
Abstract
BACKGROUND AND PURPOSE: Endovascular treatment of intracranial aneurysms is too often associated with aneurysm recurrence due to coil compaction. High packing of coils prevents compaction. To increase the packing attenuation, we sought to evaluate the results of selective embolization of aneurysms with complex-shaped coils alone.
METHODS: Twenty consecutive patients with an intracranial aneurysm were treated by selective embolization. There were 12 women and eight men, with a mean age of 48 years. Fourteen patients presented with subarachnoid hemorrhage, whereas six were asymptomatic. Mean size of aneurysms was 5 mm (range, 3–11 mm). In all cases, we tried to pack the aneurysm with complex coils only (Orbit, Cordis, Miami Lakes, FL), delivered in a concentric fashion. Remodeling technique was used in two cases of wide-neck aneurysms. Clinical and anatomic outcome were assessed by using the modified Glasgow outcome scale and 6-month MR angiography (MRA).
RESULTS: From two to five complex coils were delivered within the aneurysms. Occlusion by using complex coils alone was successful in 16 patients, and resulted in 14 complete occlusions and two neck remnants. In four patients, additional helical Orbit coils or Guglielmi detachable coils were required to complete aneurysm obliteration. No technical complication occurred, and clinical outcome was excellent in 14 cases and good in two. Follow-up MRAs were obtained in all patients and showed only one slight recanalization.
CONCLUSIONS: Intracranial aneurysms may be treated by selective embolization with complex coils only. Imaging follow-up at 6 months shows a low rate of coil compaction.
Endovascular treatment of intracranial aneurysms has made remarkable progress over the past 10 years and has been accepted as an alternative to surgical clipping (1). The principal disadvantage of this less-invasive technique, however, is aneurysm recurrence (2, 3). Several authors (4–6) have shown a positive relationship between the packing attenuation (PD) of coils within the aneurysmal sac and long-term occlusion rate. In an experimental study, Piotin et al (7) showed that optimal packing of small silicone aneurysm model was achieved with three-dimensional (3D) coils used only in a concentric fashion. Furthermore, a recent clinical study (4) showed that a PD of 24% or more was associated with an absence of coil compaction on 6-month angiographic controls in most aneurysms. The authors suggested using 3D and/or thicker coils to treat cerebral aneurysm to reach a sufficient PD. Three-dimensional coils, however, are stiffer (8) than helical coils and may limit the aneurysm packing. This explains that the endovascular procedure of aneurysm coiling usually consists in the delivery of a first 3D coil to create a good basket and then helical coils to fill the residual lumen. To our knowledge, there is no study in the literature assessing the feasibility of endosaccular coiling of cerebral aneurysms with 3D coils alone. Orbit coils (Cordis, Miami Lakes, FL) have recently been introduced and are the first 3D models available in all sizes ranging from 2 to 20 mm. In our study, we prospectively evaluated the immediate and 6 months follow-up results of selective embolization with 3D Orbit coils in 20 consecutive patients with an intracranial aneurysm.
Methods
Population
Between January and February 2004, 20 consecutive patients with intracranial aneurysms were referred to our department for endovascular treatment. As shown in the Table, there were 12 women and eight men, with a mean age of 48 years (range, 31–73 years). Fourteen patients presented with subarachnoid hemorrhage (SAH) and were classified according to the Hunt and Hess (HH) scale (9): 12 patients were grade I or II, and two were grade IV. In six patients, the aneurysm was asymptomatic. Aneurysms were located in the anterior circulation in 17 cases and in the posterior circulation in three. Mean size of aneurysms was 5 mm (range, 3–11 mm) and two had an unfavorable neck size (>4 mm) or neck-to-sac ratio (>0.7). All patients underwent conventional angiography of both carotid arteries and vertebral arteries. Therapeutic alternatives were discussed between neurosurgical and neurointerventional teams.
Endovascular treatment of intracranial aneurysms in 20 patients*
Orbit Coils
The Orbit Coil consists of a shaped 0.012-inch platinum coil attached to a delivery tube. It is designed for use with the detachment syringe that is required to purge the system properly and detach the coil through a hydraulic detachment mechanism. Orbit coils are the evolution of the Trufill detachable coil system and present a reduced system profile to allow for compatibility with 0.014-inch microcatheters.
These coils are available in both 3D (Orbit complex and mini-complex coils according to their size) and helical shapes (Orbit helical coil). The complex coils present a 3D structure that is designed to fill the outer circumference of the aneurysm while leaving the inner space open for subsequent coils (Fig 1). All sizes from 2 to 20 mm are presently available.

The 3D configuration of the complex Orbit coil.
Endovascular Procedure
In all patients, the endovascular treatment was performed under general anesthesia and systemic heparinization. The adequacy of systemic anticoagulation was monitored by frequent measurements of the activated clotting time (ACT). A baseline ACT was obtained before the bolus infusion of heparin (50–75 IU/kg body weight), and hourly thereafter. The bolus infusion of heparin was followed by a continuous drip (1,000–1,500 IU/h), with the purpose of doubling the baseline ACT. In most patients, systemic heparinization was stopped at the end of the procedure. For wide-neck aneurysms or in cases with periprocedural complications, systemic heparinization was prolonged for 48–72 hours. Patients were treated by selective embolization with Orbit coils; we have tried to obtain a 3D packing of the aneurysms by forming a basket with a complex coil that was subsequently filled concentrically with smaller complex coils in an “onion-like” fashion. An Excelsior 10 microcatheter (Target Therapeutics, Fremont, CA) was used to deliver coils within the aneurysm. In two cases with unfavorable neck-to-sac ratio, the remodeling technique (10, 11) was used to avoid coil protrusion into the parent artery. Failure of endovascular treatment was defined as an impossibility to completely occlude an aneurysm with complex Orbit coils alone. In these cases, helical Orbit coils or Guglielmi detachable coils (GDC) were used to achieve aneurysm obliteration. After endovascular treatment, patients were transferred to the intensive care unit, and fluid balance, neurologic status, and blood pressure were carefully monitored.
Immediate Outcome
Patients were evaluated by angiography to document aneurysm obliteration. Angiographic results were classified as complete occlusion (no contrast filling the aneurysmal sac), neck remnant (residual contrast filling the aneurysmal neck), or residual flow (residual contrast filling the aneurysmal body). A senior neurosurgeon (J.-P.L.) recorded the clinical course, including worsening of symptoms and death. Clinical outcome was graded according to a modified Glasgow outcome scale (GOS) (12), as follows: excellent (neurologically intact); good (mild hemiparesis, cranial nerve palsy, or other deficit that does not interfere with daily functioning or work); fair (significant hemiparesis, aphasia, confusion, or other deficit that interferes with daily activities or prevents a return to work); and poor (coma or severe neurologic deficit rendering the patient dependent on family or nursing staff).
Patient Follow-up
Imaging follow-up included MR examination and MR angiography (MRA) at 6 months. We assessed both brain tissue by using axial spin-echo T1-weighted sequence, T2-weighted sequence, fluid-attenuated inversion recovery sequence and the intracranial vessels by using time-of-flight and gadolinium-enhanced angiography. Clinical examination by a senior neurosurgeon (J.-P.L.) was simultaneously obtained with the imaging control. No patient was lost, and follow-up MRAs were compared with immediate postembolization angiograms and then assigned to one of three categories: (1) further thrombosis, when the amount of contrast agent filling the aneurysm decreased; (2) unchanged, when a similar degree of aneurysm occlusion in multiple projections was found; and (3) recanalization, when an increase of the amount of contrast filling in the aneurysm was observed. Conventional angiography, MRA, and MR imaging were reviewed for all patients by two senior neuroradiologists together (B.L., X.L.).
Illustrative Cases
Case 1
A 37-year-old woman (patient 12) presented with a SAH (HH grade I), and conventional angiography (Fig 2A) revealed an anterior communicating artery aneurysm. The patient was treated by selective embolization with Orbit coils alone. Five complex coils were delivered within the aneurysm lumen, including a 9 mm/25 cm coil (Fig 2B), a 7 mm/21 cm coil (Fig 2C), a 5 mm/15 cm coil (Fig 2D), a 3 mm/3 cm coil (Fig 2E), and a 2 mm/2 cm coil. Conventional angiograms (Figs 2F, -G) at the end of the procedure showed a neck remnant. The patient made an excellent recovery and was discharged 12 days after the treatment. MRA at 6 months showed complete occlusion of the aneurysm (Fig 2H).
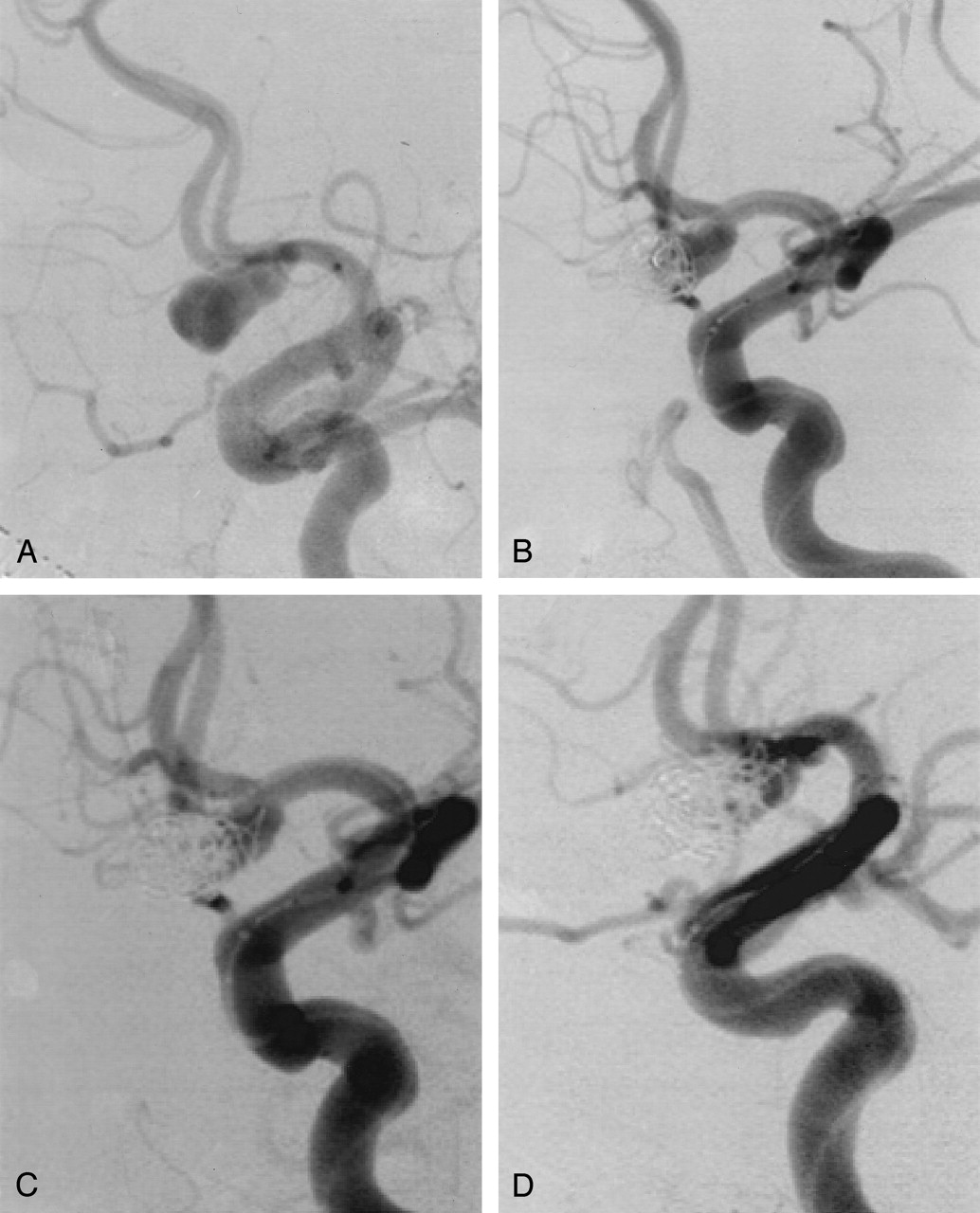

Subarachnoid hemorrhage in a 37-year-old woman.
Left ICA angiogram (A) shows an anterior communicating artery aneurysm with a length of 11 mm and a width that varied from 5 to 7 mm.
Selective embolization with complex Orbit coils only: five coils were delivered within the aneurysm lumen including a 9 mm/25 cm coil (B), a 7 mm/21 cm coil (C), a 5 mm/15 cm coil (D), a 3 mm/3 cm coil. (E), and a 2 mm/2 cm coil.
Conventional nonsubstracted (F) and substracted (G) angiograms at the end of the procedure show a neck remnant.
Follow-up MRA (H) at 6 months shows a complete aneurysm occlusion.
Case 2
A 44-year-old woman (patient 10) presenting with chronic headaches underwent brain imaging. An unruptured internal carotid artery (ICA) aneurysm was discovered, and the patient was referred to our department for embolization. Conventional angiography revealed a left ICA bifurcation aneurysm (Fig 3A). Selective coiling was performed with four complex coils delivered in a concentric fashion, including a 7 mm/21 cm coil (Fig 3B), a 4 mm/7 cm coil (Fig 3C), a 3 mm/4 cm coil (Fig 3D), and a 2 mm/2 cm coil (Fig 3E). Final result consisted of a complete occlusion and the patient was discharged 4 days after the treatment. MRA at 6 months showed a slight recanalization of the neck (Fig 3F).
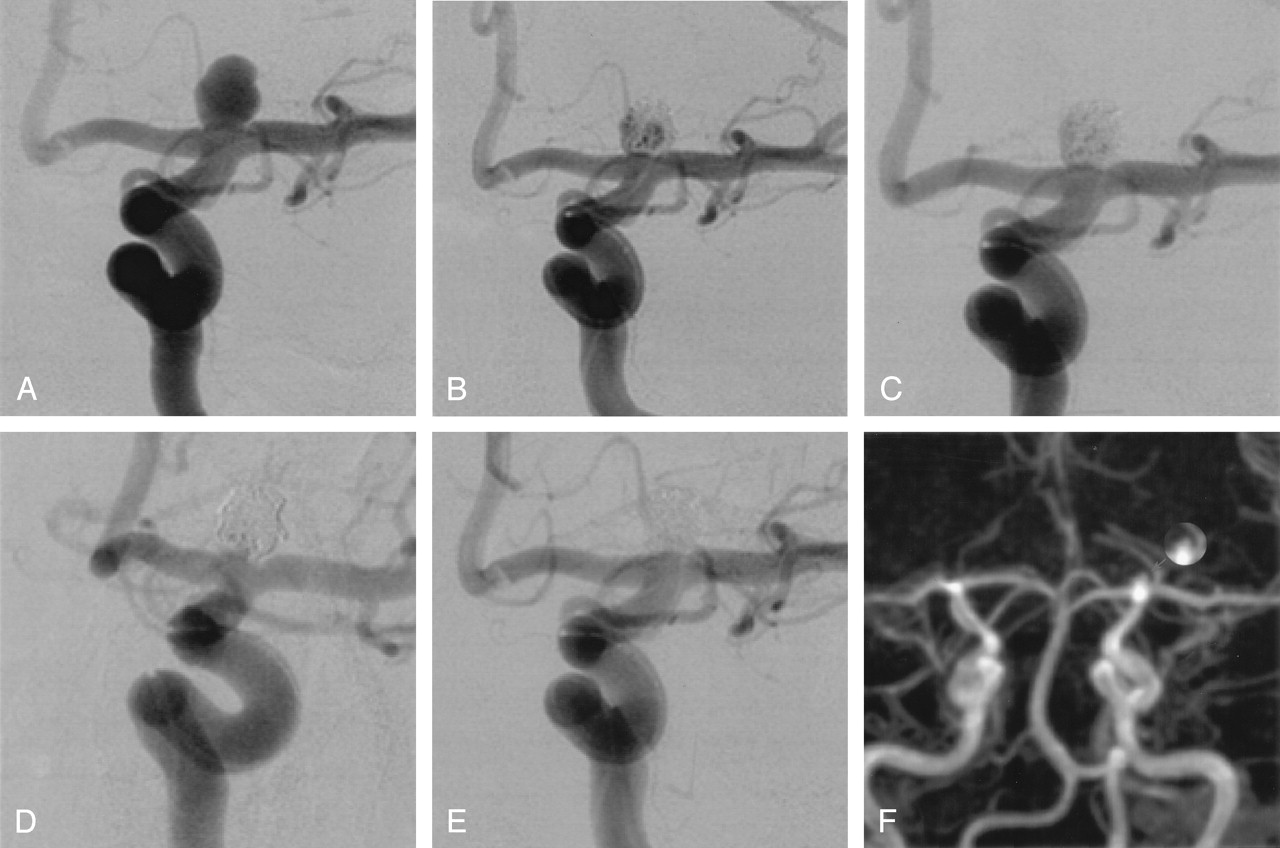
Incidental cerebral aneurysm in a 44-year-old woman.
A, Left ICA angiogram shows a round 7 mm aneurysm of the ICA bifurcation.
Selective coiling with complex Orbit coils only: four coils were delivered in a concentric fashion within the aneurysmal sac including a 7 mm/21 cm coil (B), a 4 mm/7 cm coil (C), a 3 mm/4 cm coil (D), and a 2 mm/2 cm coil.
E, Conventional angiogram at the end of the embolization shows a complete occlusion.
F, Follow-up MRA at 6 months shows a slight recanalization of the neck (arrow).
Results
Reliability of the Material
Endovascular treatment with complex Orbit coils alone was successfully performed in 16 patients. In four patients (patients 6, 7, 9, and 15), additional helical Orbit coils or GDC were required to complete aneurysm occlusion. In patients 6 and 15, the last 2 mm/1.5 cm complex coil could not be delivered because of its stiffness, and a 2 mm/2 cm helical coil (patient 6) and a 2 mm/3 cm Ultra-Soft GDC (patient 15) were placed instead to occlude the aneurysm neck. In a 73-year-old woman (patient 7) with a tortuous ICA, the microcatheter kicked back during delivery of the first complex coil. In this case, only Ultra-Soft GDCs were used allowing to occlude the aneurysmal sac with correct stabilization of the microcatheter. In a 50-year-old woman (patient 9) with a middle cerebral artery bifurcation aneurysm, a 4 mm/3 cm complex coil placed within the aneurysmal sac did not adapt a 3D configuration. Because of the nonoptimal basket, the coil was not detached and was retrieved. A 4 mm/4 cm 3D GDC was then delivered allowing to bridge the aneurysm neck. These four patients (20%) were judged as failure of endovascular treatment with complex Orbit coils.
In a most of cases (round-shape aneurysms), a 3D packing could be achieved by filling the aneurysms in a concentric fashion (Fig 3). In two cases of aneurysms with an unusual shape (length ≫ width), however, it was judged safer to fill the aneurysm in “segments” (Fig 2) to prevent from high tension on the aneurysmal sac.
A total of 55 complex Orbit coils were used and easily passed through the microcatheter without any friction in all cases. In all aneurysms, from two to five complex coils were placed to obtain good packing. During the delivery process, the first complex coils were adapted smoothly to the aneurysm wall without any tendency to move in a tumbling manner. These coils automatically assumed their configuration upon deployment except the 4 mm/3 cm complex coil that did not behave like a 3D coil. Smaller complex coils were then added and densely packed the aneurysms without any compartmentalization. At the end of the procedure, the last complex coil (2 mm/2 cm or 2 mm/1.5 cm) could be delivered in all cases but two (patients 6 and 15) despite their stiffness that is superior to that of helical coils. No stretching of complex coils was encountered during their repositioning.
The detachment of all coils immediately occurred except for two 5 mm/15 cm complex coils that could not be detached and were retrieved and then exchanged. There was no coil rupture or involuntary coil detachment. In two cases of wide-neck aneurysms treated with the remodeling technique (10, 11), all Orbit coils were easily delivered during balloon inflation. No technical complication occurred in the present series.
Anatomic and Clinical Outcome
Endovascular treatment—with complex Orbit coils alone—in 16 patients resulted in 14 complete occlusions and two neck remnants. The modified GOS was excellent in 14 patients and good in two. One patient (patient 13) with a grade IV SAH kept a mild hemiparesis despite uneventful and effective endovascular treatment. In one patient (patient 19) with a ruptured AcomA aneurysm, a thromboembolic complication resulted in an anterior cerebral artery infarct. The patient kept a mild lower limb weakness. Follow-up MRA at 6 months were obtained in all 16 patients and showed 14 complete occlusions, one neck remnant, and only one slight recanalization.
Discussion
This study shows that complex Orbit coils may be used in a concentric fashion for the endovascular treatment of intracranial aneurysms. Since the introduction of the first controlled-detachable coil (13), the indications for treatment of intracranial aneurysms have enlarged and several detachable coils systems with mechanical or electrolytical detachment are currently available (14–16). Although these platinum coils have proved to be reliable and effective (1, 6), neurointerventionalists face a major problem in the long-time course—namely, aneurysm recanalization due to coil compaction. To decrease it, many ongoing investigations are focusing on the development of biologically active coils (17), radioactive coils (18), coated-coils with a swelling hydrogel (19), and liquid polymer (20). The aims of these new therapeutic tools are to promote intraaneurysmal clot organization and fibrosis (17, 18) or increase the packing attenuation (19, 20), which is associated with higher long-term occlusion rate (4, 5). Another way to improve the packing attenuation—as suggested by a recent experimental study (7)—is to use 3D coils only to treat cerebral aneurysms. Indeed, Piotin et al (7) have shown optimal packing of silicon aneurysm model to be obtained by using complex-shaped coils. The packing attenuation was higher to that obtained after having used helical coils only or a combination of helical and complex coils. Complex coils have a propensity to form a 3D cage after deployment, and their conformability is superior to that of helical coils with subsequently less compartmentalization, allowing more homogeneous aneurysm filling. Orbit coils are the first that present 3D coils of all sizes, ranging from 2 to 20 mm.
This specific feature is a potential advantage over other available systems because it might help to increase the attenuation of coils within the aneurysm lumen. Furthermore, the combination of Orbit coil that are thicker (0.012 inch) than most other systems (0.010 inch) and 3D packing seems to reduce the number of coils that are needed to occlude intracranial aneurysms completely. Another advantage of the Orbit coil is the availability of a 2 mm-diameter complex coil, which may be useful to treat very small aneurysms. Our series confirms the feasibility and safety of this technique.
Moreover, imaging follow-up at 6 months showed a low rate of coil compaction, which suggests that 3D packing with thicker coils might decrease the recanalization rate of embolized aneurysms. These findings are in agreement with the conclusions drawn by Sluzewski et al (4); however, no angiographic control is available in the present study because our imaging protocol for the follow-up of coiled aneurysms includes only MRA at 6, 12, and 36 months. This is based on our previously published experience (21), so conventional angiography is only performed in our department if a potentially treatable recanalization is observed on MRA. Larger series with longer imaging follow-up are thus mandatory to confirm these preliminary results over longer periods of time.
Some technical limitations were encountered in this study: complex coils are stiffer than helical coils—because of their 3D configuration—and may limit aneurysm packing at the end of the treatment. In most cases, we did not observe this because complex Orbit coils are available at very small sizes. In three patients (6, 7, and 15), however, additional helical Orbit coils (one case) or Ultra-Soft GDC (two cases) were required to complete aneurysm embolization. These patients presented aneurysms that could not be safely treated without soft coils at the end of the procedure or Ultra-Soft coils for the entire treatment because of a kick-back effect on the microcatheter during delivery of stiffer coils. The other technical limitation concerned the 4 mm/3 cm complex coil that behaved like a helical coil rather than a complex coil (Patient 9) and did not bridge the aneurysm neck. In our study, the limiting characteristics of the complex Orbit coils included their relative stiffness and a 4 mm/3 cm coil that does not have a 3D configuration.
The size of the aneurysmal neck may be a limitation of the endovascular treatment because of coil protrusion into the parent artery. With the development of remodeling balloons (9, 10), most wide-neck aneurysms are now amenable to endovascular treatment. In the present study, the remodeling technique with Orbit coils proved to be effective in case of wide-neck aneurysms. No procedure-related morbidity or mortality was observed in our study, and immediate anatomic and clinical results were good or excellent in all patients.
Conclusion
Our study is the first that assess the feasibility of 3D packing with complex Orbit coils for the endovascular treatment of intracranial aneurysms. It shows that intracranial aneurysms may be packed with complex-shaped coils used in a concentric fashion. In this small series of aneurysms, with features largely favorable for stable long-term results from coiling, the incidence of recurrence at 6 months was very low. Nevertheless, additional, larger series with long-term follow-up are mandatory to confirm these preliminary results.
References
- Received August 24, 2004.
- Accepted after revision October 30, 2004.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Optimal first coil selection to avoid aneurysmal recanalization in endovascular intracranial aneurysmal coiling
- A carving method to determine an optimal working projection using three-dimensional volume rendering digital subtraction angiography in coil embolization of cerebral aneurysms
- Complex shaped detachable platinum coil system for the treatment of cerebral aneurysms: The Codman Trufill DCS and Trufill DCS Orbit Detachable Coil System COMPLEX Registry final results
- Analysis and quantification of endovascular coil distribution inside saccular aneurysms using histological images