
Abstract
SUMMARY: We report the case history and radiologic findings of a patient with a biopsy-proven dendritic cell histiocytoma presenting as a single intracranial extra-axial mass and no systemic disease. Even though this entity is relatively rare, it should nevertheless be considered in the differential diagnosis of dural-based space-occupying central nervous system lesions.
A 10-year-old African American girl presented with a 1-year history of headache worsening over the last 6 months and associated with vomiting for 2 weeks. She denied any constitutional symptoms, and her neurologic examination was unremarkable. A brain MR imaging study showed a 3.3 × 2.9 × 2.9 cm, minimally lobulated, enhancing extra-axial mass centered in the right parafalcine location with minimal extension across the falx associated with leftward midline shift (Fig 1B). There was significant edema of the frontal lobes with T2/fluid-attenuated inversion recovery hyperintensity of the white matter bilaterally (Fig 1A). 2D time-of-flight intracranial MR venogram showed focal obstruction of the anterior aspect of the superior sagittal sinus and collateral drainage through a left parasagittal vein. She subsequently underwent a subtotal surgical resection, because the danger of bleeding from cortical veins made total tumor removal unacceptably risky. Frozen sections were inconclusive, but final pathology revealed a dendritic cell histiocytoma. The tumor cells (Fig 2) were large, with a glassy, pink cytoplasm and prominent single nucleoli. The mitotic activity was low, and necrosis was absent. Numerous markers for epithelial, central nervous system, or lymphoid lineage and for melanoma were negative. Immunostains for CD68, factor XIIIa (macrophage and histiocyte markers), were positive, but CD1a and S100 immunostains were negative. The tumor was identified as a “non-Langerhans cell” dendritic cell histiocytoma.

MR imaging findings of the tumor at presentation. A, Axial T2-weighted and (B) axial postcontrast T1-weighted images demonstrate an avidly enhancing extra-axial mass centered in parafalcine location bilaterally, mainly on the right. C, After surgical intervention. Axial postcontrast T1-weighted image shows resection of the tumor locating in the right parafalcine location with a residual tumor at the superior sagittal sinus and left parafalcine region.
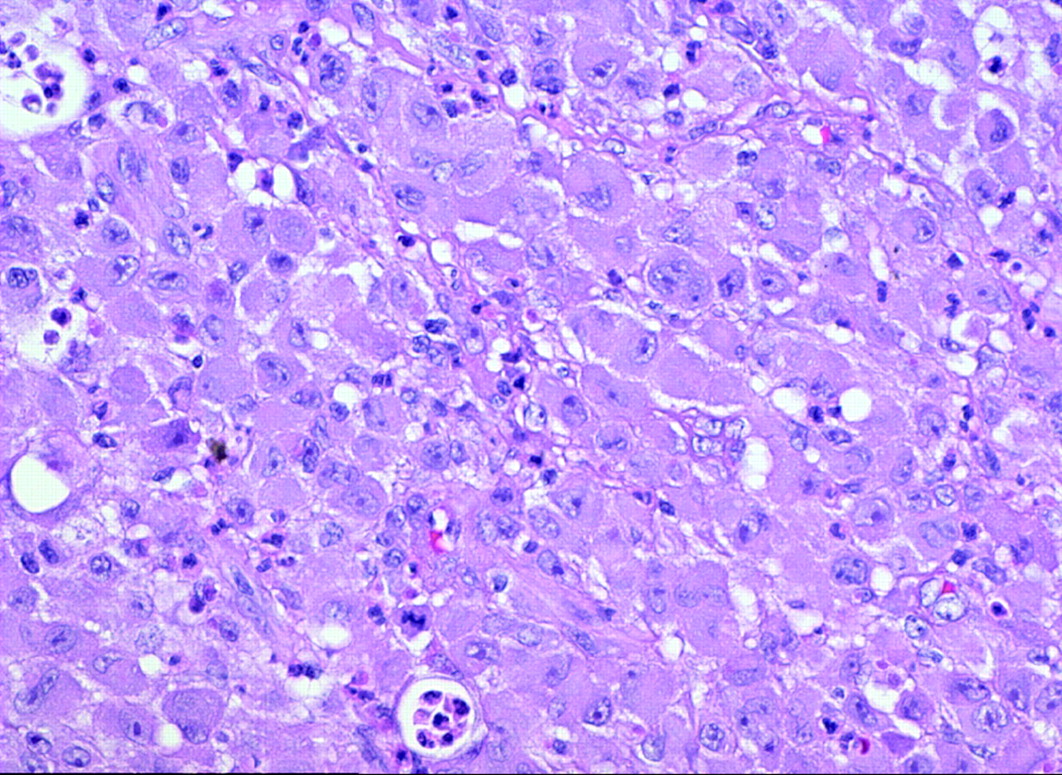
Pathology smears from surgical specimen. The lesion is composed of sheets of large cells with prominent glassy, eosinophilic cytoplasm and prominent red nucleoli. Mitotic activity was minimal. Hematoxylin-eosin stain, original magnification ×250.
The patient's headaches subsided postoperatively. Neurologic examination remained normal after her operation. Her postsurgical imaging revealed some residual left parafalcine tumor adjacent to the superior sagittal sinus with surrounding vasogenic edema. The midline shift had resolved (Fig 1C). The patient was placed on steroid therapy and pain medication for headaches due to postoperative edema. She completed 14 sessions of radiation therapy. Since that time, she has been on steroid therapy with pain medication with no improvement of her headaches. Follow-up MR studies have demonstrated a slight decrease in the size of tumor with decreasing surrounding edema.
Discussion
We present the radiologic findings of a patient with biopsy-proven dendritic cell histiocytoma presenting as a single intracranial extra-axial mass with no systemic disease. Two lines of cellular differentiation for histiocytes have been described in the literature with important functional, morphologic, and phenotypic similarities: the dendritic cells and the cells derived from the macrophage-monocyte series. Immunophenotyping is particularly useful to differentiate macrophages that are characteristically phagocytic cells with prevalent antigen-processing functions from dendritic cells with predominately antigen-presenting capabilities.1,2
The World Health Organization classifies this tumor as a solitary histiocytoma with various dendritic cell phenotypes.3 These phenotypes are illustrated in the Table.4,5 Although most often cutaneous,6–8 these lesions can develop elsewhere. They have been described in the cervical lymph nodes, the mediastinum, the spleen, the axilla, the oral cavity, the thyroid gland, the peripancreatic soft tissues, and the spine.9–12 Cases of juvenile xanthogranulomas (JXG), which are derived from dermal dendrocytes and benign fibrous histiocytomas (BFH), tumors composed of fibroblastic and histiocytic cells, have been described in the central nervous system.13,14 A careful review of the literature revealed no similar cases of supratentorial dural-based dendritic cell histiocytoma other than 12 such lesions reported briefly by Jaffe and Favara in abstract form.15 In 4 of those patients, the lesion involved dura and/or adjacent bone.
Identifying features of dendritic cells
The radiologic findings of this extra-axial tumor are nonspecific. On noncontrast brain CT, the mass appeared nodular and hyperattenuated extending into the superior sagittal sinus. The lesion enhanced avidly. It was relatively dark on T2-weighted scans. In addition, increased signal intensity on diffusion-weighted images with corresponding decreased signal intensity on an apparent diffusion coefficient map indicated some restricted diffusion, probably reflecting hypercellularity. Such features suggest an aggressive lesion without pointing to a specific diagnosis.
Until further characterizing features of these types of tumors are delineated with MR spectroscopy and/or positron-emission tomography, the differential diagnostic possibilities remain wide. An aggressive meningioma should be suggested at first even in a patient of this age, though most meningiomas occur in the middle decades of life. A hemangiopericytoma tends to occur in younger patients than those with typical meningiomas and more often in men,16 but is still rare in children. Dural metastases, lymphoma, amyloidoma, and plasmacytomas may be suggested by a history of HIV infection, systemic lymphoma, myeloma, or a primary malignancy. Also, granulomatous diseases, such as sarcoidosis, tuberculosis, or fungal infection, should be suspected when compatible systemic symptoms are present.17 Rare tumors such as JXG and BFH with dural attachment should be considered, though they are uncommon without systemic involvement and/or cutaneous and subcutaneous soft tissue lesions.13,14
Clinically, dendritic cell histiocytomas, though biologically benign, have the capacity to recur and progress, especially if incompletely resected, as was the case with our patient. Radiation therapy after complete surgical removal may prevent recurrence. A careful follow-up is essential, because these lesions can predict more systemic and serious histiocytic processes.3,13
References
- Received February 15, 2007.
- Accepted after revision May 24, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.