
Abstract
BACKGROUND AND PURPOSE: Our aim was to detail revascularization results, including impact on outcome and mortality, in the Interventional Management of Stroke (IMS) II trial.
MATERIALS AND METHODS: IMS II was designed to obtain estimates of the efficacy and safety of reduced-dose intravenous recombinant tissue plasminogen activator (rtPA) followed by additional intra-arterial rtPA and low-energy sonography via the EKOS Primo Micro-Infusion Catheter at the occlusion in selected patients with ischemic stroke treated within 3 hours of onset. Revascularization outcomes were detailed and compared with modified Rankin Scale scores 0–2, mortality outcomes, and results from IMS I.
RESULTS: Complete recanalization at 60 minutes occurred in 12 of 29 (41.4%) sonography microcatheter–treated occlusions. Complete recanalization was achieved at 2 hours or procedure end in 20/29 (68.9%) in the ultrasound catheter–treated group, and final thrombolysis in cerebral infarction (TICI) 2/3 reperfusion was achieved in 18/29 (62.0%) ultrasound-treated subjects. Fifteen-minute angiograms demonstrated some recanalization in 69/145 (46.7%) sonography microcatheter treatment intervals, compared with 39/111 (35.1%) in IMS I treatments in 23 subjects with reliable 15-minute angiograms (P = .046). Pooled IMS I-II data demonstrated that partial or complete recanalization occurred in 56/75 (74.6%) and good reperfusion (TICI 2/3) occurred in 46/75 (61.3%) of internal carotid artery T and M1 occlusions. Revascularization correlated with good outcome for TICI 2/3 reperfusion (P = .0004), TICI 2B/3 reperfusion (P = .0002), and arterial occlusive lesion 2/3 recanalization (P = .03).
CONCLUSION: IMS II provides evidence that the EKOS Primo sonography microcatheter exhibits a trend toward improved recanalization of the occlusion compared with a standard microcatheter and again confirms the correlation between recanalization and reperfusion with good clinical outcome and reduced mortality.
The Interventional Management of Stroke (IMS) I trial suggested that the combined use of reduced-dose intravenous (IV) Activase (alteplase, recombinant tissue plasminogen activator [rtPA]; Genetech, South San Francisco, Calif), followed by microcatheter-delivered intra-arterial (IA) rtPA, was relatively safe and may be clinically useful in selected patients with acute ischemic stroke, as compared with similar subjects treated with a full dose of IV rtPA in the National Institute of Neurologic Disease and Stroke (NINDS) rtPA trial.1 It had long been anticipated that multiple interventional methods might be applicable within an IV/IA rtPA paradigm and that these methods might further improve revascularization and clinical outcomes.2 Encouraged by the safety and potential efficacy reports in a small feasibility trial of the MicroLysUS Sonography Catheter (EKOS Corp, Bothell, Wash) (hereafter referred to as the sonography microcatheter), the IMS Investigators initiated another phase II trial (IMS II) to further study its use following reduced-dose IV rtPA therapy.3 This article reports in detail the revascularization, clinical, and safety outcomes in the IMS II trial, with emphasis on results obtained with the Primo sonography microcatheter (EKOS Corp), including general as well as detailed comparisons with revascularization outcomes from IMS I.
Methods
The IMS II study was a 13-center open-labeled single-arm pilot study, whose purpose was to determine the futility or lack thereof of the combined IV/IA therapy and to obtain preliminary estimates of the efficacy and safety of reduced-dose IV rtPA (0.6 mg/kg), 15% as a bolus with the remainder infused for 30 minutes, followed by additional rtPA (≤22 mg) and low-energy sonography via the sonography microatheter at the site of the arterial occlusion in eligible patients who were younger than 81 years of age with acute large ischemic strokes (National Institutes of Health Stroke Scale [NIHSS] ≥ 10) treated within 3 hours of symptoms onset.4
The EKOS system consists of 2 components: 1) a single-use 3F sonography microcatheter with an end-hole infusion lumen incorporating a high-frequency (1.7 mHZ) cylindrical sonography transducer delivering sonography at low power (<0.45 W) into a 3.3F distal tip, and 2) a reusable control unit, which provides the sonography energy source and the user interface. Three models of the sonography microcatheter were used sequentially in the trial. The first model (SV2510), similar to that used in a feasibility trial, was intended for passage over a 0.010-inch microguidewire. When successful access occurred in only 2 of 6 subjects between January 26, 2003, and April 1, 2003, the IMS II Steering Committee temporarily stopped the trial to change to a 0.014-inch guidewire-based system (SV3014) and to upgrade the control unit. The trial was restarted May 5, 2003. However, unsuccessful access in 2 of 4 subjects again prompted study delay in anticipation of a new third model under development. This Primo model was used for the remainder of the trial between December 17, 2003, and April 12, 2005. This report will focus on the Primo sonography microcatheter efficacy. Details of study design, objectives, study protocol, sonography microcatheter and standard microcatheter administration of IA rtPA, and medical management and evaluation have recently been published and are not repeated here.4
Revascularization was measured according to recanalization of the primary arterial occlusive lesion (AOL), and reperfusion was measured by a modified Thrombolysis in Cerebral Infarction (TICI) score.5,6 AOL recanalization and the modified TICI perfusion were scored as grades 0–3 (Table 1). The protocol primary study revascularization end point was 100% complete recanalization of the primary occlusion at (AOL 3) at 60 minutes, compared with complete standard microcatheter thrombolysis at 60 minutes in the IMS I trial. Secondary revascularization measures included both AOL 3 recanalization and TICI 2/3 reperfusion at 120 minutes or at the end of the procedure, compared with 60 comparable occlusions (internal carotid terminus [ICA T], M1, M2, vertebrobasilar) in the IMS I trial.
Terminology and definition of TICI reperfusion (I) and AOL recanalization scores (II)*
In addition, any recanalization of the AOL by using a sonography microcatheter at each sequential 15-minute interval was recorded and compared with standard microcatheter recanalization at each sequential 15-minute interval from IMS I subjects with comparable occlusions as well as with standard microcatheter use in comparable IMS II occlusions.
The revascularization study end points were determined at the Clinical Coordinating Center at the University of Cincinnati by a central reader (T.T.). Operators were asked to ascribe Thrombolysis in Myocardial Infarction (TIMI) recanalization scores for their procedures, as had been recorded in IMS I. Operators’ scores were compared with the scores of the central core lab.
The clinical efficacy measure of modified Rankin Scale (mRS) score 0–2 outcome at 3 months and mortality were also recorded, and both these measures were further analyzed according to revascularization status. Revascularization end points were also compared with mRS score 0–2 outcome and mortality from the IMS I study.
Finally, recanalization and reperfusion data from the sonography and standard microcatheter groups from IMS II and IMS I were pooled to estimate good outcome and mortality results that might be achieved with ICA T and M1 occlusions with the IV/IA rtPA paradigm.
As a primary safety measure, CT scans within the first 36 hours after completion of rtPA infusion were monitored for intracerebral hemorrhage (ICH) and contrast deposition, including contrast extravasation (CT attenuation >90 HU, hyperattenuation persisting at 24 hours) and contrast enhancement (high attenuation disappearing within 24 hours).7 ICH was classified according to the European Cooperative Acute Stroke Study (ECASS) classification, subdivided into hemorrhagic infarction (HI) types 1 and 2 and parenchymal hematoma (PH) types 1 and 2.8 Infarct, symptomatic ICH, and lesion (infarct + ICH) volumes were retrospectively measured digitally via a manual region-of-interest analysis and reported (G. Ramadas, personal communication, August 2006). Vessel perforation, dissection, and subarachnoid hemorrhage were also recorded.
Angiograms were examined for reocclusion during the procedure as well as for new occlusions in previously uninvolved arterial distributions. Distal emboli in the middle cerebral artery (MCA) beyond an MCA occlusion could not be systematically identified because their pretreatment presence/absence was seldom confidently identified or excluded. Baseline and new emboli into the anterior cerebral artery (ACA) distribution with MCA and ICA T (obstructed ICA flow into the M1 and A1 segments) occlusion were recorded. Microcatheter contrast injections (MCI) were recorded and compared with contrast extravasation and ICH.9
Catheter-tip temperature was recorded for all IMS II procedures by using the EKOS sonography microcatheter and reviewed postprocedure. Temperature graphs were compared with 15-minute control angiograms to identify whether observed temperature changes correlated with recanalization.
A National Institutes of Health–appointed Data and Safety Monitoring Board Committee reviewed all safety and outcome results of the IMS I and II Studies.
Results
Eighty-one subjects were entered into the IMS II trial (Fig 1). Twenty-six were treated with IV rtPA only, and 55 were treated with IV and IA rtPA. Among the 26 treated with IV-only, 2 improved clinically following IV rtPA and did not have arteriography, undergoing MR angiography (MRA) instead with no major AOL. Twelve others had no major treatable AOL at arteriography, 2 with no demonstrable AOL and 10 with distal MCA, ACA, or posterior cerebral artery occlusions not treated by the interventionist. Of these 14 with no major AOL demonstrated on angiography or MRA, mRS 0–2 was achieved in 9 (64.3%).

Patient flow and treatment group designation for 81 subjects entered into IMS II.
Of the remaining 12 IV-only subjects, 1 was discovered to have a high international normalized ratio and was excluded from IA treatment. One subject had coarctation of the aorta, and the ascending aorta could not be accessed in the usual retrograde transfemoral fashion for diagnostic arteriography and treatment. Three subjects were beyond the prescribed 5-hour initiation time; 2 had nonprotocol IA treatments other than rtPA, both with good outcomes. The other 7 subjects in the IV-only group had AOL eligible for IA treatment. Five had major intracranial occlusions distal to cervical ICA occlusions that could not be accessed due to inability to traverse the cervical ICA occlusions. One M2/3 occlusion was neither identified nor treated by the local treating interventionist. An early sonography microcatheter model would not traverse the distal ICA in another due to cervical and cavernous segment ICA tortuosity. MR spectroscopy 0–2 outcomes were achieved in 3 of these latter 7 (42.9%) subjects not treated by IA therapy.
Fifty-five subjects were treated with both IV and IA rtPA (36 by sonography microcatheter and 19 by standard microcatheter). Thirty-five subjects had the final Primo sonography microcatheter model introduced. This catheter could not be advanced beyond tortuous segments of the ICA in 3 subjects (8.6%), who were then treated with a standard microcatheter. Three subjects were treated without sonography initiated: 2 regionally in the setting of ICA and vertebral artery dissection, respectively, and 1 when the catheter-control box interface cable connection failed. Twenty-nine subjects were treated with the Primo microcatheter with sonography activation. One of the 29 subjects had both an M2 AOL treated with the sonography microcatheter and a P2 occlusion treated with a standard microcatheter.
As noted, 19 subjects were treated by standard microcatheter, including 4 in whom the sonography microcatheter advancement had been unsuccessful. In addition, there were 1 ACA and 4 M3 occlusions in which the sonography microcatheter was not indicated. One other subject had an extremely tortuous cervical ICA and the appearance of intracranial atherosclerosis, in whom the sonography microcatheter was not indicated. Four other subjects had incomplete occlusions, and IA rtPA was administered via standard microcatheter. The occlusion of 1 subject was accessed after 5 hours, and a sonography microcatheter was not introduced. The 4 other subjects had sonography-microcatheter-eligible occlusions but were treated with a standard microcatheter, according to the discretion of the operator.
Revascularization Outcome
The primary study revascularization end point of complete recanalization of the primary AOL at 60 minutes was met in 12 of 29 (41.4%) patients with the Primo microcatheter with sonography activation. None of the 4 early sonography microcatheter models used achieved complete recanalization at 60 minutes. Complete recanalization of the primary AOL at 2 hours or by procedure end was achieved in 20/29 (68.9%) of the Primo microcatheter–treated group. Twenty-three control IMS I subjects had reliable 60-minute images for comparison of this primary end point, and 7 (30.4%) had complete recanalization (P = .41). By the end of the procedure in IMS I, 32/60 (53.3%, P = .08) patients with comparable AOLs (no M3, M4) exhibited complete recanalization (Fig 2). Recanalization in 14 patients with comparable IMS II AOL treated by standard microcatheter was compared with sonography microcatheter recanalization as well and demonstrated a cumulative 15-minute recanalization graph line that lies in close proximity to the 60-minute and 120-minute recanalization data points from the IMS I dataset (Fig 2).

Graph depicts total cumulative complete grade 3 AOL recanalization at each 15-minute interval for the EKOS Primo sonography microcatheter (n = 29) and the standard microcatheter in IMS II (n = 14). Standard microcatheter recanalization data points at 60 and 120 minutes are also depicted. IMS I data are incomplete at 60 minutes, with 23 confirmed control arteriograms. Sixty- and 120-minute IMS I data points closely approximate the line of IMS II microcatheter recanalization. The open circle emphasizes an early equivalence of standard microcatheter to the sonography (US) microcatheter. The greatest recanalization effect (>20%) is within the first 15 minutes of microcatheter placement.
Recanalization of the primary AOL leads to reperfusion into distal vessel segments. Final TICI 2/3 perfusion for the 29 Primo sonography microcatheter–treated subjects was 62.0%, compared with 56.8% for a comparable IMS I IA–treated group. No significant revascularization or outcome differences existed between IMS I and II.
Sequential 15-minute control IMS II angiograms demonstrated some recanalization, however small in degree, in 69/145 (46.7%) sonography microcatheter treatment intervals, compared with 28/65 (43.1%) comparable IMS II microcatheter treatments (P = .09) and 39/111 (35.1%) comparable IMS I treatments in 23 subjects in whom reliable 15-minute angiograms were available (P = .046).
Central core lab IMS II final TIMI revascularization scores demonstrated a 41% discrepancy between the core lab and the treating interventionist, with the treating interventionist usually scoring higher (better revascularization).
Revascularization Outcome versus mRS 0–2 Clinical Outcome
Table 2 presents mRS 0–2 outcomes for ICA T and M1 occlusion in IMS II and I subjects combined, according to multiple target revascularization end points. These pooled data demonstrate that partial or complete recanalization (AOL 2/3) occurred in 56/75 (74.6%), and good reperfusion (TICI 2/3) occurred in 46/75 (61.3%) of ICA T and M1 occlusions. Pooled data demonstrate that revascularization correlates with good outcome for TICI 2/3 reperfusion (P = .0004), TICI 2B/3 reperfusion (P = .0002), and AOL 2/3 recanalization (P = .03) end points, compared with failure to achieve those end points, respectively. TICI 2A reperfusion correlated to better outcome than TICI 0/1 (P = .03). In addition, a trend toward better mRS 0–2 outcome was found for TICI 2B versus 2A reperfusion (P = .08).
mRS 0–2 outcomes and mortality with 75 ICA T (n = 29) M1 (n = 46) occlusions according to TICI reperfusion and AOL recanalization in IMS I and II*
Although only 10/23 (43.5%) M2 occlusions achieved grade 3 AOL recanalization, 16/23 (69.5%) achieved mRS 0–2 outcome. Two subjects with M2 occlusions, both of whom recanalized and were discharged to home, were lost to follow-up and are included in the mRS >2 group. Comparison of the TICI 2/3 and AOL 2/3 end points as predictors of mRS 0–2 outcome shows a sensitivity of 90.5% versus 95.2% and a specificity of 52% versus 34%, respectively.
Revascularization Outcome versus Mortality
Overall IMS II mortality was 16% of subjects, similar to the 16% mortality in IMS I. Of the 13 deaths, 4 were treated IV rtPA-only; 1 died secondary to symptomatic intracerebral hemorrhage (SICH) following failure to identify and treat an M2–3 occlusion. Three others died from sequelae of a large cerebral infarction: 1 of the 3 had an ICA occlusion that could not be traversed for IA therapy, a second was not treated after the 5-hour limit, and the third had coarctation of the aorta that could not be traversed for IA therapy. Of the 9 (16.3%) IV/IA deaths, 4 (44.4%) subjects did not recanalize to AOL grade 3, and 6 (66.6%) did not perfuse to TICI 2/3. Overall mortality and mortality in revascularized and nonrevascularized subjects with ICA T and M1 occlusions are further detailed in Table 2. Reduced mortality was associated with TICI 2/3 reperfusion (P = .01), TICI 2B/3 reperfusion (P = .05), and AOL 2/3 recanalization (P = .03), compared with failure to meet those revascularization end points. Mortality in subjects failing to achieve either TIMI 2/3 reperfusion or AOL 2/3 recanalization was <40% for both end points.
Safety Outcomes
Symptomatic ICH occurred in 8/81 (9.9%) subjects with IMS II, including 1/26 (3.8%) treated with IV rtPA alone and 1 in a sonography microcatheter–treated subject without sonography applied. Six subjects in the sonography microcatheter group experienced symptomatic ICH, including the following:
One subject with M2 occlusion and baseline serum glucose concentrations of 400 mg/mL and creatinine concentrations of 2, who recanalized completely (AOL 3) to TICI 2B flow within 30 minutes.
One subject with a nonrecanalized M1 occlusion distal to the striate arteries who experienced severe cervical ICA spasm and additional thrombus development.
One subject with a nonrecanalized M1 occlusion distal to the striate arteries.
One subject with a T occlusion who recanalized within 30 minutes, with an unusual pattern of cortical/subarachnoid hemorrhage following on-the-table ICH.
Two subjects with recanalized M1 occlusion and angiographic evidence of pseudoaneurysm of the distal striate artery rupture following microcatheter contrast injections.
Of these 6 subjects, 5 had NIHSS ≥20. Four SICHs were PH1, and 2 were PH2, based on digital volume measurement. Mean hematoma volumes in these 6 SICHs measured 23.5 mL, representing 27.9% of lesion volume, compared with 25.2 mL, or 37.1% of lesion volume, for 6 nonultrasound IMS II and IMS I SICHs.
Three of the 7 SICHs had microcatheter injections. An early concern regarding a potential link between microcatheter injections and ICH with this paradigm was transmitted to investigators.9 No direct vessel perforation, primary subarachnoid hemorrhage, or intracranial dissection was documented in IA-treated subjects. Four (7.3%) reocclusions (3 complete) occurred during the procedure in 55 IA-treated IMS II subjects. New emboli in the ACA distribution were identified in 1/22 (4.5%) M1/M2 occlusions and in 1/14 (7.1%) ICA T occlusions in IMS II.
Other Results
Retrospective temperature analysis provided 93 IMS II data points available with both arteriographic and temperature data for retrospective analysis in the sonography-treated subjects. Temperature decreases of as little as 0.2–0.3°C could be readily identified. Forty (41.9%) temperature decreases were identified. Forty-five (48.3%) recanalizations or microcatheter retractions were identified. Temperature analysis provided 81% sensitivity, 90% specificity, 85% positive predictive value, 87% negative predictive value, and 84.9% accuracy in identifying recanalization or catheter retraction on the following arteriographic sequence.
Available 24-hour CT lesion volumes demonstrated no significant differences in IMS II infarct volumes compared with IMS I subjects overall or to those treated by combined IV/IA methods.
Discussion
The IMS II trial was designed to study the safety and potential efficacy of a sonography microcatheter in the recanalization of acute intracranial artery occlusions in acute ischemic stroke, following reduced-dose IV rtPA therapy. Both clinical and technical factors contributed to the actual use of a sonography microcatheter in only 33 subjects. Clinical exclusions for AOL location and etiology (atherosclerotic occlusion, dissection) occurred. Technical problems (difficulty and failure in catheter passage, connector cable problem, etc) further limited sonography administration and evaluation in several subjects. Other potentially eligible subjects were excluded on the basis of clinical, angiographic, or other operator-defined exclusion factors.
When used per protocol, the Primo sonography microcatheter demonstrated a trend toward achieving faster and more complete AOL recanalization compared with standard microcatheter use in IMS II, with an incomplete 60-minute dataset from IMS I and with the complete 120-minute dataset from IMS I (Fig 2), though these differences were not statistically significant. It might be unduly optimistic to expect that new revascularization methods would achieve a statistical benefit compared with a widely accepted active therapy in a small trial.
Standard microcatheter use in IMS I and II allowed mechanical manipulation of thrombus, including microcatheter and microguidewire passage and drug delivery distal to the occlusion initially, as well as 15-minute guidewire/microcatheter advancement. On the other hand, sonography microcatheter use was limited to proximal bolus and drip infusion, with no guidewire manipulation beyond that required for initial and subsequent microcatheter advancement. Figure 2 suggests an early recanalization equivalency or advantage for the standard microcatheter; this potential advantage may actually be a mechanical one due to microcatheter/guidewire manipulation of favorably predisposed occlusions in the setting of IV rtPA activity. Allowing microguidewire/sonography microcatheter manipulation in a similar fashion may further enhance recanalization potential and may lead to greater in revascularization effect.
Several other important observations are suggested from Fig 2. In addition to the apparent initial 15- to 30-minute equivalence of standard microcatheter use, Fig 2 also demonstrates that the initial 15-minute period actually achieves the greatest recanalization effect for both the sonography microcatheter (21%) and the standard microcatheter (24%) in IMS II overall. This also may be due to mechanical manipulation of favorably predisposed occlusions. It also demonstrates a relatively linear increase in recanalization effect with time, suggesting that failure to achieve recanalization in any time period does not predict failure in subsequent periods. In addition, the 60-minute recanalization data points of 23 IMS I subjects with reliable images and the 120-minute data points of 53 IMS I subjects with T, M1, M2, or vertebrobasilar occlusions lie in close proximity to the 15-minute line of 14 IMS II standard microcatheter cases. This suggests reproducible results in achieving complete recanalization with the standard microcatheter.
Identification of 14/81 (17.2%) subjects without AOL qualifying for IA sonography microcatheter thrombolysis confirmed pre-IMS and IMS I study observations: IV rtPA may recanalize some vessels early, leading to normal findings on arteriograms (n = 2) or distal occlusions (n = 10) (Fig 1).1,10 Any comparison of recanalization rates by using IA-only revascularization methods with the combined approach in IMS I and II with studies of must take into account this early recanalization achieved after IV therapy.
It is not possible to accurately compare recanalization and reperfusion results achieved with the combined IV/IA rtPA therapy paradigm with other reported IA revascularization methods in which treatment was initiated later. The 78% AOL 3 recanalization and 83.3% TICI 2/3 reperfusion of isolated M1 occlusion in IMS II, comparable with 78% for both measures in IMS I, may represent a true recanalization and reperfusion benefit compared with results obtained with r-pro-urokinase treatment in the Prolyse in Acute Cerebral Thromboembolism (PROACT II) study (67% TIMI 2/3 for M1 and M2 occlusions) and with the Multimechanical Embolus Removal in Cerebral Ischemia (MERCI) retriever in the MERCI and Multi-MERCI trials (45% and 54% TIMI 2/3, respectively).11,12 However, it still remains uncertain that revascularization end point definitions and application in the IMS studies are comparable with other revascularization studies.
A relationship between both AOL and TICI revascularization end points and mRS 0–2 outcome was demonstrated for ICA T and M1 occlusion (Table 2). TICI 2/3 reperfusion better predicted good outcome than did primary AOL 2/3 recanalization. To further analyze the TICI 2 reperfusion end point in hope of identifying an acceptable or optimal stopping point for revascularization, we also categorized subjects as TICI 2A, with <50% MCA distribution reperfusion, or TICI 2B, with recanalization with flow >50% (Tables 1 and 2). TICI 2B/3 perfusion best predicted good outcome statistically (P = .0002), more robustly than TICI 2/3 (P = .0004). There was a trend for TICI 2B superiority to TICI 2A in predicting good outcome (P = .08). AOL 2/3 recanalization (partial or complete recanalization with some flow) also predicted good outcome (P = .027), suggesting that recanalization with some flow predicts good outcome nearly as well as more complete reperfusion. On the basis of these observations, safe revascularization appears to be an appropriate surrogate end point for the IV/IA treatment paradigm. It is not clear that a link between no revascularization and poor outcome is due totally to the no revascularization effect itself. Procedural factors (eg, contrast deposition, saline deposition, micro- and distal emboli, parenchymal hematoma, and even hemorrhagic transformation of injured brain) during prolonged failed revascularization procedures may contribute to the lack of good outcomes observed with this treatment paradigm.
Good outcomes with M2 occlusion were not dependent on revascularization, with 13/17 IMS (76%) I and II isolated M2 subjects achieving good outcome despite incomplete recanalization and reperfusion. This likely relates in part to the much smaller volume of ischemic brain with branch occlusions as compared with occlusions of major proximal arteries.
Of interest, operators scored their revascularization efforts more optimistically than the core lab. Differences between a TICI score of 2 and 3 are of questionable practical significance because these 2 scores are commonly viewed together as significant revascularization and correlate variably with increase in good outcome (Table 2). Nevertheless, it raises a legitimate question of accepting unadjudicated prospective data regarding important end points as a determinant of efficacy. In addition, this observation raises questions regarding revascularization end point terminology, definition, convention, and application. “Good” recanalization (AOL 2/3) in 46/75 (61.3%) and “good” reperfusion (TICI 2/3) in 56/75 (73.6%) of ICA T and M1 occlusions suggest that both measures are legitimate determinants of revascularization, but 12% difference confirms that they are not the same.
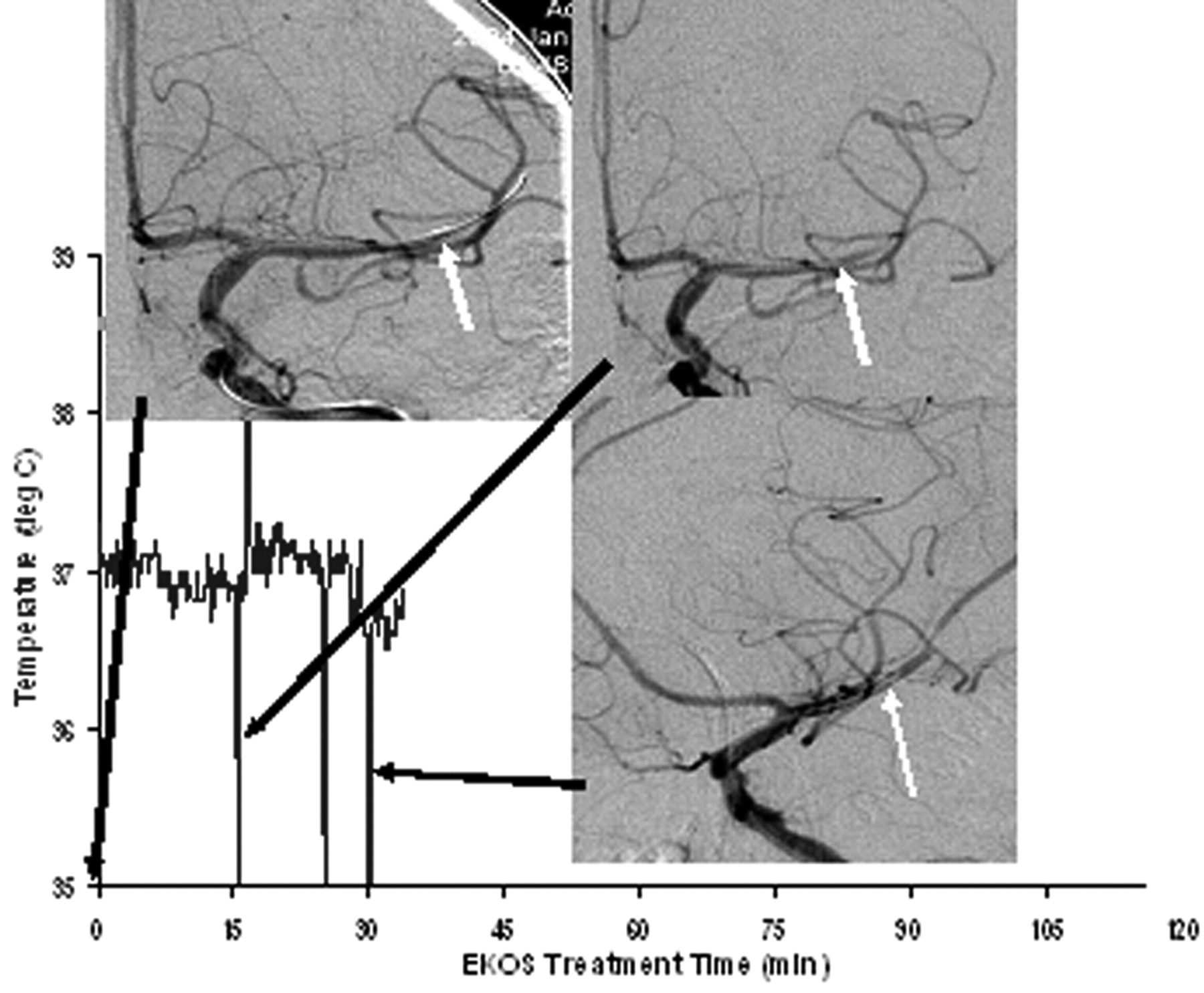
Sonography microcatheter activity measurably increases catheter-tip temperature. Monitoring this effect as a safety measure provided a unique opportunity to examine the effect of recanalization or catheter retraction on catheter-tip temperature. Retrospective correlation of catheter-tip temperature decrease with recanalization suggests that observing tip temperature during a procedure might prospectively allow identification of recanalization between strictly prescribed angiogram intervals and, therefore, might allow the revascularization procedure to be shortened. Retrospective analysis of temperature changes was not complete for all subjects. However, where available, the correlation between a decrease in temperature and recanalization or catheter retraction from the occlusion was quite strong. Whereas some recanalization was identified in 47.6% of subjects and temperature decreases were identified in 41% of subjects, treatment time might be reduced accordingly if real-time changes in temperature decrease might be prospectively identified and acted upon (Fig 3).

Temperature (T) chart correlation to recanalization in M2 occlusion. Upper left: control arteriogram demonstrates EKOS sonography microcatheter placed in the M2 occlusion (white arrow) just before treatment time 0. Upper right: 15-minute control arteriogram demonstrates microcatheter tip retraction into the M1 segment (white arrow). Note the temperature decrease of approximately 0.2°C during the 15-minute time interval, indicating cooling of the catheter by flowing blood. Lower right: oblique 30-minute arteriogram with catheter-tip position (white arrow) proximal to recanalization of the M2 segment, with distal emboli (AOL 3 recanalization, TICI 2 perfusion). Note the temperature drop of approximately 0.4°C during the 15-minute time interval. The downward spikes of T indicate cooling by contrast injection. The spike at 25 minutes was an additional injection to confirm maintenance of catheter position, where no recanalization was yet identified. deg C indicates degrees celsius.
Higher ICH and contrast deposition rates with microcatheter injections suggest that technical factors may be important in clinical outcomes.9 A correlation between MCI and ICH, as well as PH, has also been found in a thrombolysis registry analysis.13 Higher ICH rates with the sonography microcatheter use were confounded by this relationship. Demonstration of rupture points of distal lenticulostriate arteries in several instances negated focal sonography or focal tissue temperature changes as responsible for these ICH cases. No single etiologic mechanism seems responsible for the observed ICH. A multifactorial contribution of rtPA, heparin, contrast deposition, and microcatheter injection pressure/volume is hypothesized.
It is not unreasonable to set a target for good outcomes at 50% or greater in patients with major stroke treated with the IV/IA paradigm applied as rapidly as possible, with limited imaging selection. mRS 0–2 outcomes were achieved in 45% of IMS II overall, compared with 42% of IMS I subjects and with 39% in the treated group of the NINDS study, despite significantly quicker time to IV thrombolytic therapy in the latter. Six AOLs eligible for an IA therapy did not receive it for a variety of reasons. Subjects with M2 occlusions, with baseline NIHSS 11 and 21, were lost to follow-up but were included in the mRS >2 group. It is reasonable to expect that monitoring catheter-tip temperature may accelerate sonography-assisted thrombolysis procedures. Other further advances in revascularization with improved thrombus-removal devices, balloon angioplasty, and/or removable or implantable stents may play a part in further improving interventional outcomes. The IMS III trial, in which 900 subjects will be randomized to either full-dose IV rtPA or to a reduced-dose IV rtPA, plus IA therapy with either the Cordis Neurovascular (Cordis, Miami Lakes, Fla), Neurowave Catheter (EKOS, Bothell, Wash), Merci Retriever Device (Concentric Medical, Mountain View, Calif), or other devices that may be introduced as their approval status becomes defined, will have the opportunity to test this hypothesis.
Conclusions
IMS II provides further evidence that the EKOS Primo sonography microcatheter demonstrates a promising trend toward improved recanalization of the AOL when compared with a standard microcatheter. A correlation between recanalization and reperfusion with outcome is again confirmed. The role of IV/IA revascularization therapy will be further tested against full-dose IV therapy alone in the IMS-III trial.
Footnotes
This study was funded by the National Institute of Neurologic Diseases and Stroke (NINDS #NS39160) and EKOS Corp. EKOS Micro-Infusion Systems were supplied by EKOS Corp, and rtPA was supplied by Genentech Inc.
References
- Received June 20, 2007.
- Accepted after revision September 17, 2007.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Safety, technical and clinical success of the Aperio Hybrid thrombectomy device in acute ischemic stroke, a prospective post-market clinical follow-up study (HYBRID)
- SOFIA Aspiration System as first-line Technique (SOFAST): a prospective, multicenter study to assess the efficacy and safety of the 6 French SOFIA Flow Plus aspiration catheter for endovascular stroke thrombectomy
- Automated assessment of ischemic core on non-contrast computed tomography: a multicenter comparative analysis with CT perfusion
- Comparison of Thrombolysis In Cerebral Infarction (TICI) 2b and TICI 3 reperfusion in endovascular therapy for large ischemic anterior circulation strokes
- Perfusion Collateral Index versus Hypoperfusion Intensity Ratio in Assessment of Collaterals in Patients with Acute Ischemic Stroke
- Mildly elevated INR is associated with worse outcomes following mechanical thrombectomy for acute ischemic stroke
- Predictors of parenchymal hemorrhage after endovascular treatment in acute ischemic stroke: data from ANGEL-ACT Registry
- Unexplained early neurological deterioration after endovascular treatment for acute large vessel occlusion: incidence, predictors, and clinical impact: Data from ANGEL-ACT registry
- Efficacy and safety of bridging thrombolysis initiated before transfer in a drip-and-ship stroke service
- Biomarkers of Technical Success After Embolectomy for Acute Stroke
- Reliability of the Modified TICI Score among Endovascular Neurosurgeons
- Combined use of contact aspiration and the stent retriever technique versus stent retriever alone for recanalization in acute cerebral infarction: the randomized ASTER 2 study protocol
- Electronic Alberta Stroke Program Early CT score change and functional outcome in a drip-and-ship stroke service
- Automated ASPECTS in Acute Ischemic Stroke: A Comparative Analysis with CT Perfusion
- Exploring the relationship between ischemic core volume and clinical outcomes after thrombectomy or thrombolysis
- Influence of occlusion site and baseline ischemic core on outcome in patients with ischemic stroke
- Susceptibility vessel sign on MRI predicts better clinical outcome in patients with anterior circulation acute stroke treated with stent retriever as first-line strategy
- First-in-man experience of the Versi Retriever in acute ischemic stroke
- Thrombectomy using the EmboTrap device: core laboratory-assessed results in 201 consecutive patients in a real-world setting
- Mechanical thrombectomy and rescue therapy for intracranial large artery occlusion with underlying atherosclerosis
- Intravenous Recombinant Tissue-Type Plasminogen Activator: Influence on Outcome in Anterior Circulation Ischemic Stroke Treated by Mechanical Thrombectomy
- Clinical Outcomes of Endovascular Treatment within 24 Hours in Patients with Mild Ischemic Stroke and Perfusion Imaging Selection
- Indications for the Performance of Intracranial Endovascular Neurointerventional Procedures: A Scientific Statement From the American Heart Association
- MR Perfusion to Determine the Status of Collaterals in Patients with Acute Ischemic Stroke: A Look Beyond Time Maps
- Endovascular treatment for AIS with underlying ICAD
- The Impact of Conscious Sedation versus General Anesthesia for Stroke Thrombectomy on the Predictive Value of Collateral Status: A Post Hoc Analysis of the SIESTA Trial
- Multiparametric Magnetic Resonance Imaging for Prediction of Parenchymal Hemorrhage in Acute Ischemic Stroke After Reperfusion Therapy
- Time to redefine success? TICI 3 versus TICI 2b recanalization in middle cerebral artery occlusion treated with thrombectomy
- Impact of Modified TICI 3 versus Modified TICI 2b Reperfusion Score to Predict Good Outcome following Endovascular Therapy
- Endovascular Therapy of M2 Occlusion in IMS III: Role of M2 Segment Definition and Location on Clinical and Revascularization Outcomes
- Emergent mechanical thrombectomy for acute stroke using the Mindframe Capture LP system: initial single-center experience
- A Direct Aspiration, First Pass Technique (ADAPT) versus Stent Retrievers for Acute Stroke Therapy: An Observational Comparative Study
- Impact of Target Arterial Residual Stenosis on Outcome After Endovascular Revascularization
- Imaging Findings Associated with Space-Occupying Edema in Patients with Large Middle Cerebral Artery Infarcts
- TICI and Age: What's the Score?
- Effect of endovascular reperfusion in relation to site of arterial occlusion
- The Revascularization Scales Dilemma: Is It Right to Apply the Treatment in Cerebral Ischemia Scale in Posterior Circulation Stroke?
- Endovascular revascularization results in IMS III: intracranial ICA and M1 occlusions
- Outcome Differences between Intra-Arterial Iso- and Low-Osmolality Iodinated Radiographic Contrast Media in the Interventional Management of Stroke III Trial
- Early Loss of Immediate Reperfusion While Stent Retriever in Place Predicts Successful Final Reperfusion in Acute Ischemic Stroke Patients
- Outcomes of manual aspiration thrombectomy for acute ischemic stroke refractory to stent-based thrombectomy
- M2 occlusions as targets for endovascular therapy: comprehensive analysis of diffusion/perfusion MRI, angiography, and clinical outcomes
- Endovascular treatment for M2 occlusions in the era of stentrievers: a descriptive multicenter experience
- Mechanisms of Unexplained Neurological Deterioration After Intravenous Thrombolysis
- Correlation of AOL recanalization, TIMI reperfusion and TICI reperfusion with infarct growth and clinical outcome
- Unexplained Early Neurological Deterioration After Intravenous Thrombolysis: Incidence, Predictors, and Associated Factors
- Capillary Index Score in the Interventional Management of Stroke Trials I and II
- Acute Ischemic Stroke: Time, Penumbra, and Reperfusion
- Addition of Hyperacute MRI Aids in Patient Selection, Decreasing the Use of Endovascular Stroke Therapy
- Understanding IMS III: old data shed new light on a futile trial
- Thrombus Attenuation Does Not Predict Angiographic Results of Mechanical Thrombectomy with Stent Retrievers
- Prospective, Multicenter, Single-Arm Study of Mechanical Thrombectomy Using Solitaire Flow Restoration in Acute Ischemic Stroke
- What Is Meant by "TICI"?
- Recommendations on Angiographic Revascularization Grading Standards for Acute Ischemic Stroke: A Consensus Statement
- Epistemology, Parachutes, and "Yeah, but" Interventional Stroke Trials
- Advanced modality imaging evaluation in acute ischemic stroke may lead to delayed endovascular reperfusion therapy without improvement in clinical outcomes
- Mechanical Recanalization With Flow Restoration in Acute Ischemic Stroke: The ReFlow (Mechanical Recanalization With Flow Restoration in Acute Ischemic Stroke) Study
- Clarifying Differences Among Thrombolysis in Cerebral Infarction Scale Variants: Is the Artery Half Open or Half Closed?
- Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association
- Comparison of Stent-Retriever Devices versus the Merci Retriever for Endovascular Treatment of Acute Stroke
- Is Intra-Arterial Thrombolysis Beneficial for M2 Occlusions? Subgroup Analysis of the PROACT-II Trial
- The Clinical and Radiographic Importance of Distinguishing Partial from Near-Complete Reperfusion Following Intra-Arterial Stroke Therapy
- Retrospective Multicenter Study of Solitaire FR for Revascularization in the Treatment of Acute Ischemic Stroke
- Periprocedural antithrombotic strategies in acute ischemic stroke interventional therapy
- Elderly Patients Are at Higher Risk for Poor Outcomes After Intra-Arterial Therapy
- A Comparison of 2 Stroke Devices: The New Aperio Clot-Removal Device and the Solitaire AB/FR
- Single-Center Experience of Cerebral Artery Thrombectomy Using the TREVO Device in 60 Patients With Acute Ischemic Stroke
- Infarct Volume Is a Pivotal Biomarker After Intra-Arterial Stroke Therapy
- TICI: If You Are Not Confused, Then You Are Not Paying Attention
- Comparison of the Incidence of Parenchymal Hematoma and Poor Outcome in Patients with Carotid Terminus Occlusion Treated with Intra-Arterial Urokinase Alone or with Combined IV rtPA and Intra-Arterial Urokinase