from De Vries et al (2): grade 1, short-lasting periventricular densities, persisting less than 7 days; grade 2, prolonged periventricular densities, persisting 7 days or more (PVL grade 1); grade 3, periventricular densities, evolving into small localized cysts (PVL grade 2); grade 4, periventricular densities, evolving into extensive periventricular cystic lesions (PVL grade 3); and grade 5, densities extending into the subcortical white matter, evolving into extensive periventricular and subcortical cystic lesions (PVL grade 4).
Presence of the flares was assessed for the frontal, parietal, occipital, and temporal white matter separately. The degree of echogenicity of the periventricular white matter was specified as follows: grade 0, normal echogenicity; grade 1, moderately increased echogenicity, the affected region or smaller areas within the affected region being almost as bright or as bright as the choroid plexus; grade 2, seriously increased echogenicity, the affected region or smaller areas within the affected region being obviously brighter than the plexus.
Cysts were identified as areas of low echogenicity of at least 2 mm in diameter. Increased echogenicity and cysts had to be visible both in coronal and parasagittal planes.
The flares were assessed for homogeneity. An inhomogeneous aspect was considered to be present when an irregular mixture of hyperdense and hypodense areas was observed within the affected region.
MR Imaging
Neonatal MR imaging was performed as soon as the infants were in a stable respiratory and circulatory condition, before they reached a PCA of 40 weeks. For 48 of the 50 infants included, mean postnatal age at MR imaging was 20 days ± 12, with a range of 3 to 53 days. Two prematurely born infants were referred to our hospital after several weeks because of sonographic abnormalities; MR imaging was performed at the postnatal ages of 72 and 99 days, respectively. The infants were sedated with chloral hydrate (75 mg/kg) orally, their heart rate and transcutaneous oxygen saturation were monitored, and supplemental oxygen was administered when necessary.
Imaging was performed on a 1.5-T MR system. A circularly polarized knee coil was used, specially adapted for imaging small heads of preterm infants. The images were acquired with a 128 × 256 or 256 × 256 matrix, a field of view of 18 to 20 cm2, and a section thickness of 4 to 5 mm. T1-weighted spin-echo (SE) images (480/20/2 [TR/TE/excitations]) were obtained in the sagittal and axial planes. Inversion recovery images (4000/30, TI = 800) and T2-weighted SE images (3000/30,60,120/1) were obtained in the axial plane.
The images were assessed for presence of a zone of changed signal intensity within the periventricular white matter relative to the remainder of the cerebral hemispheric white matter. These signal intensity changes were described in our previous study (32) and were classified into 2 grades: grade 1, no zone of changed signal intensity, the signal of the periventricular white matter being similar or almost similar to the signal intensity of the remainder of the cerebral white matter; and grade 2, a zone of changed signal intensity within the periventricular white matter, appearing decreased on T1-weighted images and increased on T2-weighted images.
Hemorrhagic lesions were defined as areas with an increased signal intensity on T1-weighted images and decreased signal intensity on T2-weighted images (11, 36) in regions that are not normally myelinated at this age (37), as myelin deposition leads to similar signal changes. We classified the hemorrhagic lesions as small punctate hemorrhages, larger focal hemorrhages, and extensive hemorrhages affecting at least three cerebral lobes.
Cystic lesions were defined as areas with signal intensity identical to that of CSF on all pulse sequences. Lesions were considered precystic when the signal intensity was close but not identical to CSF on all pulse sequences.
Images were reviewed independently by two of the authors; in case of initial disagreement, consensus was reached.
We drafted an MR scoring system to rate increasingly severe changes in the white matter, similar to the sonographic grading system: grade 1, normal MR findings; grade 2, periventricular zone of changed signal intensity; grade 3, few (≤ 6) punctate hemorrhages in the white matter; grade 4, multiple (> 6) punctate hemorrhages in the white matter and/or small periventricular cysts and/or a few larger focal hemorrhages; grade 5, extensive signal intensity changes with hemorrhagic or (pre)cystic lesions in the periventricular white matter, with, at most, focal subcortical extension; and grade 6, diffuse signal intensity changes with hemorrhagic or (pre)cystic lesions involving both periventricular and subcortical white matter. Whenever characteristics of more than one MR grade were found, the highest score was used. Autopsy reports were available for two patients.
Results
Comparison of Sonograms and MR Images Obtained on the Same Day
The children were classified according to the highest sonographic grade up to the day of MR imaging (Fig 1). Twenty-three infants had sonographic grade 1, 15 had sonographic grade 2, four had sonographic grade 3, and eight had sonographic grade 4. None of the children had sonographic grade 5 on the day of MR imaging.

FIG 1. Neonatal MR score versus initial sonographic (US) score (n = 50). Solid circles represent infants with the same initial and end sonographic score; open circles, infants with a difference between initial and end sonographic scores
Among the 23 children with sonographic grade 1, one infant had normal MR findings. Sixteen infants had a periventricular zone of changed signal intensity on MR images (Fig 2); in three infants, this zone could not be evaluated because of the presence of extensive hemorrhages or cystic lesions. Thirteen infants had hemorrhagic lesions. Ten of them showed few or multiple small punctate hemorrhages, which occurred in both the periventricular and the subcortical areas (Fig 3); in one infant, this was in combination with a larger focal hemorrhage. The remaining three infants had extensive periventricular hemorrhagic lesions (one infant) or extensive hemorrhages throughout the white matter (two infants). Multiple small periventricular cysts depicted on MR images but not on sonograms were seen in one infant with extensive periventricular hemorrhagic lesions and in one infant, with hemorrhages throughout the white matter (Fig 4).

FIG 2. Infant born at 28 4/7 weeks.
A–D, Transient homogeneous periventricular densities are seen in the frontoparietal region on coronal and parasagittal sonograms at a PCA of 29 2/7 weeks (A). Coronal and parasagittal sonograms at a PCA of 34 4/7 weeks (B) show normalized echogenicity of the white matter with a homogeneous aspect. Axial T1-weighted (C) and T2-weighted (D) MR images on the same day show a frontal and parietal periventricular zone of mildly changed signal intensity.

FIG 3. Infant born at 34 2/7 weeks.
A–C, Parasagittal sonogram at a PCA of 35 5/7 weeks (A) shows periventricular densities with an inhomogeneous aspect in the frontoparietal region. T1-weighted MR images on the same day in the parasagittal (B) and axial (C) planes show multiple, small, punctate hemorrhages, occurring in the periventricular white matter on both sides.

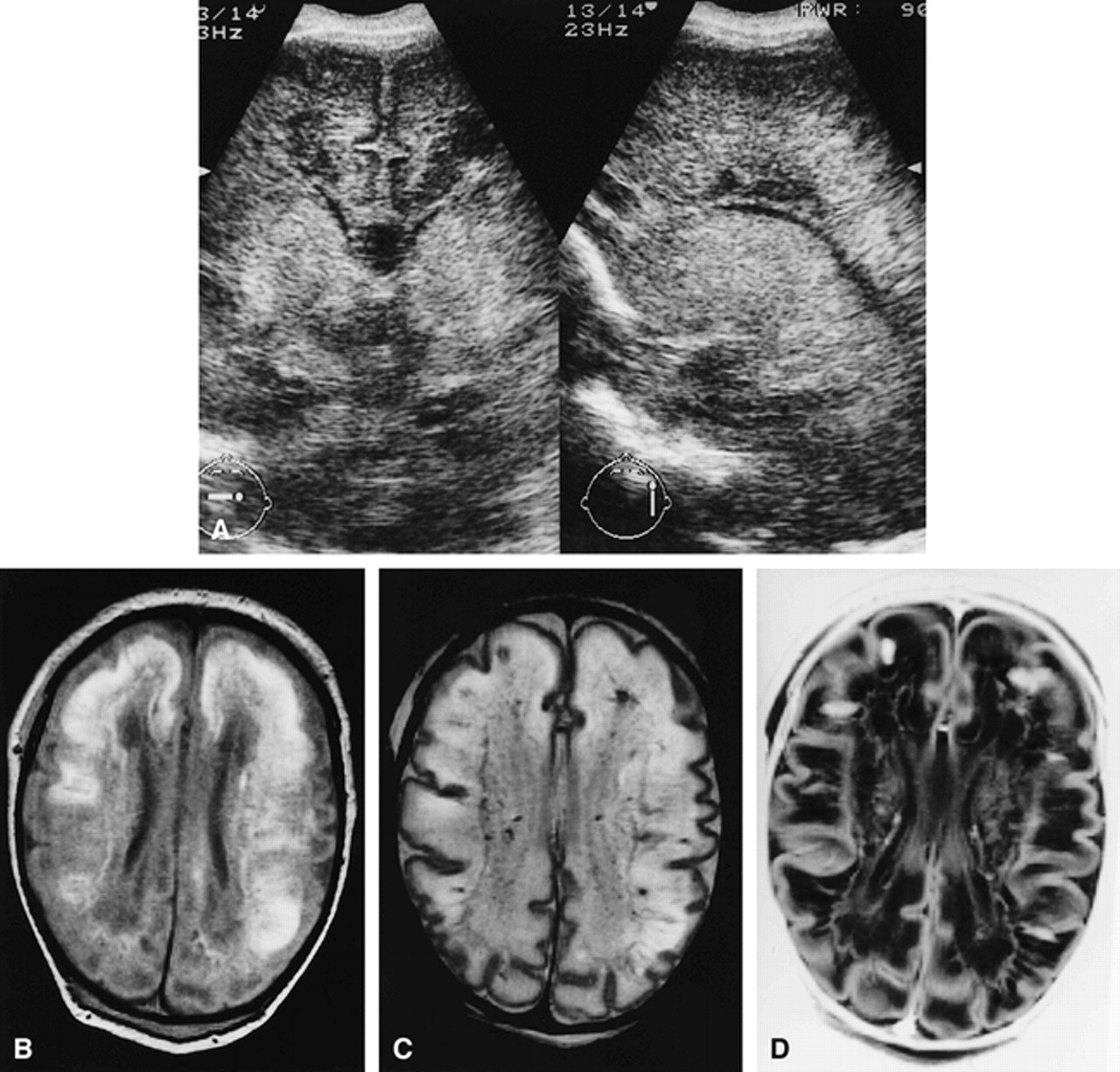
FIG 4. Infant born at 37 3/7 weeks.
A–D, Coronal and parasagittal sonograms (A) at a PCA of 38 2/7 weeks show a diffuse increased echogenicity throughout the white matter and basal ganglia with an inhomogeneous, partly precystic aspect in the frontal region. Proton density–weighted (B), T2-weighted (C), and inversion recovery (D) MR images in the axial plane show large areas of high signal on the proton density–weighted image (B) and combined high and low signal changes on the T2-weighted and inversion recovery images throughout the white matter (C, D) and basal ganglia (D). In comparison with sonograms, MR images show more extensive, small, partly cystic and partly precystic periventricular lesions in the frontal and parietal region, with signal intensities identical or close to CSF (B–D). The hemorrhagic ischemic areas correspond to the large cystic lesions detected at autopsy performed 4 days later.
Among the 15 infants with sonographic grade 2, four had normal MR findings. Eight infants had a periventricular zone of signal change. Nine infants had hemorrhagic lesions on MR images, of whom three had a few and five had more numerous periventricular punctate hemorrhages, in one also affecting the subcortical region. The remaining infant had strikingly asymmetrical lesions on both sonograms and MR images. MR imaging showed unilateral extensive hemorrhagic lesions in a large region of the white matter and periventricular punctate hemorrhages on the other side (Fig 5). In addition, unilateral lesions were present in the basal ganglia on the same side as the extensive white matter lesions.

FIG 5. Infant born at 37 6/7 weeks.
A and B, Coronal sonogram (A) at a PCA of 39 weeks shows a strikingly asymmetrical increased echogenicity of the periventricular white matter, predominantly in the left parietal region, with an inhomogeneous aspect. In addition, intraventricular and germinal-layer hemorrhages were present. T1-weighted MR image on the same day in the axial plane (B) shows extensive signal intensity changes and hemorrhagic lesions throughout the left hemisphere and a small periventricular hemorrhage on the other side.
Among the four children with sonographic grade 3, none had normal MR findings. Two infants had a periventricular zone of changed signal intensity; in one infant, the presence of this zone could not be evaluated because of extensive hemorrhagic and cystic lesions. In one infant, sonograms showed a small localized cyst in the periventricular white matter, which was also seen on MR images. Two infants had multiple punctate hemorrhages on MR images; one in combination with a few small periventricular cystic lesions and one in combination with large periventricular cysts on one side. One infant had extensive signal intensity changes of the white matter with multiple hemorrhages and more extensive periventricular cystic lesions on MR images (Fig 6).

FIG 6. Infant born at 32 weeks.
A and B, Parasagittal sonogram (A) at a PCA of 33 4/7 weeks shows a (stable) posthemorrhagic ventricular dilatation and a moderately increased echogenicity of the white matter in the parietooccipital region with an inhomogeneous aspect and few small cystic lesions. Axial T1-weighted MR image on the same day (B) shows extensive white matter signal intensity changes with multiple hemorrhagic lesions and more numerous cystic lesions.
Among the eight children with sonographic grade 4, none had normal MR findings. Two infants had a periventricular zone of changed signal intensity; in four infants the presence of this zone could not be evaluated because of extensive hemorrhagic and cystic lesions. Seven infants had hemorrhagic lesions; six of them had multiple punctate hemorrhages and one had extensive hemorrhages throughout the white matter. All infants had multiple, large, periventricular cysts on MR images, with focal extension into the subcortical region in four of them (Fig 7). Two infants had strikingly asymmetrical lesions on sonography. MR imaging showed unilateral extensive hemorrhagic and cystic lesions in a large region of the white matter and periventricular punctate hemorrhages on the other side. In addition, unilateral lesions were present in the basal ganglia in these two infants on the same side as the extensive white matter lesions.
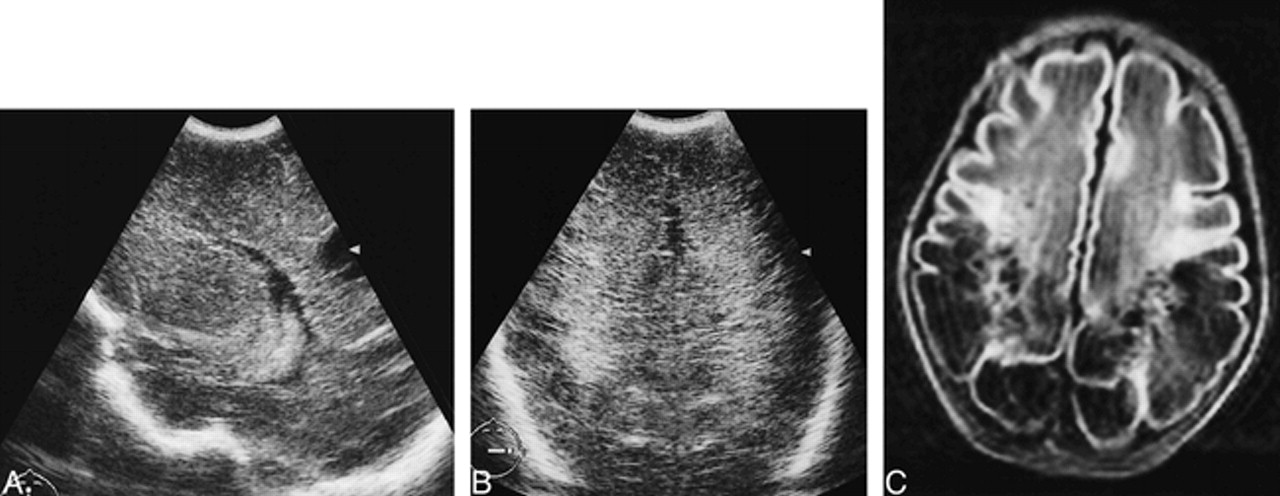
FIG 7. Infant born at 34 5/7 weeks.
A and B, Parasagittal (A) and coronal (B) sonograms at a PCA of 36 5/7 weeks show a moderately increased echogenicity of the periventricular white matter with a homogeneous aspect and one large cyst in the parietal region. Axial T1-weighted MR image on the same day (C) shows more numerous, bilateral, large periventricular cysts on MR images, with focal extension into the subcortical white matter in the entire parietooccipital region.
Overall, the extra information provided by MR imaging consisted of the demonstration of hemorrhagic lesions in 64% of the infants (32/50). In the majority of the children, the hemorrhagic lesions were distributed along the ventricles in the frontoparietooccipital regions, but hemorrhages were frequently found in the subcortical white matter as well. In a few infants, there were larger focal hemorrhages located at the frontal and occipital external angles of the lateral ventricles. In the cystic PVL group, MR images showed more numerous or more extensive cysts than the sonograms did in 75% of the infants (9/12). In addition, we found cysts on MR images in two infants in whom sonograms showed no cysts at all. In 32% of the infants (16/50) MR imaging provided no additional information over sonography alone. Fifteen of these children had flares on sonograms, while MR images showed no abnormalities or only a zone of mild periventricular signal change. The remaining infant had a small cystic lesion revealed by both sonography and MR imaging.
The degree of echogenicity and the presence or absence of inhomogeneity of the flares on sonograms were compared with the presence and the extensiveness of MR lesions. Flares with a homogeneous aspect (n = 15) were associated with no or minimal MR lesions. This was independent of whether the echogenicity score was 1 or 2. Eleven infants had a periventricular zone of changed signal intensity. Focal MR lesions were present in only five infants, and consisted of a few punctate hemorrhages, a small focal hemorrhage, or a small solitary cyst. Inhomogeneity of the flares (n = 35) was associated with hemorrhagic lesions on MR images in 80% of the children. In the infants with inhomogeneous flares and an echogenicity score of 2, numerous punctate and extensive hemorrhages were more often present (10/11 infants) than in the group with an echogenicity score of 1 (9/24 infants). A periventricular zone of changed signal intensity was present in 17 of the 35 infants, but often the presence or absence of this zone could not be evaluated because of hemorrhagic and cystic lesions. Of the infants with inhomogeneous flares and an echogenicity score of 1, 25% had multiple cystic lesions; and in those with inhomogeneous flares and an echogenicity score of 2, 58% had multiple cystic lesions.
In 92% of the children, the locations of the lesions on sonograms and MR images were almost or entirely identical. In 35% of the children, more lesions were seen on MR images, either in the subcortical region or other lobes. In 8% of the children, there was no agreement between sonography and MR imaging. These children had homogeneous flares on sonograms and normal MR findings.
Neonatal MR Score as Compared with Sonographic End Diagnosis
Forty-eight of the 50 infants came for sonography at term date, allowing a definitive sonographic diagnosis. The other two children did not survive the neonatal period. The definitive sonographic diagnosis was based on the most serious degree of abnormality during the neonatal period. The neonatal MR score was compared with this sonographic end diagnosis to evaluate its predictive value. The scores are shown in Figure 8.

FIG 8. Neonatal MR score versus sonographic (US) end score (n = 48). Solid circles represent infants with the same initial and end sonographic score; open circles, infants with a difference between initial and end sonographic scores; cross, infants who did not survive the neonatal period
Among the 36 infants with no, mild, or moderate MR abnormalities (MR score, 1 to 4), only four (11%) had a higher sonographic end score than initial score (Fig 8). Among the 14 infants with severe MR abnormalities (MR score, 5 and 6), seven (50%) had a higher sonographic end score than initial score. Two of these infants had an initial sonographic score of 1 and did not survive the neonatal period; the large cystic lesions found at autopsy suggested that the sonographic end score would have been 5. Multicystic leukomalacia developed in all four infants with an MR score of 6.
Autopsy reports were available for two infants with an initial sonographic score of 1 and an MR score of 6. Autopsies were performed 4 and 11 days, respectively, after MR imaging. Because rapid changes may follow hypoxic-ischemic events, exact correlation may be difficult. The first infant had a GA of 32 6/7 weeks at birth, and autopsy was performed 3 weeks later, 11 days after MR imaging. The findings included extensive cavitation of the cerebral white matter, more pronounced in the occipital and temporal lobes and less in the frontal lobes. The cystic lesions were filled with macrophages. The thalami showed a marked gliosis, neuronal loss, and microcalcifications. The cerebral cortex, hippocampus, basal ganglia, brain stem, and cerebellum were normal. The second infant had a GA of 37 3/7 weeks at birth, and autopsy was performed 2 weeks later, 4 days after MR imaging (Fig 4). The findings included cavitation lesions filled with macrophages throughout the cerebral white matter, with the majority in the frontoparietal region. In the occipital white matter, rarefaction, gliosis, and microcalcifications were present. In the putamen and caudate nucleus, extensive neuronal loss was observed. The thalamus exhibited many encrusted neurons. The cerebral cortex, hippocampus, brain stem, and cerebellum showed no structural changes. In both infants, the findings were compatible with a multicystic leukomalacia, with additional central gray matter damage, in conformity with the MR abnormalities.
Overall, the early MR findings were predictive of the final sonographic score. In all 12 surviving infants with extensive white matter lesions on MR images (MR score, 5 and 6), the extent and severity of the MR lesions were comparable to the final sonographic diagnosis (sonographic end score, 4 to 5). The majority of these infants had extensive hemorrhages in the periventricular and/or subcortical white matter on MR images, whereas the initial sonographic score, obtained on the same day as the MR score, had not suggested this. None of the 36 infants with no, mild, or moderate MR abnormalities (MR score, 1 to 4) had (new) cystic lesions on follow-up sonography. In two infants, the small cystic lesions, present on initial sonograms and MR images, did not change in size.
Discussion
In the present study, the most important advantage of early MR imaging in neonates was that it allowed better differentiation of abnormalities at an earlier stage than did sonography. In reviewing our results, it is clear that MR imaging provided the most important information in the group of infants with noncystic echodensities. Whereas sonography showed only periventricular densities, related MR abnormalities varied from subtle to extensive changes in signal intensity, frequently with multiple periventricular and subcortical hemorrhages in the white matter. The presence of cysts, as shown by sonography, was always confirmed by MR imaging, although MR images often showed more numerous and more extensive cysts. These early neonatal MR findings were predictive of the final sonographic score. In particular, extensive hemorrhages and signal intensity changes on MR images preceded development of a cystic PVL or multicystic leukomalacia.
A frequent finding on MR images was a periventricular zone of mildly changed signal intensity. However, in infants with more extensive cysts or hemorrhages, the presence or absence of this zone was difficult to evaluate. It is likely that the periventricular zones of changed signal intensity corresponded to the periventricular densities on sonograms, as suggested by van Wezel et al (32), and that these periventricular signal abnormalities represent mild ischemic changes of the periventricular white matter. In clinical follow-up studies, the majority of the children with a periventricular zone of changed signal intensity had mild transient disturbances in tone (38) or had normal findings (28).
Generally, hemorrhagic PVL is considered to be relatively rare (39–42) and is associated with poor prognosis. However, in the majority of our children (64%), MR imaging showed punctate or more extensive hemorrhages within the area of leukomalacia. The same phenomenon was also found by Keeney et al (27). Considering the high frequency with which the hemorrhagic aspect of PVL is observed, it is questionable whether the assumed poor prognosis is justified.
In three infants, bilateral but strikingly asymmetric hemorrhagic lesions were found in the periventricular white matter, in association with hemorrhages in the basal ganglia on the side of the most severe lesions. The question is whether this is a highly asymmetrical, hemorrhagic PVL or a unilateral venous infarction associated with some contralateral PVL. There is considerable controversy concerning the differentiation between these lesions (43, 44), and it is not impossible that they are variants of the same entity.
DiPietro et al (45) showed that irregular patchy inhomogeneous flares correlate with hemorrhagic lesions at autopsy, but others have found that both hemorrhagic and nonhemorrhagic PVL can produce identical changes on sonograms (46). We found that all but two infants with inhomogeneous flares lasting longer than 7 days had evidence of hemorrhagic lesions in the white matter on MR images. Furthermore, cystic lesions developed in most infants with inhomogeneous flares and white matter echogenicity brighter than that of the plexus. Considering our sonographic results, an irregular, inhomogeneous aspect of the flares is an important finding that is associated with more severe MR abnormalities than are homogeneous flares. Therefore, we propose to adapt the sonographic grading system incorporating the inhomogeneous noncystic PVL as a separate item (Table).
Modified sonographic grading system*
We found an overall agreement between the locations of the lesions on sonograms and on MR images, but the MR images showed more extensive lesions in the subcortical white matter and depicted lesions in other lobes. The superiority of MR imaging over sonography in the detection of hypoxic-ischemic brain injury has also been suggested by several other investigators (27, 30). In only a few infants did sonography provide more information. These infants had homogeneous flares with a moderately increased echogenicity on sonograms, and no lesions on MR images. All these infants were born very prematurely (< 29 weeks). According to Carson et al (4), such flares may represent a normal phenomenon in extremely premature neonates.
Conclusion
It is clear that sonography remains the most easily available and repeatable diagnostic tool for PVL in the neonatal period. It is true that, with this technique, it can be difficult to differentiate a normal periventricular halo from a homogeneous flare, but we found that the absence or presence of a homogeneous flare is probably not a very important concern. Such flares were associated with no or at most minimal MR abnormalities. In contrast, in infants with inhomogeneous flares, MR imaging provided important additional information about the presence and extent of hypoxic-ischemic brain damage. In this study, early MR imaging was a good predictor of the sonographic end diagnosis. None of the infants in our study with no or mild MR abnormalities developed cystic lesions, whereas all infants with extensive MR abnormalities in the white matter developed cystic leukomalacia. In this stage, without the data of clinical follow-up available, it is difficult to decide which neonates should undergo MR imaging. In light of our findings, we recommend that MR imaging be performed in infants with inhomogeneous flares. Of course, a single MR study cannot provide information about possible brain damage due to hypoxic-ischemic incidents occurring after MR imaging. In diagnosing acute PVL, a combination of serial sonography and single MR imaging provides the most valuable information.
Acknowledgments
We are grateful to Wouter Kamphorst, Department of Pathology, for providing neuropathologic reports of two infants.
Footnotes
1 Supported by Beatrix Fonds (No. 93–002).
2 Presented in part at the meeting of the European Society of Magnetic Resonance in Neuropediatrics, Amsterdam, December 1997; and at the meeting of the International Child Neurology Association, Ljubljana, Slovenia, September 1998.
↵3 Address reprint requests to M. S. van der Knaap, MD, Department of Child Neurology, University Hospital of the Vrije Universiteit De Boelelaan 1117, 1081 HV Amsterdam, the Netherlands.
References
- Received February 10, 1999.
- Copyright © American Society of Neuroradiology
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cerebral ultrasound abnormalities in infants born to mothers with autoimmune disease
- Limitations of ultrasonography for diagnosing white matter damage in preterm infants
- Magnetic resonance imaging of preterm brain injury
- Practice parameter: Neuroimaging of the neonate: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society
- Ultrasound diagnosis and neurodevelopmental outcome of localised and extensive cystic periventricular leucomalacia