
Abstract
Summary: We report a case of glaucoma that resulted as a complication of superselective ophthalmic angiography in a 67-year-old man with a recurrent olfactory groove meningioma. Superselective angiography in the right ophthalmic artery was performed to confirm the orifice of the feeding arteries during preoperative embolization. Immediately after the fourth injection of contrast medium, the patient suffered from acute angle-closure glaucoma with elevation of intraocular pressure. Early treatment, including laser iridotomy, relieved the symptoms completely.
Recent advances in microcatheter technology have facilitated superselective ophthalmic angiography for diagnosis and treatment (1–4). We report a case of glaucoma induced by superselective ophthalmic angiography that improved markedly with early treatment. As far as we are aware, this is the first report of glaucoma as a complication of the ophthalmic angiography.
Case Report
A 67-year-old male patient presented with progressive mental disturbance caused by enlargement of an olfactory groove meningioma, which had been partially removed 5 years earlier. Because of heavy bleeding during the first surgery, the plan was to perform embolization preoperatively. The patient had no medical history of glaucoma, and ophthalmologic examination, including measurement of intraocular pressure performed the day before embolization, revealed no ophthalmologic abnormalities. Angiograms revealed that the tumor was fed by the right ethmoidal and middle meningeal arteries. First, the right middle meningeal artery was embolized by using polyvinyl alcohol particles. Next, superselective angiography of the right ophthalmic artery was performed by injecting 0.3 mL ioxaglic acid (320 mg I/mL), diluted to a 50% concentration with saline, through a microcatheter (Tracker-18, Target Therapeutics, Inc., Los Angeles, CA) (Fig 1). To confirm the orifice of the posterior ethmoidal artery, angiography was performed several times at different positions in the ophthalmic artery. Immediately after the fourth injection of contrast medium, the patient complained of severe pain in the right eye and right visual loss with corneal edema and conjunctiva hyperemia. The procedure was discontinued. CT showed remarkable enhancement in the margin of the right eyeball by contrast medium administration (Fig 2). The ophthalmologist (Y.M.) made the diagnosis of right acute angle-closure glaucoma with elevation of intraocular pressure (48 mm Hg). Treatment with glycerol and pilocarpine had no effect on the increased intraocular pressure. Laser iridotomy performed 12 hours after the onset of the symptoms promptly relieved the eye pain and reduced intraocular pressure (20 mm Hg). Vision in the patient’s right eye completely returned 8 days after the procedure, with normalization of intraocular pressure (10 mm Hg). The meningioma was entirely removed surgically 1 month after the embolization. His mental state improved after the surgery, and he was able to return to work.

Right ophthalmic angiogram (lateral projection). The anterior ethmoidal (arrow) and posterior ethmoidal arteries (arrowhead) faintly feed the tumor in the olfactory groove.
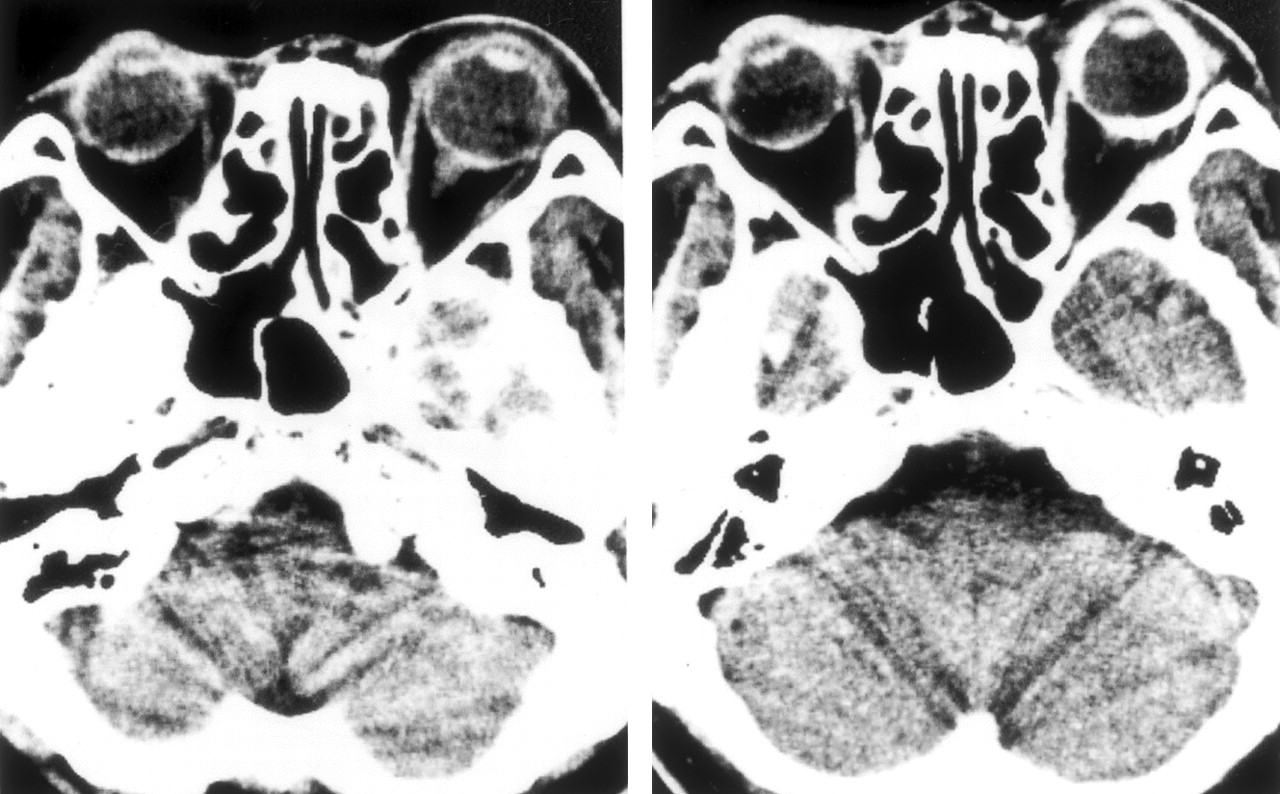
Axial CT scan obtained before (left) and after (right) ophthalmic angiography. The margin of the right eye is markedly enhanced by contrast medium after angiography.
Discussion
Recent advances in microcatheter technology have made catheterization of the ophthalmic artery and its branches possible. Neurointerventional techniques have been used for both embolization of hypervascular lesion fed by the ophthalmic artery (1, 2) and fibrinolytic therapy of central retinal artery thrombosis (3, 4). The efficacy of preoperative embolization of the posterior ethmoidal artery via the ophthalmic artery has been reported for hypervascular meningioma in the olfactory groove (1, 2). Ischemic retinal complications may be caused by migration of embolization materials into the central retinal artery in this procedure (5). Li et al reported a case of ocular complication associated with injection of meglumine sodium diatrizoate into the ophthalmic artery (6). One hour after injection, the patient complained of orbital pain with swelling of the eye and loss of vision, although the case report did not refer to intraocular pressure. Although this case might be similar to that of our patient, to our knowledge there has been no report of glaucoma as a complication of superselective ophthalmic angiography.
Superselective ophthalmic angiography was thought to induce glaucoma in this case, because ophthalmologic examination the day before the procedure revealed no abnormality and the symptoms occurred in the right eye immediately after superselective angiography in the right ophthalmic artery. The ocular complication appears to be related to the radiographic contrast material, which has direct chemotoxicity as well as high osmolality (584 mOsm/kg H2O) (6). Intraarterial delivery of hyperosmotic agents can lead to disruption of the blood-ocular barriers, consisting of the blood-aqueous barrier and the blood-retinal barrier. The blood-aqueous barrier is formed by an epithelial barrier located in the nonpigmental layer of the ciliary epithelium and in the posterior iridal epithelium. In primates, disruption of the blood-aqueous barriers by Conray-60 produced alterations in the cell morphology and extravasation of Evans blue dye from the vascular space into anterior chamber (7). The pathophysiology of the glaucoma in our case seemed to be osmotic disruption of blood-aqueous barrier by repeated injection of ionic contrast medium into the ophthalmic artery. Pulmonary edema has been shown to depend on dose and rate of contrast medium (8). In cases of superselective ophthalmic angiography, a minimal amount of contrast medium may be recommended to prevent this complication. In rat models, nonionic contrast medium causes fewer, and more transient pulmonary edemas than ionic contrast medium (9). Ionic contrast medium (ioxaglic acid) was used in this case because of its advantage to prevent embolisms; however, nonionic contrast medium might be better for superselective ophthalmic angiography. Early ophthalmologic treatment avoided permanent visual complication. The glaucoma induced by ophthalmic angiography may cause profound, permanent loss of vision. As superselective ophthalmic angiography becomes popular in the future, ionic contrast material should be avoided for ophthalmic artery injections.
Conclusion
We have presented a case of acute closure-angle glaucoma as a complication of superselective ophthalmic angiography. Marked improvement was achieved by ophthalmologic treatment, including laser iridotomy. Ionic contrast medium should be avoided for ophthalmic angiography.
References
- Received February 16, 2003.
- Accepted after revision March 6, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.