
We commend Cuvinciuc et al1 on their recent review of nontraumatic cortical subarachnoid hemorrhage (cSAH). While not an uncommon clinical presentation, there is an overall paucity of literature on this subject, with the largest reported series by Kumar et al2 comprising only 29 patients. Cuvinciuc et al1 suggested that cSAH may occur in the setting of high-grade atherosclerotic stenosis of the extracranial cerebral arteries, potentially by a mechanism similar to cSAH in Moyamoya disease (eg, rupture of fragile dilated pial collateral vessels). Recently 3 cases of cSAH have been described in association with bilateral cervical internal carotid artery (ICA) stenosis,3 and 2 further cases, in the setting of acute ICA occlusion during ischemic stroke.4 We describe a rare case of unilateral extracranial ICA stenosis associated with cSAH and discuss the angiographic findings that support the postulated mechanism of fragile pial collateral vessels.
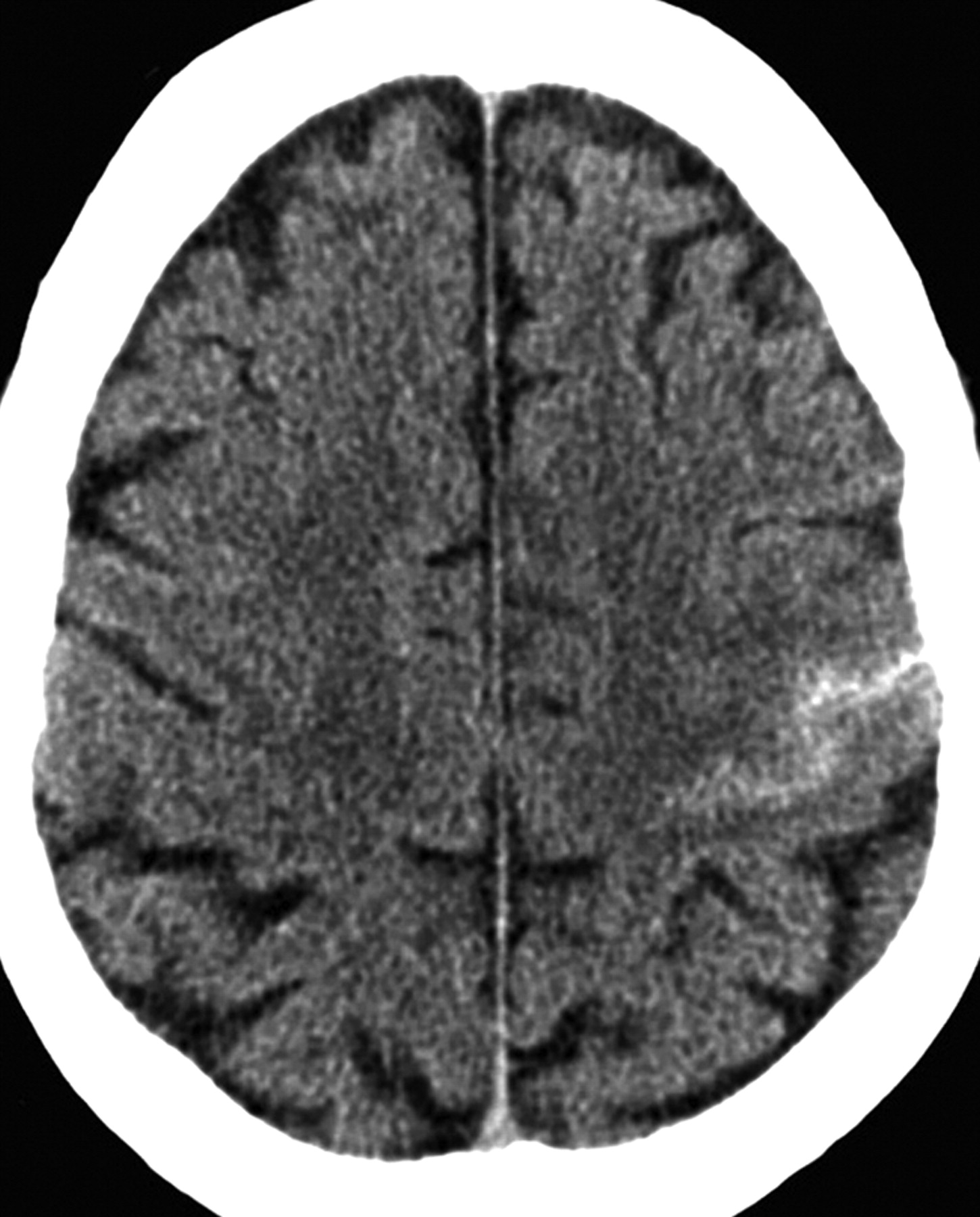
A 70-year-old man experienced a sudden onset of transient aphasia and dysarthria, along with right face and arm numbness at a systolic blood pressure of 200 mm Hg. Noncontrast CT demonstrated isolated cSAH in the left central sulcus (Fig 1), and CT angiography (CTA) revealed an 80% left ICA-origin stenosis without evidence for arterial or venous cause of the cSAH. He continued to have recurrent events in the hospital and was managed for possible transient ischemia or seizure with intravenous anticoagulation and seizure prophylaxis, respectively. MR imaging excluded acute infarction, posterior reversible leukoencephalopathy, amyloid angiopathy, or an underlying mass. There was no clinical evidence of endocarditis, with negative findings on blood cultures and a normal finding on transthoracic echocardiogram. Continuous electroencephalographic monitoring during these episodes did not reveal epileptiform correlation during briefly symptomatic episodes that remained similar to those on the initial presentation. Given the frequency of transient symptoms, carotid endarterectomy (CEA) was considered for the ipsilateral stenosis. However, it was imperative to definitively rule out any vascular lesions responsible for the cSAH, which could worsen from potential hyperperfusion syndrome following CEA. Cerebral angiography was performed and demonstrated no evidence of vasculitis, reversible cerebral vasoconstriction syndrome, mycotic aneurysm, or arteriovenous malformation.

Noncontrast axial CT scan demonstrates subarachnoid hemorrhage in the left central sulcus.
Of note, the 80% left ICA-origin stenosis (Fig 2) resulted in a shift of the angiographic watershed between the left middle cerebral artery (MCA) and posterior cerebral artery (PCA) territories toward the central sulcus (Fig 3). Most importantly, there was minimal collateral support via the circle of Willis. A hypoplastic precommunicating right anterior cerebral artery (ACA) segment provided minimal flow across the anterior communicating artery. No left posterior communicating artery was discernible. Subsequently, the patient underwent emergent ipsilateral CEA with resolution of his symptoms.

Left common carotid artery angiogram demonstrated 80% ICA stenosis.
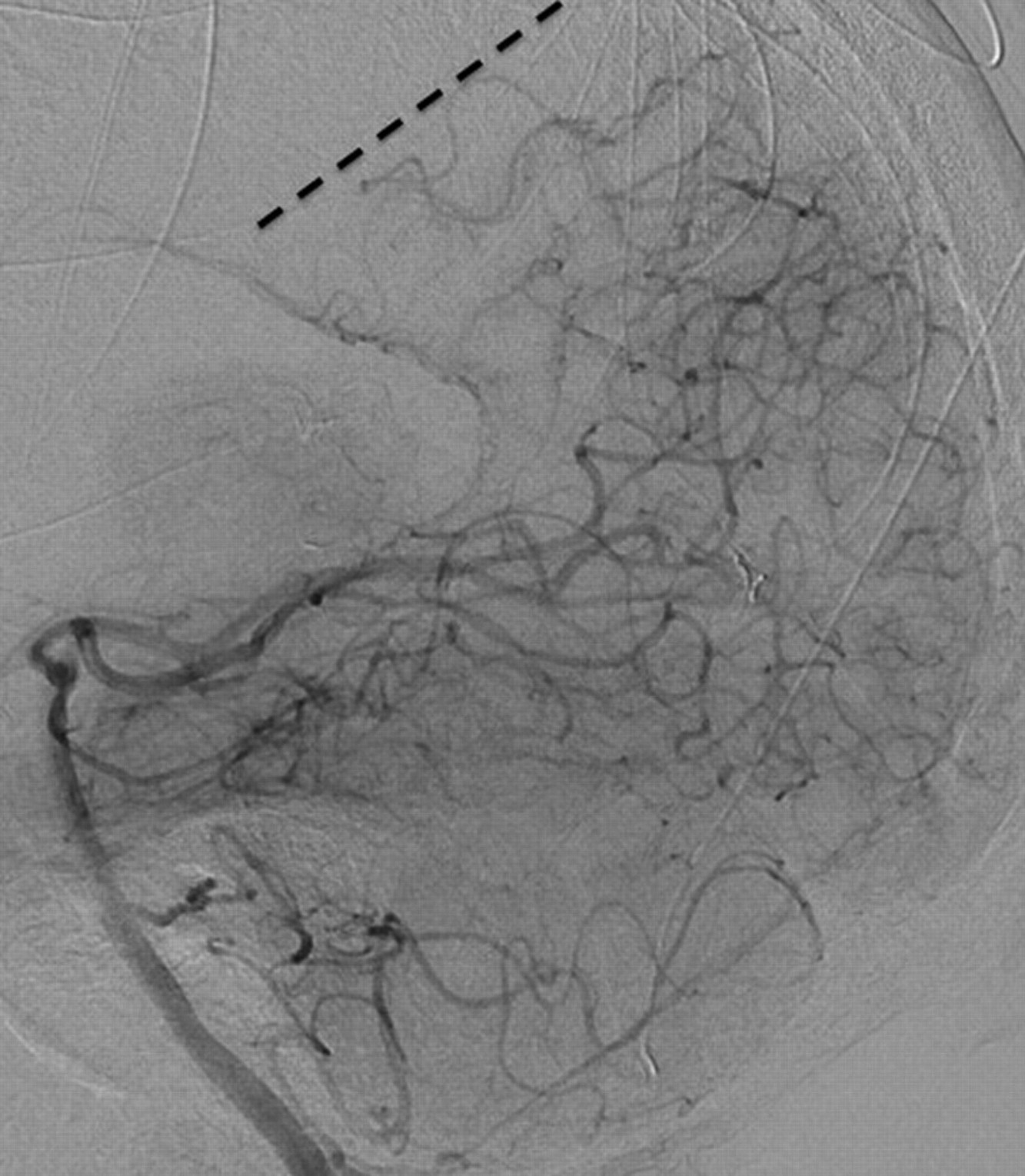
Left vertebral artery angiogram reveals a shift of the left PCA/MCA watershed (dotted line) toward the central sulcus. Perisplenial PCA collaterals also retrogradely fill the pericallosal ACA territory, indicating the severe left anterior circulation hemodynamic compromise.
Isolated cSAH in the present case, the 3 cases with bilateral ICA stenosis described by Kleinig et al,3 and the 2 cases of acute ICA occlusion described by Geraldes et al,4 all occurred on the symptomatic side or the side with the more severe anatomic narrowing (stenosis or occlusion). All 6 patients were acutely symptomatic suggesting that cSAH may derive from an acute alteration in hemodynamics (eg, plaque rupture and further atherothrombotic narrowing or acute hypertension). We propose that this hemodynamic stress may damage already maximally dilated pial collateral vasculature and produce cSAH.
This idea is supported by our angiographic findings, in which the subarachnoid hemorrhage colocalized to the watershed region between the MCA and PCA territories. In the setting of severe ICA stenosis or occlusion, it is the MCA-PCA watershed rather than the MCA-ACA watershed that may be particularly prone to this phenomenon, because the ipsilateral ACA and MCA have reduced perfusion pressure and are less able to respond to acute hemodynamic failure, particularly in the absence of sufficient blood flow via the anterior or posterior communicating arteries as in this case. On the other hand, the normally perfused PCA territory is able to mount a compensatory increase in perfusion pressure, which may rupture fragile pial collateral vessels in the watershed. Consistent with this idea, 4 of the 6 described cases occurred in a perirolandic location, at the watershed between the MCA and PCA territories.
The rarity of cSAH in the setting of unilateral extracranial ICA stenosis may reflect the collateral pathways across the circle of Willis that are usually present. As in our case, the absence of adequate collaterals may provide a clue to this mechanism of cSAH. Contrary to Cuvinciuc et al,1 who advocated only brain vascular imaging, CTA evaluation of cSAH must include the cervical vasculature, lest a high-risk yet treatable lesion is missed.
References
- Copyright © American Society of Neuroradiology





{kind=link}
{kind=link}
{kind=link}