
Abstract
Summary: A recently developed neck-bridging device (TriSpan; Target Therapeutics/Boston Scientific, Fremont, CA) was used to prevent coil migration into the internal carotid artery during transvenous occlusion of a high-flow, large-tear carotid cavernous fistula.
Management of carotid cavernous fistulas (CCFs) depends on their physiopathology (1–5). Type A CCFs are fast flowing and result from trauma or rupture (or both) of an aneurysm of the intracavernous segment of the internal carotid artery (ICA). They are characterized by a large tear between the ICA and the cavernous sinus (CS), whereas types B, C, and D CCFs are genuine, normally slow flowing, dural arteriovenous malformations. Arteriovenous shunt surgery occurs within the dura mater of the CS. Type B involves small branches of the ICA, and type C is supplied by branches of the external carotid artery (ECA), whereas type D involves branches of both the ICA and the ECA (1).
We describe the treatment of a spontaneous, large-hole, high-flow CCF resulting from rupture of an aneurysm between the pre- and parasellar intracavernous segments of the left ICA. In this case, treatment consisted of transvenous coil embolization of the CS with simultaneous protection of the large tear by a transarterially introduced Trispan coil.
Case Report
An 82-year-old man claimed a sudden onset of a disturbing intracranial bruit and ocular pain with exophthalmus of the left eye. Within the next several days, he developed complete left-side ophthalmoplegia and ocular symptoms of the contralateral eye.
Physical examination revealed proptosis of the left eye with scleral injection, chemosis, and ptosis deficit of cranial nerves III, IV, VI, and VI. Cerebral bruits could be heard over the entire skull, with a maximum over the left periorbital area.
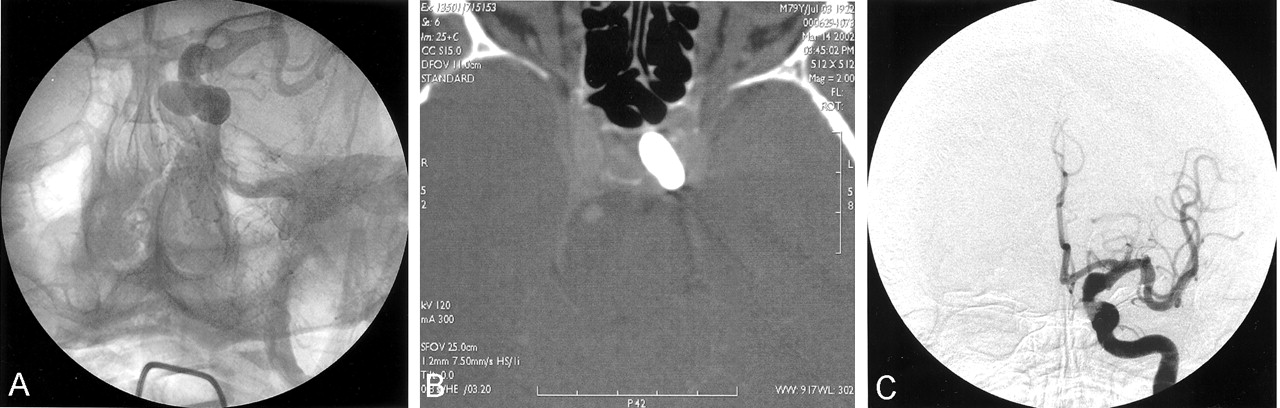
MR imaging and MR angiography of the brain confirmed a high-flow CCF with bilateral dilatation of the CS. A multisection, helical contrast-enhanced CT scan directly demonstrated a large tear between the fusiform, aneurysmatically dilatated pre- and parasellar segments of the left ICA and the CS with a large plexus intercavernosus (Fig 1).

Coronal reconstruction of a contrast-enhanced CT scan showing the large tear between the aneurysmatic fusiform dilatation of the ICA and the cavernous sinus.
Digital subtraction angiography (DSA) confirmed the left-side high-flow CCF with only faint opacification of the ICA distal to the fistula due to the almost complete blood steal from ICA to the CS (Fig 2A and B) with immediate, massive filling of the CS and early drainage through the superior ophthalmic vein into the angular vein, through the intercavernous sinus to the contralateral CS, to the pterygoid plexus bilaterally and the left-side superior petrosal sinus and retrograde flow through the sphenopariatel sinus and insular veins at the left side.

Biplane digital subtraction angiography of the left ICA showing the high-flow CCF with drainage into the inferior petrosal sinus, the ophthalmic vein, and the contralateral side in anteroposterior (A) and lateral view (B).
In view of the age of the patient, who also suffered from coronary artery disease and hypertension, it was our goal to preserve the left ICA, so balloon occlusion of the fistula by arterial approach was attempted first. Because of the size of the tear, stabilization of a detachable balloon inside the CS was not possible; however, we ultimately closed the fistula by placing an Apollo detachable silicon balloon (volume, 0.9 mL; diameter, 8 × 22 mm; detachment strength, medium) from the medial border of the CS to the lateral wall of the aneurysm with preservation of an open ICA lumen in front of the balloon. The position of the balloon and parent ICA were confirmed by native and contrast-enhanced CT the following day (Fig 3).
Unsubtracted view of the left ICA showing the position of the balloon extending from the medial wall of the cavernous sinus to the lateral and dorsal wall of the aneurysm (A) confirmed by CT scan 1 day later (C), whereas the subtracted anteroposterior view confirms preservation of the parent artery and occlusion of the fistula (B).
The initial result was clinically good, with normalization of the proptosis, scleral injection, and chemosis and improvement of eye movements. Five days after this endovascular treatment, however, the patient reported recurrence of the pulsatile tinnitus consisting of a worsening of symptoms. CT and DSA confirmed spontaneous deflation of the balloon with complete reopening of the fistula.
Guided by the biplane road map, obtained from the 6F guiding catheter placed in the left ICA, the CS could be reached through the left superior petrosal sinus, although placement of even large Guglielmi detachable coils (GDCs) resulted in immediate extension and displacement through the large tear from the CS compartment into the ICA (GDC-18; 3D detachable coil).
Another double-tip microcatheter (FasTracker 18, Target Therapeutics) was inserted into the cavernous sinus via the 6F guiding catheter placed in the ICA. The large hole between the ICA and the CS could be crossed without any problem, and the bridging device (Trispan, 14 mm/7 mm) was deployed inside the CS.
Once the tear-bridging device was deployed inside the CS, the microcatheter was gently pulled back to ensure a stable position, until the Trispan loops were fixed at the dural wall of the CS and the stem of the coil was in a stable position at the center of the tear, comparable to placement of the Trispan coil in a wide-necked aneurysm (2, 3, 4). After we confirmed the stable position of the Trispan coil, the CS was packed through the transvenously introduced microcatheter (Excelsior; Target Therapeutics), starting at the origin of the superior ophthalmic vein with the result of dense packing of the CS compartment adjacent to the tear but without any tendency of coil protrusion through the Trispan-protected hole into the ICA (Fig 4). After confirmation of the occlusion of the fistula, the tear-bridging Trispan coil was also electronically detached from the pusher wire.

Nonsubtracted oblique view (A) showing the transarterially introduced microcatheter with the neck-bridging device between the CS and ICA (heavy arrows) and the transvenously introduced microcatheter during packing of the CS (thin arrows). Corresponding digital subtraction angiography confirms the protected ICA and dense packing of the CS compartment directly adjacent to the ICA-CS tear with occlusion of the fistula (B).
The patient’s condition further improved during the weeks that followed, and angiography 6 months later confirmed occlusion of the CCF without development of a venous pouch at the site of the ICA-CS tear.
Discussion
The TriSpan coil is a new device that was designed to treat wide-necked aneurysms. Once this device is placed from inside at the neck of the aneurysm, it protects the parent artery from coil protrusion during the entire process of packing the aneurysm with GDCs.
In our 82-year-old patient, a CCF developed because of the spontaneous rupture of an aneurysm arising from the pre- and parasellar intracavernous segments of the ICA. Contrast-enhanced CT, MR imaging, and DSA revealed a large tear that may have been further increased by the first therapeutic procedure: by using the normal transarterial approach, the balloon could be navigated into the CS; however, because the large tear the balloon extended from the CS through the tear into the fundus of the aneurysm, a widening of the tear may have been the result of insufflation and detachment of the balloon, which was stable for only 1 week.
Stable positioning of normal and 3D electrolytically detachable coils inside the lumen of the CS was impossible. Dealing with the situation of a high-flow CCF with venous drainage into the superior ophthalmic vein, as well as retrograde flow into the sphenoparietal sinus and insular veins, we had to take care not to occlude one of these venous outlets of the CS, which may redirect the drainage into the other exit and suddenly increase the symptoms of venous congestion in this region. The goal of the transvenous procedure was to reach and selectively occlude the compartment of the CS that was in direct contact with the fistula. Stable position of any coil, however, was impossible because of the small size of this venous compartment compared with the large hole of the CCF, which is an anatomic situation comparable to that in wide-necked aneurysms.
The use of the tear-bridging device permitted selective and stable coil packing of this compartment of the CCF directly adjacent to the large tear (Fig 5), which may be the reason that complete occlusion could be obtained during one session and no venous pouch or pseudoaneurysm developed either primarily or at the control angiography 6 months later.

Drawing of the neck-bridging TriSpan coil showing the three nitinol loops, partly covered by platinum to increase radiopacity, fixed together at their struts and the detachment zone at the end of the pusher wire.
- Received March 30, 2003.
- Accepted after revision August 8, 2003.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.