
Abstract
BACKGROUND AND PURPOSE: Patients with vertebral fractures containing intraosseous clefts may represent a distinct subgroup of vertebroplasty patients, yet the development of subsequent vertebral fractures in this population has not been explored. We tested the hypothesis that after vertebroplasty for intraosseous clefts, subsequent fractures would occur earlier and more frequently than after treatment of non–cleft-containing fractures.
METHODS: We retrospectively reviewed 362 patients treated with vertebroplasty for osteoporotic fractures. The location, frequency, and timing of subsequent fractures were compared between 2 subgroups: group 1, patients treated at fractures containing clefts, and group 2, treated patients without clefts. A vertebra-by-vertebra analysis was used to compare the relative risk and timing of subsequent fractures adjacent to vertebrae with or without clefts.
RESULTS: Group 1 included 63 patients treated at 65 vertebrae and group 2 included 250 patients treated at 399 vertebrae. Group 1 demonstrated a nearly twofold increased risk of subsequent fracture (odds ratio [OR], 1.90; 95% confidence interval [CI], 1.04–3.49, P = .037). At the vertebral level, the relative risk of subsequent fracture was 2.02 (95% CI, 1.46–2.58; P = .013) times greater adjacent to a treated cleft. Fractures adjacent to any treated level occurred significantly sooner than nonadjacent fracture (P = .0004). The presence of a cleft was not significantly associated with the timing of subsequent fractures.
CONCLUSIONS: Patients with osteoporotic vertebral fractures containing clefts are at increased risk for subsequent fractures and treatment of these clefts is associated with increased rates of adjacent fracture. There is no significant difference in the timing of subsequent fractures based on the presence of a cleft.
Percutaneous vertebroplasty has been in clinical use in the United States for almost 10 years and has been well described in a broad patient population.1–3 Patients presenting with intraosseous clefts, also known as Kummel osteonecrosis, represent a common subpopulation treated with vertebroplasty. Clinical series have demonstrated that clefts are quite common and that excellent pain relief can be achieved with vertebroplasty in these patients.4
There is an ongoing debate about whether vertebroplasty may cause subsequent fractures in nearby vertebrae. Numerous small clinical series have offered circumstantial evidence implicating vertebroplasty in subsequent fractures.5,6
In our practice and in others, early onset and increased rates of subsequent fractures of adjacent vertebrae have been noted after vertebroplasty in patients with intraosseous clefts (A.T. Trout, D.F. Kallmes, K.F. Layton, and K.R. Thielen, unpublished data). This observation may be due to the biomechanical effect of a focal, rigid mass of cement placed in a preexisting cleft during vertebroplasty. Alternatively, patients presenting with clefts may represent a subgroup of patients with particularly severe osteoporosis, which may put them at elevated risk for subsequent fracture.
In this study, we evaluated the potential adverse consequences of vertebroplasty in the setting of intraosseous clefts, specifically regarding the incidence and pattern of subsequent vertebral fractures. We subdivided our hypothesis into 2 main analyses: a patient-level analysis and a vertebra-by-vertebra analysis. At the patient level, we analyzed whether after vertebroplasty, patients with treated clefts suffered subsequent fractures more frequently and earlier than those without clefts. At the vertebral level, we tested whether vertebrae adjacent to treated clefts would fracture more frequently and earlier than vertebrae adjacent to treated levels that did not contain clefts.
Methods
We performed a retrospective review of all patients treated with vertebroplasty at our institution between July 1999 and September 2004. Four-hundred and thirty-one patients were treated during this interval. Institutional Review Board approval was obtained for this study and all patients had previously consented to the use of their medical records for research purposes. Reviews of these records were Health Insurance Portability and Accountability Act (HIPAA) compliant. Of the 431 patients treated, 362 (83.9%) were treated for vertebral fractures that were osteoporotic in nature and were selected for this analysis. Patient records were reviewed for evidence of intraosseous clefts in the vertebrae treated with vertebroplasty and for evidence of subsequent vertebral fractures after vertebroplasty. Intraosseous clefts were identified with preprocedural MR imaging or based on the cement filling pattern documented in the procedural reports (Figs 1 and 2). Subsequent fractures after vertebroplasty were diagnosed with MR imaging or bone scan based on previously described criteria.7–9 In brief, altered signal intensity (high intensity on T2-weighted MR imaging and corresponding low signal intensity on T1-weighted imaging), distinct fracture lines, or vertebral deformation observed on MR imaging or increased tracer uptake on bone scan, were used to identify subsequent fractures.

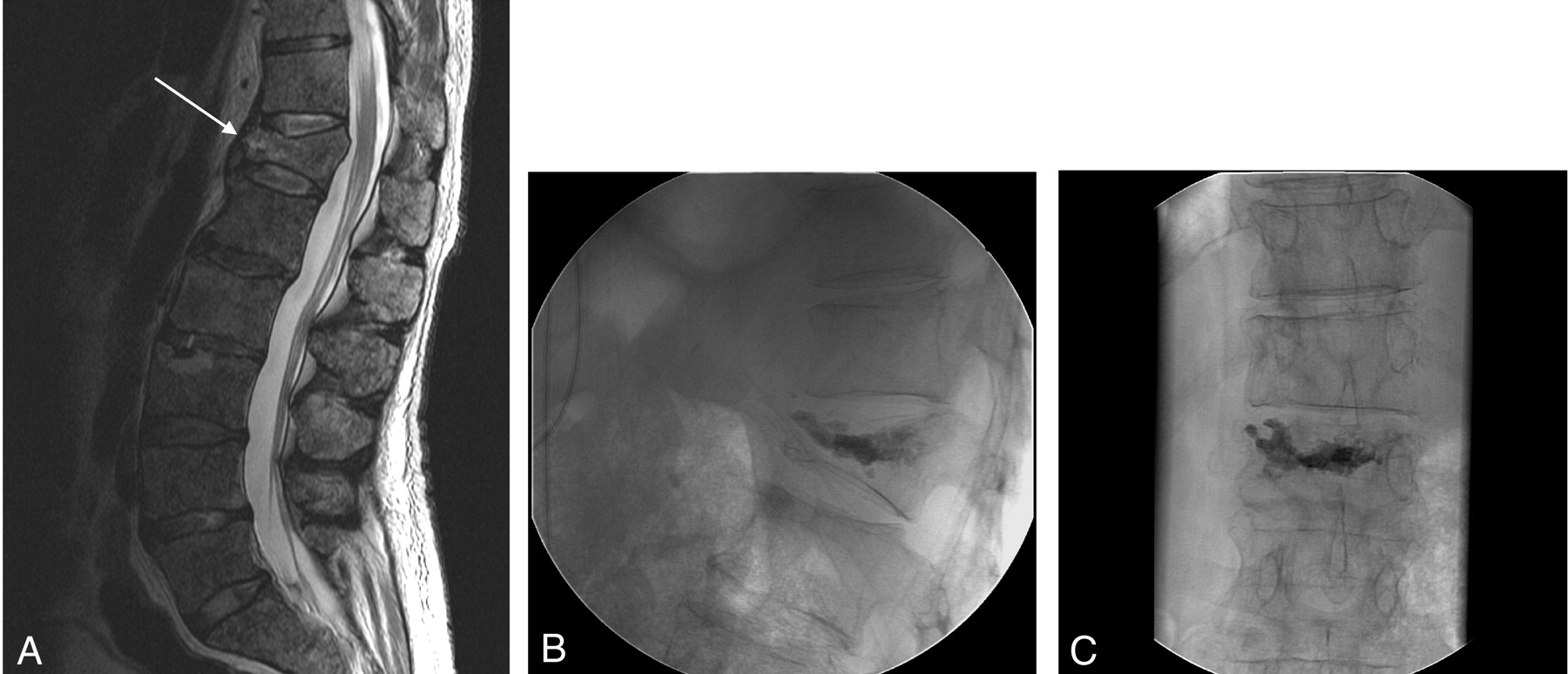
Prevertebroplasty MR imaging (A) and intraoperative fluoroscopic images (B and C) of the treated level in a patient with an intraosseous cleft. T2-weighted (repetition time [TR]/echo time [TE], 2800/102 fast spin-echo with fat-saturation) MR (A) demonstrates acute compression of L2 in this 82-year-old male patient. The arrow indicates a fluid-filled cleft within the fractured vertebra. The lateral (B) fluoroscopic image shows filling of the cleft in the anterior portion of the vertebral body with little trabecular pattern to the implanted cement. A more typical trabecular filling pattern is seen in the posterior aspect of the treated vertebral body on the lateral projection.
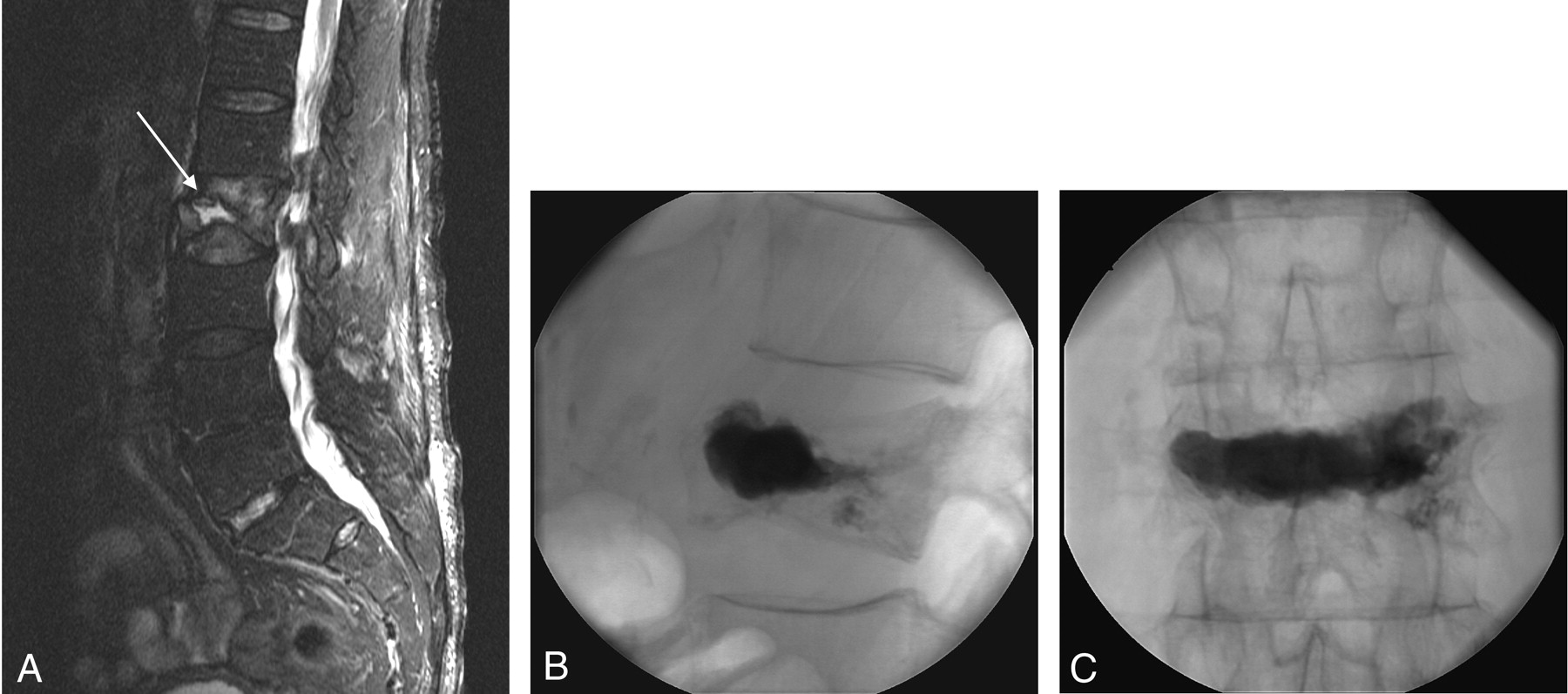
Prevertebroplasty MR imaging (A) and intraoperative fluoroscopic images (B and C) of the treated level in a patient without an intraosseous cleft. T2-weighted (repetition time [TR]/echo time [TE], 3300/150 fast spin-echo, without fat saturation) MR (A) demonstrates acute compression of T12 in this 61-year-old male patient. Lateral (B) and anteroposterior (C) fluoroscopic images after vertebroplasty at T12 show cement evenly distributed among the trabeculae of the fractured vertebral body.
The timing of subsequent fractures was determined based on the date of confirmatory imaging. All vertebroplasty patients were encouraged to call or return to the clinic with any new or worsening symptoms. If clinically warranted, images were obtained at the time of subsequent visit. Scheduled radiographs, however, were not obtained.
Vertebroplasty Procedure
Percutaneous vertebroplasty is offered to patients with refractory pain that is referable to an acute or subacute vertebral compression fracture of the thoracic or lumbar spine as evidenced on MR imaging or bone scan. Vertebroplasty is not offered when the exclusion criteria are met: improvement with conservative management, technical contraindications, and pain that does not localize to the known fracture.
Vertebroplasties were performed by staff radiologists according to the methods outlined previously.10 Specifically, patients were treated by using intravenous conscious sedation. Biplane fluoroscopy was used in all cases. Local anesthesia was administered in the skin, subcutaneous tissues, muscular tissues, and over the periosteum of the targeted pedicle. Transpedicular or parapedicular trajectories were used in all cases. Eleven- or 14-gauge needles were advanced into the central aspect of the vertebral bodies for unipediculate approaches, whereas placement of the needle was made into the midportion of the hemivertebra for bipediculate approaches.
Cement was prepared as described previously.10 In brief, polymethylmethacrylate powder was combined with sterile barium sulfate for opacification and gentamicin powder for infection control, followed by the addition of liquid monomer to make a thin, “cake-glaze” consistency material. The mixture was then injected with either an injector device (Cook Inc.; Bloomington, Ind) or 1-mL syringes. Cement injection was considered complete when the cement reached the posterior quarter of the vertebral body on the lateral projection. Injection was immediately terminated in the event of epidural, venous, or trans-endplate extravasation. After needle removal, patients were left on strict bed rest for 1 hour and then discharged.
Patient Groups
The 362 patients included in this analysis were divided into 2 groups. Group 1 included those patients who harbored an intraosseous cleft at 1 or more levels treated with vertebroplasty (Fig 1). Group 2 included patients without an intraosseous cleft at any level (Fig 2).
Statistical Comparison of Fracture Distribution
A Monte Carlo Approximation for the Fisher Exact Test was used to compare the distribution along the spinal axis of treated fractures based on the presence or absence of intraosseous clefts as well as to compare the distribution of subsequent fractures based on the presence of a cleft in the previously treated vertebra.
Statistical Comparisons of Groups
Risk of Subsequent Fracture Based on the Presence of Intraosseous Clefts, Patient-by-Patient Analysis.
Using χ2 analysis and the odds ratio (OR) statistic, we compared the rate of subsequent fracture between groups 1 and 2. The purpose of this comparison was to identify whether patients with treated intraosseous clefts at any vertebral level are, as a group, at increased risk for subsequent fracture. Hypothesis testing of the OR was performed by using the Z statistic for a 2-tailed distribution with a null hypothesis of OR = 1.
Timing of Subsequent Fracture, Patient-by-Patient Analysis.
Using survival analysis and the logrank statistic, we compared the time to subsequent fracture after vertebroplasty between groups 1 and 2. Specifically, we were investigating whether patients with a cleft at any treated vertebral level develop subsequent fractures sooner than those without.
Risk of Subsequent, Adjacent-Level Fracture Based on the Presence of Intraosseous Clefts, Fracture-by-Fracture Analysis.
Using the relative risk calculation, we compared the rate of subsequent fracture adjacent to treated vertebrae based on the presence or absence of an intraosseous cleft in the treated level. Adjacent level fracture was defined as fracture of either of the 2 vertebrae that share intervertebral disks with the treated level. For this analysis, L5 was defined as having only one adjacent level (L4) and we included only subsequent fractures after the initial vertebroplasty in a given patient. Fractures that occurred after subsequent vertebroplasty (or vertebroplasties) in that patient were excluded to prevent the difficulty of determining to which vertebroplasty the subsequent fractures were related. Hypothesis testing with a null hypothesis of RR = 1 was performed by using the Z statistic for a 2-tailed distribution.
Timing of Subsequent Fracture, Fracture-by-Fracture Analysis.
In addition to analyzing the timing of subsequent fractures at the patient level, we performed the same analysis at the level of individual vertebrae. This analysis was performed to assess fracture timing based on perceived risk with adjacent vertebrae considered to be at increased risk for subsequent fracture. Nonadjacent vertebrae, however, were considered to be at less risk for fracture because they are not associated with a treated cleft-bearing level.
For this analysis, each fracture was considered independently, and survival analysis and the logrank statistic were used for the after analysis. First, the time to subsequent fracture was determined based on whether the fracture occurred adjacent or nonadjacent to the treated level, regardless of the presence of an intraosseous cleft. Second, we looked at nonadjacent, subsequent fractures and adjacent subsequent fractures as independent groups and analyzed the time to fracture based on the presence or absence of a cleft in the treated level. The purpose of this analysis was to assess whether fractures of vertebrae adjacent to a treated cleft-bearing level have a different time course than fractures both adjacent to non–cleft-bearing levels and nonadjacent to any treated level (cleft or non–cleft-bearing). Statistical software used for all analyses was JMP version 5 (SAS Institute, Cary NC) or SAS version 8.02 (SAS Institute, Cary NC).
Results
Five hundred and seventy-three vertebral levels were treated in the 362 selected patients during the examined time interval. Forty-nine patients (13.5%) were treated at both cleft- and non–cleft-containing vertebrae and were excluded from further analysis, leaving 313 patients treated at 463 vertebral levels. Sixty-three (20.1%) of these patients had evidence of intraosseous clefts in a total of 65 treated vertebral levels (Fig 3). These patients were designated as group 1. Two hundred and fifty patients were treated at only non–cleft-bearing vertebrae (group 2). Intraosseous clefts were diagnosed on the basis of MR imaging in 12 (19.0%) of the 63 patients. The remaining clefts were diagnosed intraoperatively. There was no significant difference in the distribution along the neuraxis of treated fractures based on the presence or absence of a cleft (P = .07) (Fig 3).

Location of treated vertebrae divided based upon the presence or absence of clefts. Data are depicted as a percentage of each subgroup. The distribution of treated vertebrae is similar between patients with and without documented intraosseous clefts. In accordance with previous descriptions,4,13 there is an increased incidence of fractures and clefts at the thoracolumbar junction in our patient population.
Seventy-three (23.3%) of the 313 selected patients developed 126 subsequent vertebral fractures after vertebroplasty. In group 1, 21 (33.3%) patients suffered a total of 28 subsequent vertebral fractures. In group 2, 52 (20.8%) patients suffered 98 subsequent fractures. This frequency was significantly different (see below).
The distribution over the spinal axis of subsequent fractures was similar regardless of the presence or absence of an intraosseous cleft in a previously treated vertebra (P = .95) (Fig 4). In addition, no particular region of the spine seemed to be particularly at risk for developing subsequent fractures.

Location of subsequent vertebral fractures divided based upon the presence or absence of an intraosseous cleft in a previously treated vertebral level. Data are depicted as a percentage of each subgroup. The distribution of subsequent fractures is similar regardless of the presence or absence of a cleft in the previously treated level. In addition, no specific zone of the spine seems more likely to develop subsequent fractures.
Analysis of Risk of Subsequent Fracture
Risk of Subsequent Fracture Based on the Presence of Intraosseous Clefts, Patient-by-Patient Analysis.
Patients with a documented cleft in any treated vertebral level were significantly more likely to incur subsequent fracture (χ2 = 0.036). Specifically these patients had almost a twofold increased risk of subsequent vertebral fractures compared with patients without intraosseous clefts (OR = 1.90, 95% CI = 1.04 to 3.49, P = .037).
Risk of Subsequent Adjacent-Level Fracture Based on the Presence of Intraosseous Clefts, Fracture-by-Fracture Analysis.
Based upon the locations of the 463 treated vertebral bodies, 656 adjacent levels were considered at risk for subsequent fracture. This number is less than the 926 hypothetical adjacent levels (2 × 463) because of the presence of pre-existing fractures, adjacent treated levels, and only a single adjacent level for L5. Seventy-nine vertebrae containing clefts and 385 non–cleft-containing vertebrae were treated with vertebroplasty yielding 121 and 535 at-risk adjacent levels, respectively. Sixteen (13.2%) of 121 at-risk vertebrae adjacent to treated clefts subsequently fractured. Thirty-five (6.5%) of 535 at-risk vertebrae adjacent to treated levels without clefts subsequently fractured (relative risk 2.02 [95% CI = 1.46–2.58, P = .013]).
Timing of Subsequent Fractures
Patient-by-Patient Analysis.
Among the cohort of patients presenting with subsequent fractures, the median times to diagnosis of a fracture group 1 versus group 2 were 47 days (range, 6–766 days) and 83 days (range, 2–1330 days), respectively. This difference was not statistically significant (logrank = 0.34).
Fracture Level Analysis.
Subsequent fractures adjacent to any treated level in either group 1 or 2 occurred significantly sooner than fractures nonadjacent to a treated level (median 57 and 127 days, respectively, logrank = 0.0004). This effect remained within the individual groups as well, with adjacent level fractures occurring sooner in both patients with and without intraosseous clefts at any vertebral level (logrank = 0.024 for cleft patients and 0.009 for noncleft patients).
Nonadjacent level fractures occurred on a similar time course between groups 1 and 2 (median, 314 and 116 days, respectively; logrank = 0.60). In addition, although there was no significant difference in the timing of adjacent level fractures between groups 1 and 2, there was a trend toward significance (median 31 and 70 days for cleft and noncleft, respectively; logrank = 0.089).
Discussion
In this study, we compared the location, frequency, and timing of subsequent fractures among patients treated with vertebroplasty at vertebrae with and without pre-existing clefts. Our data suggest that among patients with osteoporotic vertebral compression fractures, the presence of a treated cleft is associated with a rate of subsequent fracture higher than that seen in patients without preexisting clefts. Specifically, these patients have nearly a twofold increased risk of subsequent fracture after vertebroplasty. Further, at the vertebral level, the risk of subsequent fractures adjacent to treated clefts was twofold greater than that adjacent to non–cleft-bearing, treated vertebrae. Although there is an increased rate of subsequent fracture associated with treatment of cleft-bearing vertebrae, there is no significant difference in the timing of these subsequent fractures.
It is difficult to prove whether the increase in fracture risk associated with clefts observed in this study results from abnormal biomechanics or simply reflects the nature of the underlying pathologic condition. It is possible that intraosseous clefts are a marker for aggressive osteoporosis with high risk of subsequent fractures. To date, however, there is no evidence in the literature that these patients suffer from a distinct pathologic condition. In addition, the finding in the current study that the time course of subsequent fractures is not significantly different in patients with intraosseous clefts casts doubt on this possibility. If these patients truly had a more aggressive form of osteoporosis, one would reasonably expect that subsequent fractures would occur at shorter time intervals. Regardless, there is clearly a need for specific analysis of the subpopulation of patients with intraosseous clefts to determine whether their disease is significantly different from that of patients without intraosseous clefts.
Even without absolute proof that treatment of intraosseous clefts with vertebroplasty causes subsequent fractures, the data presented here may still be of use to practitioners. Based on the findings presented, it may be appropriate to specifically address the potential elevation in risk for subsequent fracture during the consent process before vertebroplasty in patients with cleft activity. In addition, we believe that the high rate of subsequent fractures adjacent to treated clefts warrants consideration of a trial of prophylactic vertebroplasty in the vertebrae adjacent to treated clefts.
Prior studies have suggested that vertebroplasty may lead to early-onset, subsequent vertebral fractures,11,12 and this effect is observed in our patient population (note that these data are derived from a subset of the same population that has previously been used to demonstrate this effect [A.T. Trout, D.F. Kallmes, and T.J. Kaufmann, unpublished data]). Although there is no specific association between vertebroplasty at cleft-bearing vertebrae and the timing of subsequent fractures, the data presented here reaffirm the association between vertebroplasty in general and early onset adjacent level fractures. Unfortunately, these data cannot necessarily be generalized because the results were based on a cohort of patients with and without intraosseous clefts, and there is no control group that was not treated with vertebroplasty.
There is broad agreement that clefts occur primarily at the thoracolumbar junction,4,13 and this was observed in our patient population. Osteoporotic vertebral compression fractures in general are known to occur more commonly at the thoracolumbar junction as well.14,15 Based upon these observations, one might conclude that the perceived increased risk of subsequent fracture adjacent to clefts simply reflects the tendency for subsequent fractures to cluster in the thoracolumbar region. Our data, however, do not support this conclusion. The distribution of baseline fractures did not differ based on the presence of a cleft, and subsequent fractures were similarly distributed regardless of the presence of an intraosseous cleft in a previously treated vertebral body. In addition, subsequent fractures occurred at similar frequencies at all levels between T7 and L5. These findings suggest that neither baseline cleft-bearing fractures nor subsequent fractures were location-dependent.
Although we consider our data provocative, the issues surrounding percutaneous treatment of cleft-bearing vertebrae deserve further research. An analysis of the population of patients with pre-existing clefts is warranted to determine whether these patients differ significantly from the typical vertebroplasty population in terms of t score, fracture severity, or other variables. In the general osteoporotic population, bone mineral attenuation and increasing fracture severity have previously been shown to be associated with the risk of subsequent fractures.16–18 It is possible that patients with intraosseous clefts possess these or other risk factors unique to a cleft-forming pathologic condition that leads to an increased fracture rate.
The finding of increased subsequent fracture associated with treated clefts also raises the issue of the biomechanical properties of the implanted cement. The increased stiffness and rigidity of the cement, particularly as a focal mass within a cleft, may contribute to the observed effect. Thus, we believe that development of a more compliant cement is warranted.
Finally, these data may indicate the need for further evaluation of kyphoplasty and the growing practice of overfilling clefts in an attempt to gain height restoration during vertebroplasty. Specifically, it may be valuable to consider the biomechanical effects of these procedures in light of our results demonstrating an increased risk of subsequent fracture after treatment of cleft-containing vertebrae. In kyphoplasty, artificial clefts are created before cement infusion and thus each treated vertebra contains a focal cement mass. To our knowledge, no data exist that compare subsequent fracture rates and timing after vertebroplasty and kyphoplasty. With regard to the practice of overfilling clefts to achieve height restoration, infusion of larger than necessary volumes of cement into cleft-bearing vertebrae may further increase the risk of subsequent fracture. Thus, this procedure should be further evaluated and, until that time, performed with caution.
This study suffered several limitations. Most importantly, the study is retrospective in nature. In addition, we considered each fracture after vertebroplasty as a separate occurrence regardless of whether the fracture occurred alone or in temporal association with other vertebral fractures. Although we felt this was the best way to account for the relationship between the subsequent fracture and the treated level, it does not account for the possibility of fracture clustering.19 Another limitation of this study is that subsequent fractures were identified on the basis of imaging performed in response to worsening or new symptoms. Because scheduled radiographs were not obtained, subclinical fractures may have been missed and the exact timing of the subsequent fracture cannot be determined. Finally, although patients without intraosseous clefts were used as a control group for those with preexisting clefts, a true control population of patients who were not treated with vertebroplasty was not used.
Conclusion
Patients with osteoporosis-induced vertebral compression fractures containing intraosseous clefts are at increased risk for subsequent fracture. Specifically, treatment of cleft-containing vertebrae with vertebroplasty is associated with increased fracture of adjacent vertebrae. There is, however, no temporal association between clefts treated with vertebroplasty and subsequent fractures.
Footnotes
This research was presented in abstract form for presentation at the 2005 Annual Meeting of the Radiological Society of North America.
References
- Received August 8, 2005.
- Accepted after revision November 22, 2005.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Asymptomatic and Unrecognized Cement Pulmonary Embolism Commonly Occurs with Vertebroplasty
- Subsequent Fracture after Percutaneous Vertebroplasty Can Be Predicted on Preoperative Multidetector Row CT
- Teriparatide and Raloxifene Reduce the Risk of New Adjacent Vertebral Fractures in Postmenopausal Women with Osteoporosis: Results from Two Randomized Controlled Trials
- Clinical Outcomes with Hemivertebral Filling during Percutaneous Vertebroplasty
- Efficacy of Percutaneous Vertebroplasty for Multiple Synchronous and Metachronous Vertebral Compression Fractures
- Vertebroplasty for the Treatment of Traumatic Nonosteoporotic Compression Fractures