
Abstract
SUMMARY: An unusual case of venous congestive encephalopathy associated with cavernous sinus dural arteriovenous malformation is reported. The parenchymal changes consisted of a well-demarcated area of hyperintensity on T2-weighted MR images involving the cortex and underlying white matter in the ipsilateral temporal and posterior frontal region. It showed mass effect and persisted for 2 years before evolving into a venous infarction.
Venous congestive encephalopathy has been well identified in the last few years in patients with dural arteriovenous malformations (DAVMs).1-3 The underlying venous hypertension mainly depends on the volume of arteriovenous shunting through the fistula and the resistance to venous outflow.4 MR imaging has been very useful in identifying parenchymal changes. DAVMs of the cavernous sinus usually follow a benign course and significant parenchymal changes and related clinical symptoms are rarely seen in these lesions. Mild chemosis, proptosis, bruit, and extraocular muscle palsies are the common presentations. We report a case of localized congestive encephalopathy in a case of DAVM of the cavernous sinus that initially posed a diagnostic difficulty and later evolved into a chronic venous infarction.
Case Report
A 48-year-old woman was being treated for seizures and mild chemosis/proptosis of the right eye for 3 months. She had been diabetic for 15 years and was under treatment for mild hypertension for the last 3 years. She had recurrent ptosis, diplopia on right side, headache, and blurring of vision during the last 2 years. A CT scan performed 2 years earlier was essentially normal.
Ophthalmic examination showed mild chemosis and proptosis of the right eye. There was no bruit over the eye or in the retroauricular region. Vision in the right eye was 6/9. The extraocular muscle movements were mildly restricted. There was no neurologic deficit in the limbs. A recent MR imaging showed an enlarged right cavernous sinus with flow void and a T2-hyperintense parenchymal lesion in the temporal and adjacent posterior frontal region (Fig 1A). Gyri in the affected region were swollen and hyperintense on T2-weighted images. Effaced sulci and mass effect on ipsilateral ventricle were seen. A focal T2 hyperintensity was also noted in the middle cerebellar peduncle on the right side (Fig 1B). Angiography was undertaken with a provisional diagnosis of cavernous carotid aneurysm and possibly a middle cerebral artery (MCA) branch territory infarction. Angiography showed a DAVM involving right cavernous sinus. It was fed by cavernous carotid branches as well as feeders from external carotid artery on the right side and minimal supply from the contralateral vessels. The right cavernous sinus was large. The venous drainage was restricted with only a mildly dilated right superior ophthalmic vein. The inferior petrosal sinus (IPS) was not shown. A prominent reverse drainage to sphenoparietal sinus and opacification of its cortical venous tributaries was seen (Fig 1C). The territory corresponded to the parenchymal lesion on MRI Partial reflux into the right superior petrosal sinus was also seen. A venous route approach for interventional treatment to the right cavernous sinus through IPS and also through angular vein failed. External carotid artery feeders were embolized with polyvinyl alcohol particles and the patient was asked to practice intermittent carotid compression as a therapeutic measure.

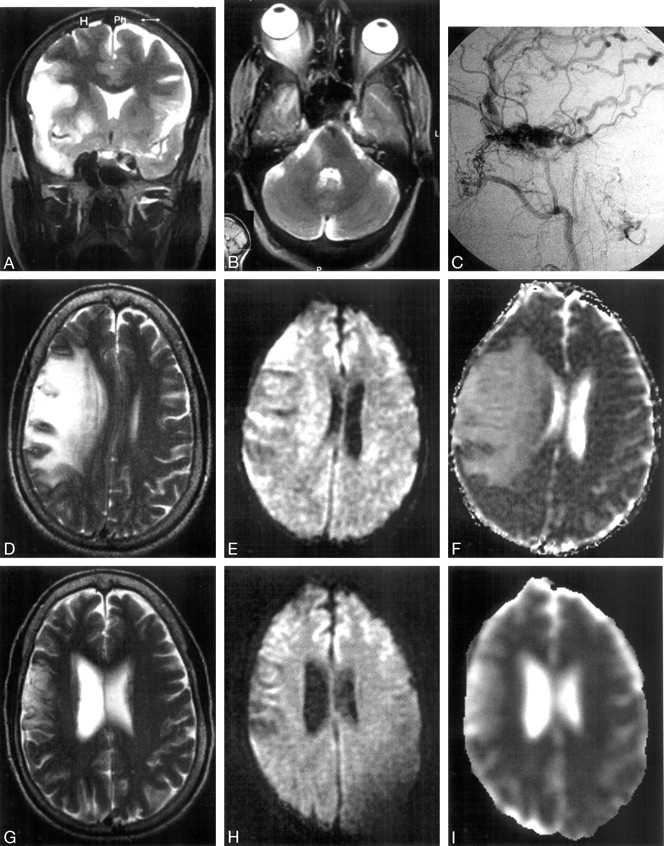
A, Coronal T2-weighted image shows an enlarged right cavernous sinus with flow void and a right temporofrontal parenchymal hyperintense lesion. B, Axial T2-weighted image shows the enlarged right cavernous sinus, a right middle cerebellar peduncle lesion, and right-sided proptosis. C, Lateral view of right external carotid angiography shows the DAVM. The right cavernous sinus is large and predominantly draining into spheno-parietal sinus and its tributaries. D, T2-weighted MR image 9 months later shows increased mass effect from the parenchymal lesion. Corresponding DW image (E) and ADC map (F) with values ranging from 1.2 to 1.6 × 10−3 mm2/s. G, T2-weighted MR image 24 months later shows venous infarction in the affected region with resolution of mass effect. DW image (H) and ADC map (I) with values ranging from 1.0 to 2.1 × 10−3 mm2/s.
Although arterial infarction was ruled out, at that stage the parenchymal lesion was not fully understood and ischemic/neoplastic processes were considered in differential diagnosis. The patient showed improvement in the eye signs. She underwent subsequent MR imaging 9 months later. The parenchymal lesion showed increase in size and mass effect and showed increased edema of the underlying white matter. Diffusion-weighted (DW) imaging was negative (Fig 1D–F). There were no new neurologic deficits, though an increase in the dose of antiepileptic drug was necessary in the intervening period. Eye signs suggested presence of residual DAVM. At this stage, the parenchymal lesion was suspected to be due to chronic venous insufficiency of the territory secondary to the DAVM. The patient refused any aggressive transorbital approach for interventional treatment or surgical treatment. Additional follow-up MR imaging 15 months later (24 months after the diagnosis was confirmed) showed regression in the size of the parenchymal lesion, the mass effect to have vanished, and the imaging was suggestive of chronic venous infarction in the affected territory (Fig 1G–I). The cavernous sinus returned to normal size and the right superior ophthalmic vein showed regression in size. The eye signs showed considerable resolution. The neurologic examination was within normal limits.
Discussion
DAVMs, often seen in the setting of chronic venous sinus occlusion, may show 3 similar main patterns of parenchymal involvement2: (1) brain swelling without abnormal signal intensity on T2-weighted images, (2) brain swelling with abnormal signal intensity on T2-weighted images but no hematoma, and (3) parenchymal hematoma and edema. Focal parenchymal enhancement, abnormal flow voids, and demonstrable abnormal vessels on MRA may be seen.2,5 In addition the occluded venous sinus(es) can be shown on MR venography. The first 2 patterns are regarded to be due to interstitial edema secondary to cortical venous drainage (CVD) and related venous congestion.2 The site of parenchymal involvement may be remote, and the changes reported are more diffuse in distribution.1,2,4 Aggressive lesions are usually present with seizures, focal deficits, cognitive impairment,4 and, in some cases, hemorrhage. Cortical venous reflux and/or stenosis of venous pathway are usually present in such patients. CVD was seen in 22/118 (19%) patients with DAVM of the cavernous sinus in a retrospective study by Stiebel-Kalish et al.6 Parenchymal changes other than enhancement, however, were not discussed in that report. The report suggests high probability of CVD in patients with bilateral eye signs 12/28 (43%). All 7 patients with neurologic signs/symptoms had CVD. Our patient had unilateral eye signs. In a series of 28 patients studied by Halbach et al,7 only one patient had cortical venous reflux to Sylvian vein. Pontine congestion related to the perimesencephalic drainage has been reported earlier in DAVM of the cavernous sinus.8,9 Presentation with seizures, a parenchymal lesion having a tumor-like MR imaging pattern, and the changes persisting for 2 years were the unusual features of our case with a cavernous sinus DAVM. Gyral swelling and chronic nature of the lesion, however, indicated a pathology other than tumor or arterial infarction, respectively. As has been seen in venous ischemia,10 DW imaging did not show any evidence of cytotoxic edema at that time and the parenchymal changes appeared to be related to venous hypertension, which led to pressure-driven interstitial edema. Isolated reports suggest that such changes may persist up to 2 years.2 It appears that successful therapeutic intervention at this stage could have salvaged the tissue involved. Reversal of imaging changes and clinical improvement after early intervention has been observed in some reports.1,2,4 Although an increase in antiepileptic dosage was required, the lack of focal deficits despite an increase in the interstitial edema and mass effect (Fig 1D) may be due to slow progression and also to the fact that the involved cortical territory was relatively noneloquent. The unchanged neurologic status at the chronic venous infarction stage supports the latter. In addition, the other factors could be (1) a maintained delivery of oxygenated blood as in venous sinus occlusive disease2 resulting in late as well as limited cell dysfunction/loss and (2) a reduced or resolving venous hypertension due to evolution of the primary lesion (ie, the DAVM). The localized involvement of parenchyma in our case matches with the drainage territory of sphenoparietal sinus and relates to the compromised venous drainage. Thus, the affected parenchyma had little alternative venous drainage available other than the sphenoparietal sinus affected by venous hypertension leading to focal congestive encephalopathy.
In conclusion, the report highlights an unusual presentation in a case of cavernous sinus DAVM. It also draws attention to the entity of focal or localized chronic venous ischemia later evolving into venous infarction.
References
- Received July 4, 2005.
- Accepted after revision July 25, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.