
Abstract
BACKGROUND AND PURPOSE: Although previous brain imaging studies of Wilson disease (WD) focused on the dopaminergic system, correlational data on the integrity of the pre- and postsynaptic compartments are lacking. The present study was initiated to intraindividually determine the integrity of these compartments in patients with WD.
METHODS: A total of 46 patients with WD and 10 matched control subjects underwent [123I]2β-carbomethoxy-3β-(4[123I]iodophenyl)tropane ([123I]β-CIT) and [123I]iodobenzamide ([123I]IBZM) single photon emission CT (SPECT). For both radiotracers, specific striatal binding ratios (with the cerebellum as the reference region) were calculated after a standardized region-of-interest technique was applied. In addition, the severity of putative neurologic symptoms was evaluated by using a linear scoring system.
RESULTS: In patients without neurologic symptoms, striatal binding ratios of both radiotracers did not differ from those of the control group (13.8 ± 3.1 vs 12.0 ± 3.4 and 2.00 ± 0.19 vs 1.90 ± 0.27; n.s.). In symptomatic patients, however, striatal binding ratios for both [123I]β-CIT and [123I]IBZM were significantly reduced (9.1 ± 2.3 and 1.64 ± 0.18; P < .001). In all patients with WD, the [123I]β-CIT and [123I]IBZM binding ratios were significantly correlated (r = 0.65, P < .001), as were SPECT parameters and the severity of the neurologic symptoms (r = −0.60 and −0.62; P < .001).
CONCLUSION: These findings of a concordant bicompartmental dopaminergic deficit in neurologic WD provide in vivo evidence for assigning WD to the group of secondary Parkinsonian syndromes. These results could be relevant in therapeutic decision making in patients with this copper deposition disorder.
In Wilson disease (WD), a genetically defined but effectively treatable copper deposition disorder, cerebral manifestation may be expressed as rigidity, tremor, dyskinesia, and dysarthria (1). Because of these complaints and because of the deposits of the surplus copper predominantly found in the striatal regions of the brain (2), WD has been assigned to a group of diseases known as the secondary Parkinsonian syndromes. With respect to the dopaminergic neurotransmission, these syndromes are generally characterized by alterations of both the pre- and postsynaptic pathways (3).
Although a number of previous brain imaging studies of WD have focused on the dopaminergic system (4–9), the literature lacks data on the intraindividual correlations of the integrity of the pre- and postsynaptic compartments. The present study was initiated to investigate these features with a view to further improve the understanding of the disease.
Methods
Forty-six patients with WD (21 female, 25 male; ages, 40 years ± 11 [mean ± SD]) were compared with an age- and sex-matched control group comprising 10 subjects (four female, six male; ages, 40 years ± 11) without evidence of dopaminergic or other basal ganglia disorders. WD was diagnosed by using the established [64Cu]copper test (10), the results of which verified pathologically decreased copper incorporation into ceruloplasmin. In all patients with WD, the severity of putative neurologic symptoms (tremor, ataxia, dysdiadochokinesia, dysarthria) was scored by an experienced neurologist, who was blinded to the results of the single photon emission CT (SPECT). An established linear system was used to score symptoms as follows: 0, none; 1, minimal; 2, slight; 3, moderate; and 4, severe (11). In addition, disease duration (defined as time from the onset of symptoms to date of the SPECT scanning) and treatment duration was recorded. In all patients, the clinical and brain SPECT examinations were performed within 7 days (±2 days). At the time of the SPECT studies, all patients had an equivalent or negative copper balance, which was defined as normal serum and urine copper concentrations. They were treated with zinc, d-penicillamine, and triene, either as a single or a combined medication. The study was approved by the local ethics committee, and written informed consent for the SPECT imaging was obtained from all patients.
All patients and subjects were imaged 24 hours after the intravenous administration of 185–200 MBq [123I]2β-carbomethoxy-3β-(4[123I]iodophenyl)tropane ([123I]β-CIT), a radioligand that binds to the presynaptic dopamine transporters in the striatum, and two hours after the intravenous administration of 200 MBq [123I]iodobenzamide ([123I]IBZM), a radioligand that binds to the postsynaptic striatal dopamine D2 receptors. Imaging was performed by using a brain-dedicated Ceraspect camera (DSI, Waltham, MA). The SPECT acquisition and imaging processing has been described in detail elsewhere (12). By applying a region-of-interest method (with the cerebellum as the reference), specific [123I]β-CIT and [123I]IBZM binding ratios of the striatum were obtained.
Statistical analyses were performed by using SPSS (SPSS, Munich, Germany). Differences between the control group and the WD group were tested for significance by applying a one-factorial analysis of variance (ANOVA) and, in a second step, by using the Student t test for independent populations. For all patients with WD, intercorrelations between the striatal [123I]β-CIT and the [123I]IBZM binding ratios, as well as correlations between the SPECT data and the clinical parameters (disease duration, treatment duration, scoring of neurologic symptoms) were tested for linearity. For that, the standardized predicted values were plotted against standardized residuals and correlation calculated by using linear regression analyses. Striatal binding ratios for [123I]β-CIT and [123I]IBZM are codetermined by age effects (13, 14). Therefore, partial correlation analyses were applied to correct for this cofactor. Significance levels were set at P < .05, < .01, and <.001.
Results
No significant lateralization of the obtained striatal [123I]β-CIT or [123I]IBZM binding ratios was observed. Therefore, mean values were calculated from the corresponding left and right hemispheric region-of-interest data.
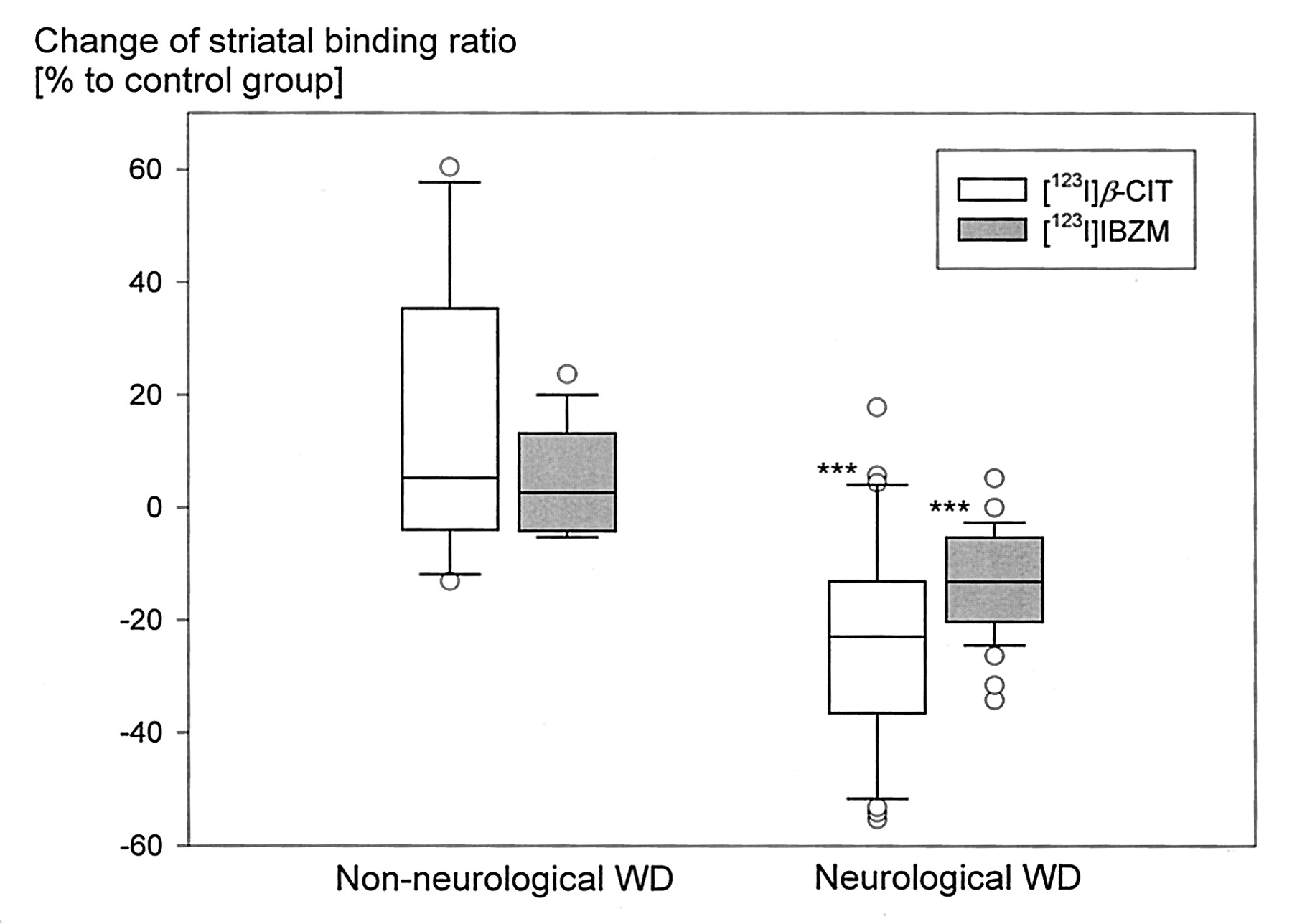
In the WD group, 20 patients (43%) had a neurologic symptom score of 0 (“non-neurologic WD patients”), and 26 patients (57%) had a score of >0 (“neurologic WD patients”). Among the neurologic WD patients, eight (17%) had a score of 1, five (11%) had a score of 2, 10 (22%) had a score of 3, and three (7%) had a score of 4. The mean duration of the disease was 20 years ± 11, and the mean treatment duration was 18 years ± 11. Regarding the striatal [123I]β-CIT and [123I]IBZM binding ratios, significant group differences were found in all subjects examined (P < .001 after one-factorial ANOVA). However, whereas in the non-neurologic WD patients, the striatal binding ratios of both [123I]β-CIT and [123I]IBZM did not differ from those of the control group (13.8 ± 3.1 vs 12.0 ± 3.4 and 2.00 ± 0.19 vs 1.90 ± 0.27; n.s.), the binding ratios of the neurologic WD patients were significantly reduced compared with those of the control subjects (9.1 ± 2.3 and 1.64 ± 0.18; P < .001) (Fig 1). The changes in striatal [123I] β-CIT and [123I]IBZM binding ratios in both groups of patients with WD, as compared with the control group, are illustrated in Figure 2.

Typical examples of [123I]β-CIT (top row) and [123I]IBZM (bottom row) SPECT images in a subject from the control group (left), a non-neurologic WD patient (middle), and a neurologic WD patient (right). Transverse sections at the level of maximal diameter of the striatum are shown. No differences were noted between the control subject and the non-neurologic WD patient. In contrast, specific binding is reduced for both radiotracers in the striata of the neurologic WD patient.

Box plots show the striatal [123I]β-CIT and [123I]IBZM binding ratios in non-neurologic and neurologic WD patients, given in percentages, as related to those in the control group. No differences were noted in the non-neurologic WD patients, but a highly significant deficit was observed in neurologic WD patients. *** indicates P < .001.
In the patients with WD, the striatal binding ratios of [123I]IBZM were positively correlated with the [123I]β-CIT ratios (Fig 3). This correlation was proved to be linear and highly significant (P < .001), with an age-corrected correlation coefficient of r = 0.65. The striatal binding ratios of both [123I]β-CIT and [123I]IBZM were not correlated with disease duration or treatment duration (age-corrected r = −0.12 to 0.33, n.s.). Highly significant negative correlations, however, were found with the scoring of neurologic symptoms (age-corrected r = −0.60 and −0.62; P < .001).

Scatter plot shows the positive correlation between the [123I]β-CIT and [123I]IBZM binding ratios in the striatum of non-neurologic WD patients (solid dots) and neurologic WD patients (open dots). The correlation was proved to be linear and highly significant.
Discussion
The correct execution and control of movement is regulated and coordinated by the basal ganglia and cerebellum via extensive inputs from cortical brain areas, parallel internal circuitry, and projections back to the cortex via thalamic relay nuclei (15). The striatum is the input region of the basal ganglia, and it receives corticostriatal fibers as well as the dopaminergic nigrostriatal projections, which were investigated in the present study. The role of the dopaminergic nigrostriatal projections for realizing motor function is complex. Dopamine has a differential (inhibitory and excitatory) effect on striatal neurons that is mediated by two distinct classes of dopamine receptors: D1-like receptors (D1 and D5) and D2-like receptors (D2, D3, D4) (15). In the striatum, most of the dopaminergic receptors are either D1 or D2 receptors. Whereas D2 receptor stimulation is known to have inhibitory effects on the extrapyramidal motor system, D1 receptor stimulation activates the motor system (15). All together, this complex dopaminergic system facilitates movement, and in case of its deficiency, it causes movement disorders such as Parkinson disease or WD.
The present study was performed to intraindividually investigate the pre- and postsynaptic parts of dopaminergic neurotransmission in vivo in patients with WD. By using a high-resolution brain-dedicated SPECT camera, we found concordant pre- and postsynaptic dopaminergic deficits in patients with neurologic WD, with a strong intercorrelation between the severity of the deficits in the pre- and the postsynaptic compartments.
Applying SPECT and positron emission tomography (PET), several authors have already reported on the alteration of the postsynaptic dopamine D2 receptors in patients with WD (4, 7, 8). In addition, preliminary findings on a presynaptic dopaminergic deficit in WD are reported in the literature (5, 9). We recently specified these findings of other groups by showing that the integrity of the nigrostriatal dopaminergic neurons in the striatum of patients with WD is differentially altered depending on the course and severity of the disease (12).
Until now, only one multiple case report about intraindividually imaging both the pre- and postsynaptic pathways of dopaminergic neurotransmission in WD has been published. In 1995, Westermark et al (6) examined four patients by using [11C]nomifensine PET imaging of the presynaptic dopamine transporters and [11C]raclopride PET imaging of the postsynaptic dopamine D2 receptors. They reported a positive correlation in the obtained data, although they were not able to substantiate the correlation statistically because of the small number of patients. However, in this study, we verified the results of Westermark et al in a larger and more representative population with WD.
The most likely explanation for our findings of concordant pre- and postsynaptic dopaminergic deficits in neurologic WD is copper deposition in the substantia nigra or in the striatum itself. In the present study, we were not able to correlate the SPECT findings with the MR imaging or CT imaging data, which can be used to directly monitor brain copper depositions (16, 17). However, we found that, in WD, the dopaminergic deficits are correlated with the symptoms. These findings are supported by those from a number of other radionuclide imaging studies showing similar correlations not only for the dopaminergic neurotransmission but also for the striatal glucose consumption (5, 7, 8). In addition, a convincing number of reports in the literature about WD show that the severity of neurologic symptoms is correlated with the extent of the brain copper deposition, as measured with MR imaging (2, 7, 18), or with the level of copper in the CSF (also a marker of brain copper accumulation) (19, 20). Altogether, our present results provide further support for the conclusion that the clinical features in WD are directly linked to the cerebral copper deposition.
Interestingly, early reports in the literature suggested that patients with WD could benefit from additional dopamine substitution, in addition to the usual anti-copper medication. In 1970, Barbeau and Friesen suggested the use of l-dopa in patients with WD and a rapid deterioration of neurologic symptoms despite adequate chelation (21). This suggestion was later substantiated by two case reports (22, 23). However, our finding of different degrees of alteration of the dopaminergic synapses in patients with WD suggests that effective l-dopa substitution could not be expected for all patients. In fact, in 1989, Frankel et al (24) applied the apomorphine test in a group of patients with WD. This test is normally used to investigate dopamine responsiveness in patients with Parkinson disease. Here, the authors found that only two of the seven investigated patients had an adequate response. The results in the study by Frankel et al are similar to those of Morgan el al (25) who reported a patient with progressive neurologic WD, in whom the dopaminergic substitution proved to be ineffective as a supplement to penicillamine. Presuming that SPECT or PET can be used to identify the subpopulation of patients with WD who benefit from dopaminergic medication, we can speculate that the described brain imaging procedures could improve decision making in complementary dopaminergic treatment. However, additional prospective studies are required to clarify this hypothesis.
Our finding that the dopaminergic alteration in WD concerns not only the nigrostriatal neurons that produce and release the neurotransmitter into the synaptic gap but also the postsynaptic D2 receptors through which dopamine mediates its effect could lead to the conclusion that potent success with substitutional dopaminergic treatment cannot be expected. This conclusion is supported by 1) the general lack of further reports in the literature (subsequent to the studies cited above) on applying dopaminergic medication in patients with WD and 2) observations showing that substitutional dopaminergic medication is of limited value in other secondary Parkinsonian syndromes, such as multisystem atrophy or progressive supranuclear palsy (26).
If one compares the striatal binding ratios of both [123I]β-CIT and [123I]IBZM in our control group and patient group with the respective values in the literature (13, 14), our values appear to be 20–80% higher. This finding is most likely due to the use of our high-resolution brain-dedicated SPECT system with a circular crystal arrangement close to the skull. Own phantom experiments with both a conventional triple-head gamma camera (Multispect 3; Siemens, Germany) and the Ceraspect system (data not presented) showed not only higher system sensitivity in favor of the latter but also a virtually linear relationship between the target-to-background ratios obtained with both cameras. Hereby, the slope of the regression line equals 0.4–0.6 (depending on the target size, intercept <1). This results in higher target-to-background ratios for the Ceraspect system. Altogether, the brain-dedicated ring system more accurately reflects the true distribution of cerebral activity.
Conclusion
Our findings of a concordant bicompartmental dopaminergic deficit in patients with neurologic WD provide in vivo evidence for assigning WD to the group of secondary Parkinsonian syndromes. Further studies are now needed to address the issue of whether these findings have the potential to modify the therapeutic decision making in treating this copper deposition disorder.
Acknowledgments
The authors are grateful to Ingrid Kämpfer, Christoph Krummeich and Dietlind Sorger for preparing [123I]β-CIT and [123I]IBZM, to Hans-Jürgen Kühn for performing the [64Cu] test, and to Mike Reuter for his support in the medical care of the patients. We also thank Phillip T. Meyer and Bernhard Sattler for performing the phantom SPECT studies.
Footnotes
Presented in parts at the Joint Meeting of the German, Swiss, and Austrian Societies of Nuclear Medicine, Munich, Germany, April 2000.
References
- Received May 29, 2002.
- Accepted after revision August 15, 2002.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}