
Abstract
BACKGROUND AND PURPOSE: Spinal epidural abscesses are major complications of epidural anesthesia, and their MR features have been reported. In patients receiving continuous infusion via an epidural catheter, MR findings may mimic those of spinal epidural abscess in the absence of infection. The purpose of this study was to assess the spinal MR findings associated with continuous epidural anesthesia.
METHODS: Spinal MR findings in five consecutive patients receiving continuous epidural anesthesia were retrospectively evaluated. Axial and sagittal T1- and T2-weighted spin-echo and contrast-enhanced fat-suppressed T1-weighted spin-echo images were obtained. Infection was ruled out on microbiologic analysis three patients and on follow-up in two. Each lesion was evaluated for its MR signal intensity, location, extent, delineation, and enhancement pattern. In three patients, follow-up MR imaging was performed within 5–150 days, and the images were compared.
RESULTS: Posterior epidural lesions were identified in all five patients. The lesions were isointense to hypointense relative to the spinal cord on T1-weighted images, isointense relative to CSF on T2-weighted images, and well enhanced on enhanced T1-weighted images. The anomalous enhancement involved two to seven vertebral bodies. In one patient, the enhanced lesion slightly compressed the spinal cord. On follow-up MR imaging, the epidural lesions decreased in two patients and did not change in one.
CONCLUSION: Continuous epidural anesthesia can result in MR findings similar to those of epidural abscess, even in the absence of infection.
Spinal epidural abscesses (SEAs) are major complications of epidural catheter placement (1–7). Although SEAs after the administration of epidural anesthesia are rare, the increased use of temporary catheters and long-term epidural anesthesia has led to an increased incidence of epidural infection (8–13). Spinal cord compression due to sterile masses has been reported in patients receiving long-term spinal infusions of high-dose morphine (14–16). However, to our knowledge, no reports of systematic MR imaging studies of these spinal lesions have been published. The purpose of this study was to assess spinal MR images in five consecutive patients without infection who received continuous epidural anesthesia.
Methods
Spinal MR images from five consecutive patients (one man, four women; age range 26–70 years; mean age, 54.2 years) who underwent epidural anesthesia in our institution between March 2001 and November 2003 were retrospectively evaluated (Table 1). The underlying conditions for the pain control were postherpetic neuralgia in two patients, and postoperative pain, compression fracture of vertebral bodies, and whiplash injury in one patient each. In all patients, epidural catheters were introduced in the operating room under aseptic conditions. The polyamide catheters were inserted through a Tuohy needle by using the loss-of-resistance technique. They were fixed with adhesive dressings after attachment to an epidural bacterial filter. Bupivacaine 50–120 mg/day was continuously infused for 7–25 days by using a syringe pump.
Clinical features of patients receiving epidural analgesia
Table 1 shows the indications for MR imaging. We examined patient 5 to investigate the spinal MR finding after the patient provided informed consent. All patients underwent initial MR imaging within 7 days of the removal the epidural catheter. We used a 1.5-T superconductive MR imaging system (Gyroscan, ACS-NT; Philips Medical Systems, Amsterdam, The Netherlands) and a quadrature synergy spinal coil. In all patients, sagittal T1-weighted spin-echo (SE), axial T2-weighted fast SE, sagittal fat-suppressed T2-weighted fast SE, and axial and sagittal contrast-enhanced fat-suppressed T1-weighted SE images were obtained. T1-weighted SE images were acquired with the following parameters: TR/TE/NEX = 450/13/1, section thickness = 5 mm, and intersection gap = 0.5 mm. For T2-weighted FSE image acquisition, the parameters were TR/TEeff/NEX = 2500/120/1, section thickness = 5 mm, and intersection gap = 0.5 mm. For all sequences, the FOV was 20–30 cm, and the matrix was 192–256 × 256–512.
In three patients with catheter dysfunction or fever (patients 1–3), the catheter tip was sent for Gram staining and aerobic and anaerobic bacterial cultures. The laboratory results ruled out infection. The other two patients had no inflammatory changes during clinical follow-up. None had neurologic deficits in the course of epidural anesthesia or follow-up.
Two radiologists (I.I., N.M.) performed qualitative visual inspection of the spinal MR images. By consensus, we recorded the signal intensity, location, extent, delineation, and enhancement pattern of the spinal lesions. Patients 1–3 underwent follow-up MR imaging study within 5–150 days of their first examination; in these patients, the initial and subsequent images were assessed for changes.
Results
Table 2 summarizes the initial MR features of the five patients. In all five, the lesions were located in the posterior epidural space at the site of catheter insertion. All lesions were hypointense relative to the spinal cord on T1-weighted images and isointense to CSF on T2-weighted images (Figs 1 and 2). In patient 3, the lesion had hypointense areas on T2-weighted images (Fig 1). On fat-suppressed contrast-enhanced T1-weighted images, enhancement of the lesions was homogenous in three patients, relatively homogenous in one, and inhomogeneous in one. The enhanced lesions were clearly delineated from the adjacent subdural space, spinal cord, and posterior fat tissue. The lesions extended along the spine and involved two to eight vertebral bodies (mean, 4.8 vertebral bodies). In patient 2, the enhanced lesion slightly compressed the spinal cord (Fig 2).

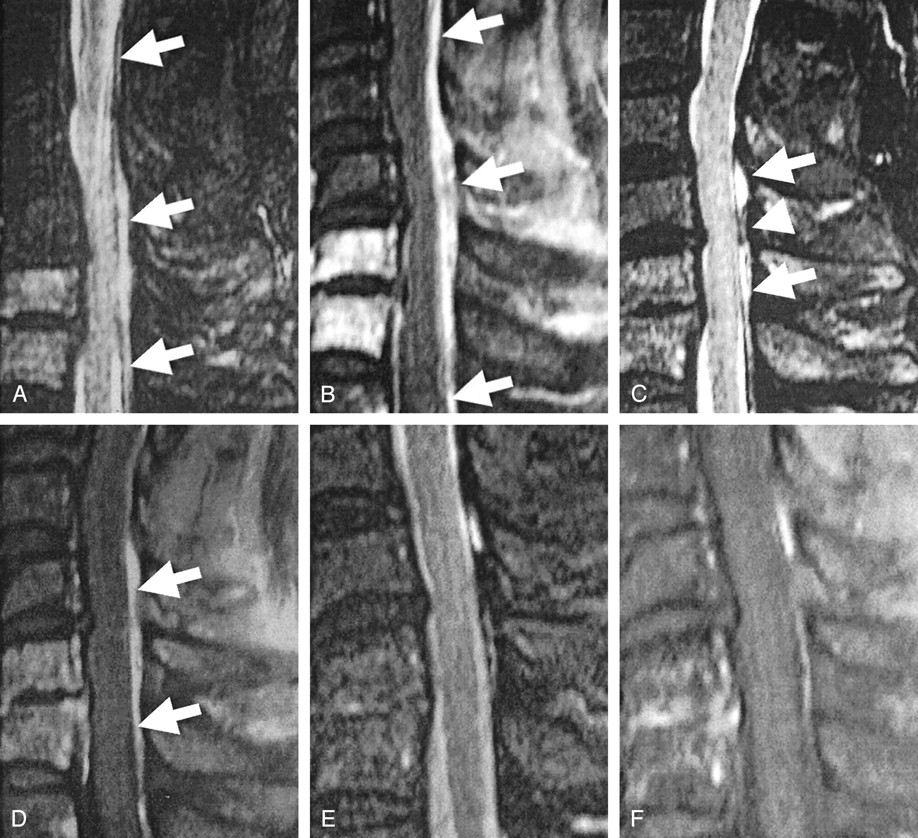
Case 3. A 57-year-old woman who received epidural anesthesia and underwent MR imaging at 3 days (A–D) and 6 weeks (E and F) after the epidural catheter was removed.
A, Fat-suppressed T2-weighted fast SE image shows a lesion in the posterior epidural space from T12 to L1 (arrow) that is isointense relative to CSF. Lesion has some hypointense areas (arrowheads).
B, On T1-weighted SE images, the lesion (arrow) is relatively hyperintense relative to CSF.
C and D, On sagittal (C) and axial (D) fat-suppressed enhanced T1-weighted images, the lesion (arrow) is homogeneously enhancing.
E and F, T2-weighted fast SE (E) and enhanced T1-weighted (F) images do not show the epidural lesion.
Case 2. A 66-year-old man who received epidural anesthesia and underwent MR imaging 2 days (A and B), 2 months (C and D), and 5 months (E and F) after the epidural catheter was removed.
A, On this fat-suppressed T2-weighted fast SE image, lesion in the posterior epidural space from C3 to T1 (arrows) is isointense relative to CSF. Fresh compression fracture of the C6 and C7 vertebral bodies is hyperintense.
B, On this sagittal fat-suppressed enhanced T1-weighted image, lesion in the posterior epidural space from C1 to T1 (arrows) is inhomogeneously enhancing.
C, Although the signal intensity of the lesion has not changed on this fat-suppressed T2-weighted fast SE image, its extent is reduced, now extending from C5 to T1 (arrows). Epidural lesion has a hypointense area (arrowhead).
D, On this fat-suppressed enhanced T1-weighted image, lesion (arrows) has decreased in size and is enhanced homogeneously.
E and F, Fat-suppressed T2-weighted fast SE (E) and fat-suppressed enhanced T1-weighted (F) images do not clearly depict the lesion.
Summary of initial MR imaging findings
In patient 2, 2-month follow-up T2-weighted images showed a hypointense area in the lesion of the posterior epidural space (Fig 2). In patients 2 and 3, follow-up images obtained at 5 months and 6 weeks, respectively, showed that the lesions in the posterior epidural space almost disappeared (Figs 1 and 2). In patient 1, follow-up images obtained 6 days after removal of the catheter showed no change.
Discussion
Sterile masses can lead to spinal cord compression after long-term spinal infusion of high doses of morphine (14–16). Proposed causes of the spinal lesion are damage to neural tissues, which predisposes the patient to analgesic toxicity; configuration of the catheter tip; characteristics of the infused drug; hypersensitivity reactions; previous or simultaneous exposure to other intraspinal devices, such as spinal cord stimulators; and regional CSF flow dynamics. The pathology of catheter-related masses might be necrotic and connective tissue, inflammatory cells, arachnoid fibrosis, and meningothelial hyperplasia.
Coffey and Burchiel (17) evaluated 41 patients and found that 39 (95%) with catheter-associated masses were receiving morphine sulfate and hydromorphone or various combinations of local anesthetics and other substances. They noted that 24 months was the median duration of therapy at the time the mass was detected, and they suggested that the dose of morphine was a potential cause. McMillan et al (18) reported that three of seven patients receiving intrathecal analgesic therapy for 118 months had catheter-associated masses. Patients with spinal lesions received larger doses of morphine and were younger than those without such lesions. Although their catheter-associated lesions were probably sterile granulomas due to the continuous injection of analgesic material, as in our patients, some differences are observed. For instance, our patients received a low-to-medium dose of bupivacaine, which is a local, long-lasting anesthetic with relatively low toxicity and a slower onset of effect. The patients’ spinal lesions were linear or band-shaped with an average length of 4.8 vertebral bodies. In comparison, the previously reported masses were round and localized at the catheter tip.
Another major difference between their results and ours involved signal intensity. Although granulomas are usually not as hyperintense as CSF on T2-weighted images, all of our patients’ lesions had CSF-equivalent signal intensity on T2-weighted images, as well as remarkable enhancement. Our lesion were thought to be highly vascularized granulation tissues with increased water content, which are composed of newly formed capillaries and inflammatory cells. Continuous injection into epidural space is believed to cause mechanical and chemical injury to the posterior epidural fat tissue and precedes the healing reaction. The collagen and/or fibrous component of granulation tissue may increase with time and decrease the signal intensity on T2-weighted images. In patients 2 and 3, initial or follow-up T2-weighted images showed hypointense areas in the lesions. The hypointense areas may represent the collagen and/or fibrous tissues of granulomas, which appear in the healing process. We propose that continuous epidural anesthesia induces such a reaction, in varying degrees. Further study is needed to clarify the mechanisms underlying the formation of the granulomas in the posterior epidural space in patients receiving opioid or nonopioid analgesics.
The incidence of catheter-related SEA is 0.04–0.05% (19, 20). The rarity and nonspecific clinical features make the initial diagnosis of SEA difficult. MR imaging, especially contrast-enhanced MR imaging, is useful for the diagnosis of SEA (8–13). SEA can be divided into the acute, subacute, and chronic phase (10, 19). Symptoms of acute SEA may appear within hours to days. In the acute phase, pus is found in the epidural space with no enhancement on contrast-enhanced MR imaging. In the subacute phase, granulation tissue surrounding the pus results in rim enhancement. Patients with chronic SEA often present with the signs and symptoms seen in patients with acute SEA, though they have a more prolonged course. In the chronic phase, granulation tissue is visualized as homogeneous, linear or bandlike enhancement on contrast-enhanced MR imaging. Compared with sporadic SEA, catheter-related SEAs do not have a specific pattern of MR imaging findings with respect to signal intensity or enhancement (1, 2). Almost all cases of catheter-related SEA were located in the posterior epidural space where the tip of the catheter was inserted. The location, shape, and enhancement pattern of our patients were similar to those of patients with chronic catheter-related SEA. However, chronic SEA is hypointense relative to CSF on T2-weighted images. The MR findings of noninfected lesions may improve over time. These MR findings may be useful for differentiating SEA from noninfected lesions.
Our study had some limitations. First, two patients did not undergo microbiologic tests to rule out infection, however, their clinical course ruled out SEA. Patient 5 had no symptoms indicative of SEA, and patient 4, who had lower back pain due to a compression fracture, had no exacerbation of symptoms in the absence of medication. Second, we did not perform diffusion-weighted imaging. Eastwood et al (21) studied diffusion-weighted images in a patient with SEA and reported findings consistent with those in published reports on brain abscesses. Diffusion-weighted imaging may be helpful for differentiating abscesses from changes after epidural anesthesia. Third, because we did not obtain pathologic specimens of the lesions in the posterior epidural space, we were unable to confirm the disease. The mechanism underlying the development of these masses during the epidural anesthesia is unclear.
Conclusion
Our five consecutive patients who underwent continuous epidural anesthesia infusion had spinal MR findings similar to those of patients with epidural abscesses. However, well-enhanced posterior epidural lesions with CSF-equivalent signal intensity on T2-weighted images may suggest noninfected granulomas with highly vascularized tissues and increased water content. MR findings of the noninfected lesions may improve over time. This information is of value to radiologists attempting to interpret MR findings in patients receiving continuous epidural anesthesia.
References
- Received July 1, 2004.
- Accepted after revision August 31, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.