
Abstract
SUMMARY: One of the goals of neuroimaging in acute ischemic stroke is to identify those patients whose outcome will be improved by therapeutic intervention. This article will discuss the design, analysis, and interpretation of clinical research studies carried out to establish the accuracy and clinical value of neuroimaging to select such patients.
Pathophysiology of Preventable Infarction
With acute obstruction of an artery supplying blood to the brain, there is a reduction in the cerebral blood flow (CBF) to the area of the brain that was perfused by the artery. This reduction in CBF is most severe in the central perfusion territory of the artery and becomes increasingly less so in more peripheral areas where collateral circulation from other arteries provides additional flow (Fig 1).1 A series of cellular biochemical and pathophysiologic changes occur in response to the reduced CBF, which, with time, can lead to cell death. If removal of arterial obstruction and re-establishment of blood flow occurs quickly, some of the cells that would have died will recover normal function and some will die anyway.2 Thus, in the early hours after cerebral arterial occlusion, the area of the brain with reduced blood flow consists of a mixture of cells that are already irreversibly damaged and destined for death along with some that exhibit abnormal biochemical changes and will go on to die later but may recover if the biochemical processes leading to cell death are interrupted by pharmacologic treatment or re-establishment of CBF. Because the rapidity at which cell death occurs depends not only on the magnitude and duration of the CBF reduction but also on individual properties of the cells, irreversibly damaged cells are more common in the central areas with the greatest reduction of blood flow, whereas potentially salvageable cells are more common in the periphery. However, there will be some variation due to the degree of heterogeneity of the individual cellular responses (Fig 2).2

Diagrammatic representation of the distribution of CBF following acute obstruction of an artery supplying blood to the brain. There is a reduction in the CBF to the area of the brain that was perfused by the artery. This reduction in CBF is most severe in the central perfusion territory of the artery and becomes increasingly less so in more peripheral areas where collateral circulation from other arteries provides additional flow.

Diagrammatic representation of the state of brain tissue following acute obstruction of an artery supplying blood to the brain. For the sake of simplicity, the different tissue states are shown as concentric rings. In reality, cells from the different types of tissue will be intermixed to some degree.
The goal of therapy for acute ischemic stroke is to intervene to prevent death in those vulnerable cells that are still alive but whose natural history is to die because of insufficient CBF. Clearly, the earlier the intervention occurs, the more likely such vulnerable cells will exist. However, human ischemic stroke is a very heterogeneous disease, and the time of onset is not always known with certainty. A method to identify those patients who have vulnerable brain cells that are still alive but whose natural history is to die would be a great advantage, first, in testing the efficacy of acute stroke interventions and, then, in applying the interventions to the general population. One of the goals of neuroimaging of acute ischemic stroke is to identify such areas of preventable infarction in the brain.
Simply put, areas of preventable infarction have 2 characteristics: The cells in them will die if untreated and will live if treated. As noted previously, the existence and extent will be time-dependent. Biochemical and pathophysiologic (and therefore neuroimaging) characteristics that define preventable infarction may be different, depending on the treatment. The cells that can be salvaged by a neuroprotective strategy that interferes with a specific biochemical pathway in the absence of reperfusion may be different from the cells salvaged by reperfusion.
Neuroimaging of Preventable Infarction
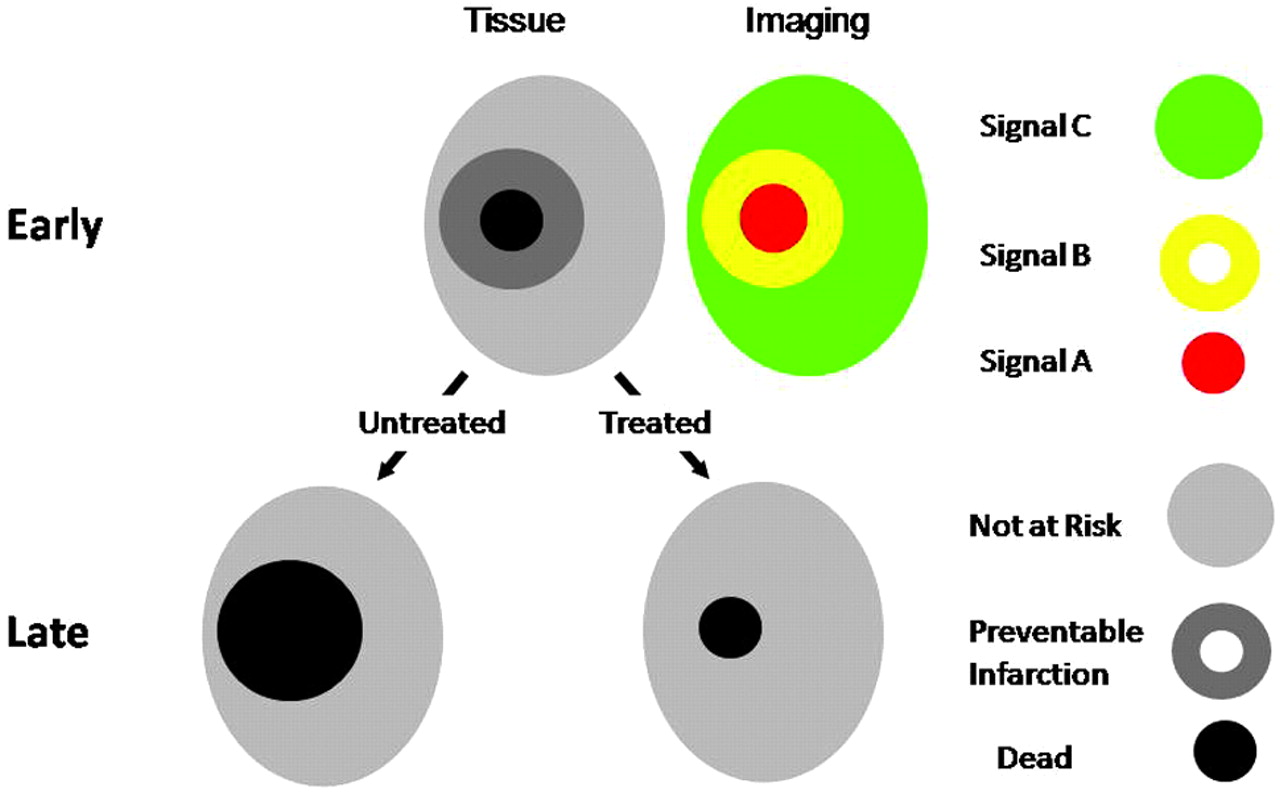
Neuroimaging of preventable infarction requires 3 neuroimaging signals that spatially match the 3 pathophysiologic tissue types in the brain with acute cerebral ischemia: dead (signal A), preventable infarction (signal B), not at risk (signal C) (Fig 3). To accurately identify preventable infarction, the 3 signals must meet the criteria in the Table. Fulfilling these criteria is not easy. The essential elements of an experimental protocol to establish the accuracy of a neuroimaging method to identify preventable infarction are the following:
) Two groups
Untreated (natural history).
Treated.
) Two images
Early physiologic imaging, before therapy, to define regions A, B, and C.
Late structural imaging to define the area of infarction.
) Documentation of effective treatment

Neuroimaging of preventable infarction requires 3 neuroimaging signals that spatially match the 3 pathophysiologic tissue types in the brain with acute cerebral ischemia: dead (signal A), preventable infarction (signal B), not at risk (signal C). The state of the tissue is in gray-scale. Imaging results are in color.
Criteria to establish accurate neuroimaging of preventable infarction
In the case of reperfusion, documentation of effective treatment will require a third image to show those areas that have been successfully reperfused.
The demonstration in untreated patients that signal A reliably predicts 100% cell death, that signal C reliable predicts 100% cell survival, and that signal B has an indeterminate outcome is not sufficient to conclude that signal B accurately identifies preventable infarction. Simply because region B is homogeneous in its neuroimaging characteristics, does not mean it is homogeneous biochemically and pathophysiologically. It may be that signal B cannot distinguish between a mixture of dead cells and tissue not at risk (Fig 4).

The demonstration in untreated patients that signal A reliably predicts 100% cell death, that signal C reliable predicts 100% cell survival, and that signal B has an indeterminate outcome is not sufficient to conclude that signal B accurately identifies preventable infarction. Simply because region B is homogeneous in its neuroimaging characteristics does not mean it is homogeneous biochemically and pathophysiologically. It may be a mixture of dead cells and tissue not at risk between which signal B cannot distinguish (lower row). The state of the tissue is in gray-scale. Imaging results are in color.
Clinical Value of Neuroimaging of Preventable Infarction
Even the demonstration of the accuracy of neuroimaging to identify preventable infarction by these criteria does not show clinical value. Clinical value can be proved only by demonstrating in a randomized controlled trial (RCT) that there is an improvement in patient outcome that depends on the use of the neuroimaging technique. Rigorous designs for such trials can use either 1 RCT or 2 sequential RCTs:
) Single RCT design
Group 1
Does not receive imaging—none treated.
Group 2
Does not receive imaging— All treated.
Group 3
Receives imaging to guide therapy.
Preventable infarction—treated.
No preventable infarction—not treated.
) Two sequential RCTs design
RCT 1 without imaging—shows no treatment benefit.
RCT 2—eligibility criteria identical to that of RCT 1. All enrolled subjects receive imaging before treatment. The Echoplanar Imaging Thrombolytic Evaluation Trial is an example of this design.3
In both of these designs, the patients who received treatment based on neuroimaging must have a better outcome than all the other groups, to prove the clinical value of neuroimaging. The advantages of these trial designs are that they directly test the hypothesis of the added value of imaging and account for the true cost of imaging (adverse events, delay in initiating therapy, and added expense). The disadvantage is that the sample sizes will be very large unless there is a high fraction of those with preventable infarction who benefit.
A slightly less rigorous design uses 2 sequential RCTs:
) RCT 1 without imaging—shows no treatment benefit.
) RCT 2 with a design identical to that of RCT 1 but with imaging added to the eligibility criteria—shows treatment benefit.
Although this design also directly tests the hypothesis of the added value of imaging, it does not necessarily account for the true cost of imaging because all potentially eligible subjects receive imaging but only those who meet imaging criteria are enrolled. The expense and adverse effects of imaging on those not enrolled may not be accurately accounted for. The Carotid Occlusion Surgery Study (COSS) of extracranial-intracranial bypass surgery to prevent subsequent stroke in patients with recently symptomatic internal carotid occlusion is an example of this design (www.cosstrial.org). The original EC/IC Bypass trial showed no benefit of surgery in patients with recently symptomatic internal carotid artery occlusion selected by clinical and arteriographic criteria.4 COSS uses essentially the same eligibility criteria but has added ipsilateral increased cerebral oxygen extraction fraction measured by positron-emission tomography.
Less rigorous RCT study designs that do not account for the cost of imaging can be used to investigate the clinical benefit of neuroimaging-guided therapy in acute imaging. These include the following:
) Single RCT
All subjects receive imaging.
Prespecified analysis shows that treatment benefit is only in those with preventable infarction.
) Single RCT
Imaging part of eligibility criteria.
The problem with these designs is the failure to prove that imaging criteria are necessary to select patients who will benefit from therapy because there is no demonstration of the lack of benefit when imaging criteria are not used. The first design does not adequately account for potential deleterious effects of imaging on outcome. If imaging has significant adverse events or delays time-sensitive treatment, its use may adversely affect the outcome in the treated patients who do not meet imaging criteria, leading to the erroneous conclusion that they did not benefit from therapy. Similarly, the second design leaves open the possibility that the patients who meet all eligibility criteria other than imaging would benefit as well.
Conclusions
Demonstrating the accuracy and clinical value of neuroimaging to select patients with acute ischemic stroke who have preventable infarction requires rigorously designed carefully conducted clinical research. This article provides guidelines for the design, analysis, and interpretation of such research to facilitate the process of investigating and validating the role of neuroimaging in acute stroke care.
Footnotes
This research was supported by the H. Houston Merritt Distinguished Professorship in Neurology.
Paper previously presented in part at: Advanced Neuroimaging and Acute Stroke Meeting, September 7–8, 2007; Washington, DC; and the Annual Meeting of the Radiological Society of North America, November 26, 2007; Chicago, Ill.
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}
{kind=link}