
Abstract
Summary: We present an autopsy case of primary leptomeningeal melanoma visualized with technetium-99m-hexamethylpropyleneamine oxime (Tc-99m-HMPAO) single photon emission CT (SPECT) of the brain. Increased uptake of Tc-99m-HMPAO coincided with leptomeningeal enhancement on MR images and with the tumor location of the autopsy findings. It was thought that Tc-99m-HMPAO could correlate closely with melanoma. Tc-99m-HMPAO SPECT clearly showed primary leptomeningeal melanoma and severe hypoperfusion induced by intracranial hypertension and tumor proliferation.
Primary leptomeningeal melanoma of the CNS is a rare and highly aggressive neoplasm with poor prognosis (1, 2). It is hypothesized that primary leptomeningeal melanoma derives from malignant transformation of leptomeningeal melanocytes within leptomeninges at the cerebral convexity, base of the brain, brain stem, or spinal cord (1–3). The tumor cells rapidly invade along the pia mater and spread into the whole subarachnoid space (1). MR imaging is very useful for the detection, visualization, and diagnosis of this disease (2). Intracranial malignant melanomas can be detected by single photon emission CT (SPECT) of the brain, which shows malignant melanomas as increased accumulation (2, 4, 5). In this report, we present an autopsy case of primary leptomeningeal melanoma visualized with technetium-99m-hexamethylpropyleneamine oxime (Tc-99m-HMPAO) SPECT of the brain.
Case Report
A 24-year-old man with severe morning headache and vomiting was admitted to our hospital for investigation and treatment. Neurologic examinations performed at admission revealed severe headache and nuchal rigidity. The patient was alert and well oriented. Motor tests and sensory examinations revealed no neurologic deficits. Laboratory tests revealed no remarkable changes involving acute inflammation. T1- and T2-weighted MR images of the brain showed slightly ventricular enlargement, indicating acute hydrocephalus and slight swelling in the left frontal lobe. Contrast-enhanced T1-weighted MR images showed slightly leptomeningeal enhancement along the left frontal lobe. Lumbar puncture showed clear CSF and an increased intracranial pressure of 40 cmH2O. CSF examination found a cell count of 24/3 mm3, protein content of 59 mg/dL, and glucose level of 38 mg/dL. Cytology of the CSF showed no tumor cells (class II). Bacterial, fungal, or viral infection was not observed. SPECT of the brain with Tc-99m-HMPAO (740 MBq) was performed for the evaluation of brain perfusion. SPECT of the brain showed slightly increased uptake of Tc-99m-HMPAO in the left frontal cortex and normal perfusion except for the left frontal cortex.
Ventricular drainage was performed because the intracranial hypertension due to acute hydrocephalus was progressing rapidly. At that time, corticomeningeal biopsy was also performed to confirm the diagnosis. At surgery, the appearance of the leptomeninges presented the appearance of black tumor. Based on the operative finding, primary or metastatic malignant melanoma was suspected. Histopathologic examination (Fig 1A) revealed atypical cells with melanin granules. Tumor cells diffusely invaded along the pia mater and spread into the subarachnoid space. Chemical and radiologic examinations of the extracranial organ did not show any other tumors suggesting malignant melanoma. The intracranial disease was diagnosed as a rare primary leptomeningeal melanoma. Thereafter, a ventriculoperitoneal shunt operation was performed. As adjuvant therapy for the leptomeningeal melanoma, chemotherapy using dacarbazine, nimustin hydrochloride, and vincristine was administered; however, chemotherapy had no effect on the tumor.

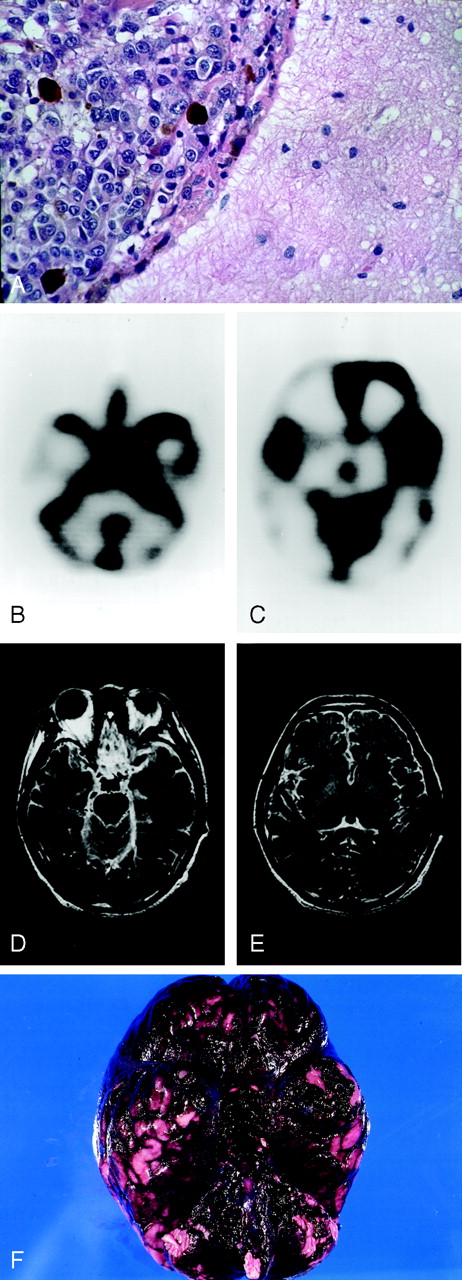
Images from the case of a 24-year-old man with primary leptomeningeal melanoma.
A, Photomicrograph (hematoxylin and eosin stain; original magnification, ×200) from the corticomeningeal biopsy shows the atypical cells with melanin granules. Tumor cells diffusely invaded along the pia mater and spread into the subarachnoid space, indicating a leptomeningeal melanoma.
B, SPECT scan of the brain, obtained during the terminal state, shows increased uptake of Tc-99m-HMPAO in the basal cistern and cisterns surrounding the brain stem, both cerebellar hemispheres, and both sylvian fissures.
C, SPECT scan of the brain shows severe hypoperfusion in the cerebral and cerebellar hemispheres, especially in the brain stem, both cerebellar hemispheres, and thalami.
D and E, Contrast-enhanced T1-weighted MR images (600/16/1 [TR/TE/NEX]), obtained during the terminal state, show thick and diffuse leptomeningeal enhancement in the whole leptomenigeal and subarachnoid space.
F, Macroscopic appearance at the base of the brain. The brain is thickly and diffusely covered with black tumors, indicating the primary leptomeningeal melanoma.
Four months after onset, the patient experienced disturbance of consciousness. Tc-99m-HMPAO SPECT and MR imaging were again performed. SPECT of the brain (Fig 1B and C) showed increased uptake of Tc-99m-HMPAO in the whole subarachnoid space, especially in the basal cisterns, cisterns surrounding the brain stem and cerebellar hemispheres, and both sylvian fissures. Also, severe hypoperfusion in the whole brain was noted on the SPECT scans. MR images showed a linear band of slightly shortened T1 relaxation time in the surface of the brain and brain stem. Contrast-enhanced T1-weighted MR images (Fig 1D and E) showed thick and diffusely leptomeningeal enhancement along the whole leptomeninges and subarachnoid space. The patient died approximately 5 months after onset as a result of rapidly progressive worsened conditions.
At autopsy, macroscopic appearances of the brain (Fig 1F) and spinal cord were thickly and diffusely covered with black tumors. Histopathologic examination revealed that the whole subarachnoid space, Virchow-Robin space, and all ventricular walls were filled with melanoma cells. The superficial cerebral parenchyma was directly infiltrated from the leptomeninges. Malignant melanoma was not found in the skin or the extracranial organs, except for shunt-carried dissemination in the peritoneum and omentum. The final diagnosis was primary leptomeningeal melanoma.
Discussion
Tc-99m-HMPAO, as a lipophilic agent, consists of macrocyclic amine radicals and is the brain perfusion tracer for regional cerebral blood flow with SPECT (6). HMPAO freely passes the normal blood-brain barrier. It is transformed to hydrophilic form, which is retained in the cells. This mechanism of HMPAO uptake in the normal brain is proposed to be dependent on glutathione (7). Tc-99m-HMPAO has been widely used to evaluate regional cerebral blood flow in cases of brain disease. On the other hand, it has been known that Tc-99m-HMPAO is uncommonly accumulated in the brain tumors (8). This mechanism is not clear, but it is supposed that high vascularity and/or glutathione lead to Tc-99m-HMPAO uptake in the brain tumors (8).
In our case of malignant leptomeningeal melanoma, this disease was clearly detected and visualized with Tc-99m-HMPAO SPECT. Increased uptake of Tc-99m-HMPAO was observed mainly during the terminal state in the whole subarachnoid space, especially in the basal cisterns, cisterns surrounding the brain stem and cerebellar hemispheres, and both sylvian fissures. The location of Tc-99m-HMPAO accumulation coincided with the leptomeningeal enhancement on MR images and the tumor location of the autopsy findings. It was thought that Tc-99m-HMPAO could correlate closely with melanoma. In the literature on SPECT study of malignant melanoma, there is only one report of Tc-99m-HMPAO accumulation in primary extracranial malignant melanoma (9). To our knowledge, this is the first report of increased uptake of Tc-99m-HMPAO in primary intracranial malignant melanoma. Melanoma cells have many amine receptors (5, 9) and contain high glutathione (10, 11). Ryu et al (9) supposed that the mechanism of Tc-99m-HMPAO uptake in cases of malignant melanoma is associated with increased tumoral vascularity, glutathione, and many amine receptors. A similar mechanism was also suggested in our case. Tc-99m-HMPAO may be useful for the detection and visualization of primary malignant melanoma.
In the brain perfusion of this patient, Tc-99m-HMPAO SPECT performed during the terminal state showed diffuse and severe hypoperfusion of cerebral parenchyma. Primary leptomeningeal melanoma of the CNS in this case was the diffuse type that invaded along the pia mater and spread into the subarachnoid space (1). It was supposed that severe intracranial hypertension due to the tumor proliferation rapidly and aggressively caused cerebral hypoperfusion. Tc-99m-HMPAO SPECT was also helpful for the evaluation of regional cerebral blood flow changes and the patient’s prognosis.
MR imaging is useful for the detection, visualization, and diagnosis of leptomeningeal melanoma. The characteristic MR imaging appearance of melanomas includes shortening of T1 and T2 relaxation times caused by the paramagnetic free radicals into melanin (12). In our case, MR images obtained during the terminal stage clearly showed the typical shortening of T1 relaxation time and thick and diffuse contrast enhancement in the whole leptomeninges and subarachnoid space. Contrast-enhanced T1-weighted MR imaging is the best imaging for the detection and visualization of primary or metastatic leptomeningeal melanomas (2). In our case, MR images other than T1-weighted and contrast-enhanced T1-weighted images could not be obtained. If diffusion-weighted or T2-weighted MR images could have been obtained, the hypoperfused areas on the second SPECT scans might have been shown as cerebral ischemia.
Conclusion
Tc-99m-HMPAO SPECT clearly showed primary leptomeningeal melanoma and severe hypoperfusion induced by intracranial hypertension and the tumor proliferation in the whole brain. Tc-99m-HMPAO SPECT revealed the connection of tumor proliferation with cerebral circulation during the terminal state of primary leptomeningeal melanoma.
References
- Received July 23, 2001.
- Accepted after revision November 26, 2001.
- Copyright © American Society of Neuroradiology





{kind=link}