
Abstract
Summary: We compared two methods of 3D digital subtraction angiography (DSA)—propeller and standard rotation—for the assessment of aneurysmal morphology and its relation to neighboring vessels. Aneurysms were correctly visualized and localized with both techniques. 3D DSA with propeller rotation technique seems to be effective and allows us to reduce the amount of contrast material related to a shortened acquisition time. Technical progress including propeller rotation allows a larger range of rotation and faster rotational speeds.
3D reconstruction of intracranial vessels is of particular interest for the evaluation of intracranial aneurysms. This technique allows us to assess the aneurismal neck, including its shape, size, and relationships with neighboring vessels. It can include views that are impossible to obtain by using only conventional angiographic projections (1–7). These features are important to consider when one decides on surgical or endovascular treatment (2, 8).
Standard 3D digital subtraction angiography (DSA) usually uses a roll rotational angiography mode over a 180°–200° angle, with a maximal rotation speed between 20 ° and 30° per second. The C-arm is placed perpendicular to the head axis. 3D DSA with the propeller technique has been developed to decrease the acquisition time without altering image quality. The C-arm remains in the same position as it does during conventional angiography. Images are acquired over an angle of 240° with a maximal rotation speed of 55° per second. This new position also decreases the total amount of contrast material inject. The whole acquisition involves an average of 100 images per run, with theoretically similar image quality of standard rotation.
The aim of this study was to perform 3D DSA with both acquisition techniques—roll and propeller rotation—in consecutive patients with a ruptured intracranial aneurysm. We sought to compare image quality and anatomic information obtained with both techniques.
Technical Description
Subjects
The study group included consecutive patients admitted to the emergency department of Lille University Hospital, France, between November 2002 and March 2003 because of a subarachnoid hemorrhage. They included 31 women and 23 men with a mean age of 47 years (range, 14–91 years). Subarachnoid hemorrhage was confirmed by means of emergency cranial CT. All patients underwent conventional 2D DSA of both the carotid and the vertebral arteries the day after their admission. After diagnostic angiography, discussion between the neurosurgical and neurointerventional teams led to the decision to perform aneurysm exclusion by means of an endovascular approach within 24 hours in all patients.
2D DSA was performed with anteroposterior, lateral, and working views. An angiogram was acquired at a rate of two images per second with a 512 × 512 matrix size and a 20-cm field of view. 3D rotational angiography was then preformed by using the C-arm (Allura V 5000; Philips Medical Systems, Best, the Netherlands) and the standard rotation or the propeller rotation technique.
Endovascular treatment was performed 24 hours later and included the 3D DSA technique not used for the initial diagnostic angiography. This angiographic control performed just before the treatment was planned to check for the absence of morphologic change.
Standard 3D DSA
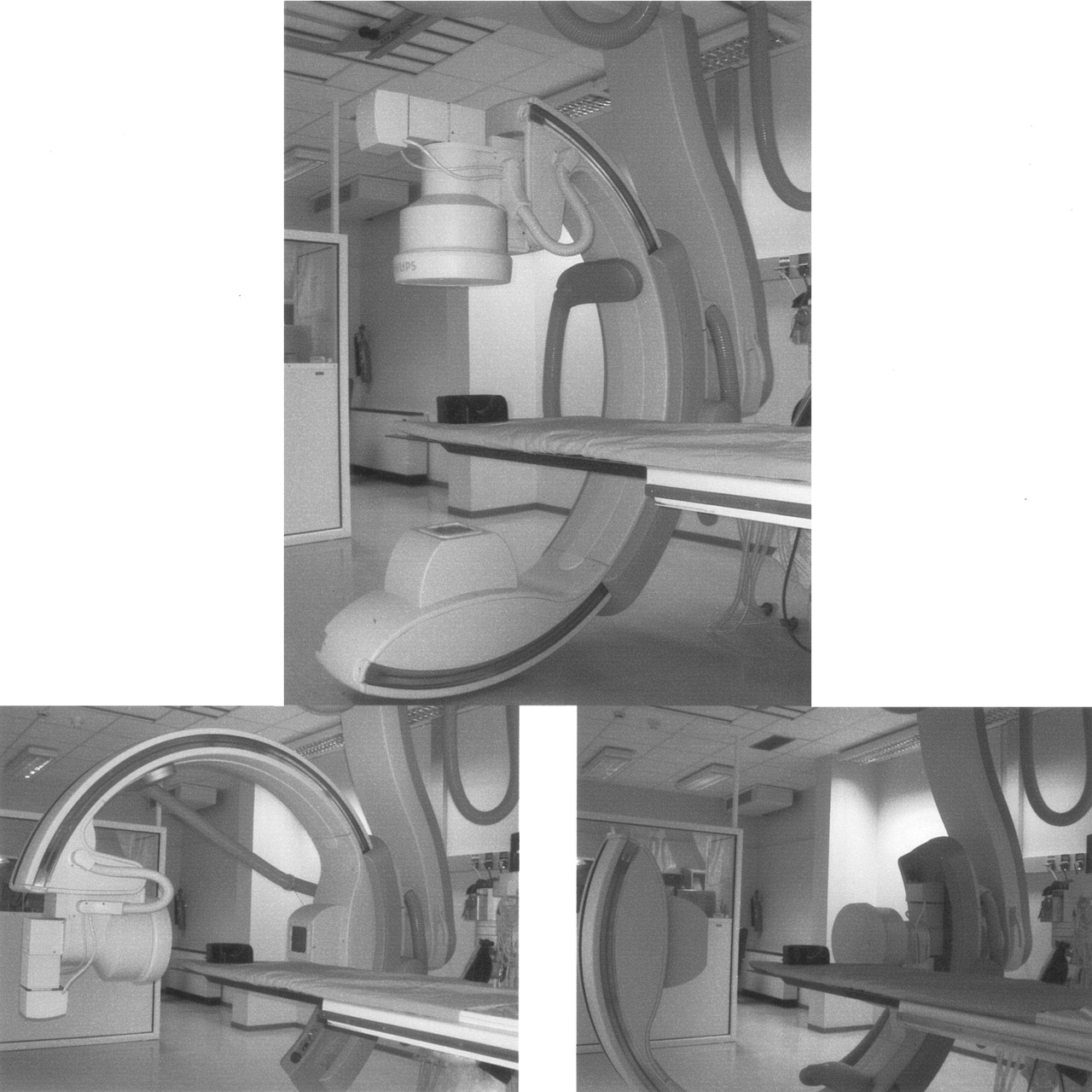
For the standard 3D DSA technique, the range of rotational angiography extended over 180° (left oblique 90° and right oblique 90) (Fig 1) at a maximum rotational speed of 30° per second within 7 seconds. Nonionic contrast medium (Iodixanol, Visipaque 320; Amersham Health, Cork, Ireland) with an average flow rate of 4 mL/s was injected into the internal carotid artery or the vertebral artery. Contrast material was injected into the vertebral artery and the internal carotid artery (16 and 28 mL, respectively) according to the location of the aneurysm.

Standard roll rotational angiography mode. C-arm is placed perpendicular to the head axis (top). Range of rotational angiography extends over 180° (right oblique 90°, left image, and left oblique 90°, right image).
Propeller Rotation 3D DSA
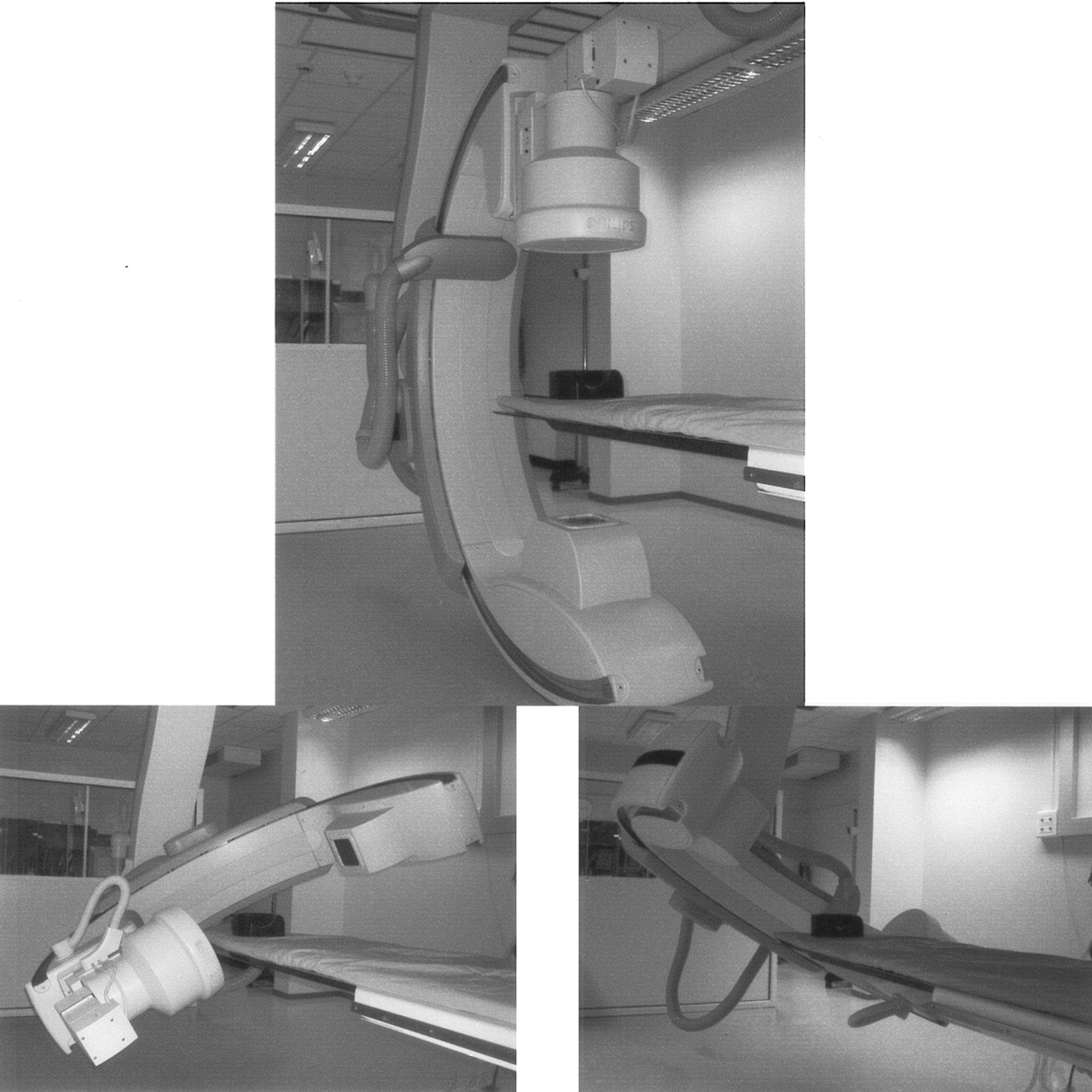
For the 3D DSA technique with the propeller rotation, the range of rotational angiography extended over 240°(left oblique 120° and right oblique 120) (Fig 2) at a maximum rotational speed of 55° per second within 4 seconds. An injection of the same nonionic contrast material with an average flow-rate of 4 mL/s was performed. The injected volume of contrast material was 9 and 16 mL for the vertebral and internal carotid arteries, respectively.

Propeller rotational angiography mode. C-arm remains in the same position as with conventional angiography (top). Range of rotational angiography extends over 240° (right oblique 120°, left image, and left oblique 120°, right image).
Methods
The rotational imaging was performed with a motorized C-arm around the anatomy of interest, during which 100 unsubtracted images were taken. The mask and contrast runs were performed with the C-arm in the same angle position. 3D rotational angiographic data were transferred to an independent workstation (Integris; Philips Medical Systems) for reconstructions including the volume-rendered technique. Intracranial 3D angiograms were then generated by one of two senior neuroradiologists (B.L., J.Y.G.). The threshold was manually adjusted by using a visual control to remove the surrounding bone structures and to optimize vessel conspicuity. The same reconstructions and same views were obtained with both procedures. The irradiation rate and time reconstructions were the same for both techniques as the number of images. The two senior neuroradiologists reviewed the 3D DSA image reconstructions to analyze image quality, visualization and location of aneurysm, and possible incorporation of vessels into the aneurysm or neck. Because the size of ruptured aneurysms might have changed between examinations (diagnostic and therapeutic angiographic studies), this parameter was not assessed.
Image contrast was graded low when the contrast in the enhanced arterial lumen was only slightly higher than the contrast in the background, moderate when the signal intensity was clearly higher, and high when the signal intensity was optimal. Image interpretation was performed only on 3D reconstructions, and visualization of surrounding vessels was classified as poor, ambiguous, or accurate. Cases that led to a disagreement between observers were reviewed by both readers to reach a consensus. For each examination, a score was calculated. Standard 3D DSA was considered the reference.
Statistical analysis consisted of a comparison of the κ statistics for the scores for each examination performed with the two 3D DSA techniques. κ values higher than 0.6 suggested substantial agreement, and values higher than 0.8 indicated excellent agreement. P values lower than .05 indicated a significant difference.
Results
The protocol was performed in 23 patients (eight men, 15 women; mean age, 51 years [range 30–70 years]) with 24 aneurysms: 23 in the anterior circulation and one in the posterior circulation.
The imaging protocol was performed in all patients, with an high overall image quality. Aneurysms were correctly visualized and localized with both techniques in all cases. In 10 cases, vessel incorporation into the neck was detected with accuracy by using the propeller rotation technique; in nine cases, it was detected with the roll rotation technique. In one patient, a discrepancy was observed between the examinations, because visualization of vessel incorporation was judged poor with standard 3D DSA and accurate with the propeller rotation technique.
Discussion
The therapeutic strategy for intracranial ruptured aneurysms requires high-spatial-resolution imaging to evaluate the morphology of the aneurysm and also the vascular structures adjoining the cerebral aneurysm. 3D-reconstructed DSA has been developed to provide accurate anatomic information, allowing us to decide on the most appropriate treatment between surgical and endovascular techniques. This approach enables us to select the optimal angle of view and to choose the first coil. Previous studies have shown the usefulness of this method in demonstrating intracranial aneurysms (1, 2), in assessing coil positioning during endovascular treatment (5), and in evaluating the degree of aneurysm occlusion.
However, limitations of 3D DSA should be pointed out. First, several acquisitions are often performed during the same procedure, and this requires additional injections of contrast material. Second, additional time is needed with the standard rotation technique because the C-arm must be positioned perpendicular to the table axis, whereas conventional angiography is performed with the C-arm in the same axis as the examination table. By using the propeller rotation technique, high-quality 3D images of the cerebral arteries are acquired during a shorter acquisition time (4–7 seconds) with less contrast medium (40% less) that that used with the standard technique. Furthermore, it is not necessary to shift the C-arm because propeller rotation may be performed with the C-arm in the same position as that used for conventional angiography. This technical point sharply decreases the examination time. These improvements are achieved with the same image quality and diagnostic value as that of the standard rotation technique.
Conclusion
Recent technologic advances in 3D DSA—including the propeller rotation technique—seems interesting for the diagnosis of ruptured cerebral aneurysms. Compared with the standard rotation technique, this method is faster, it is easier to perform, and it requires less contrast material. Moreover, the image quality is not altered.
- Received April 24, 2004.
- Accepted after revision July 11, 2004.
- Copyright © American Society of Neuroradiology




{kind=link}
{kind=link}