
Article Figures & Data
Figures
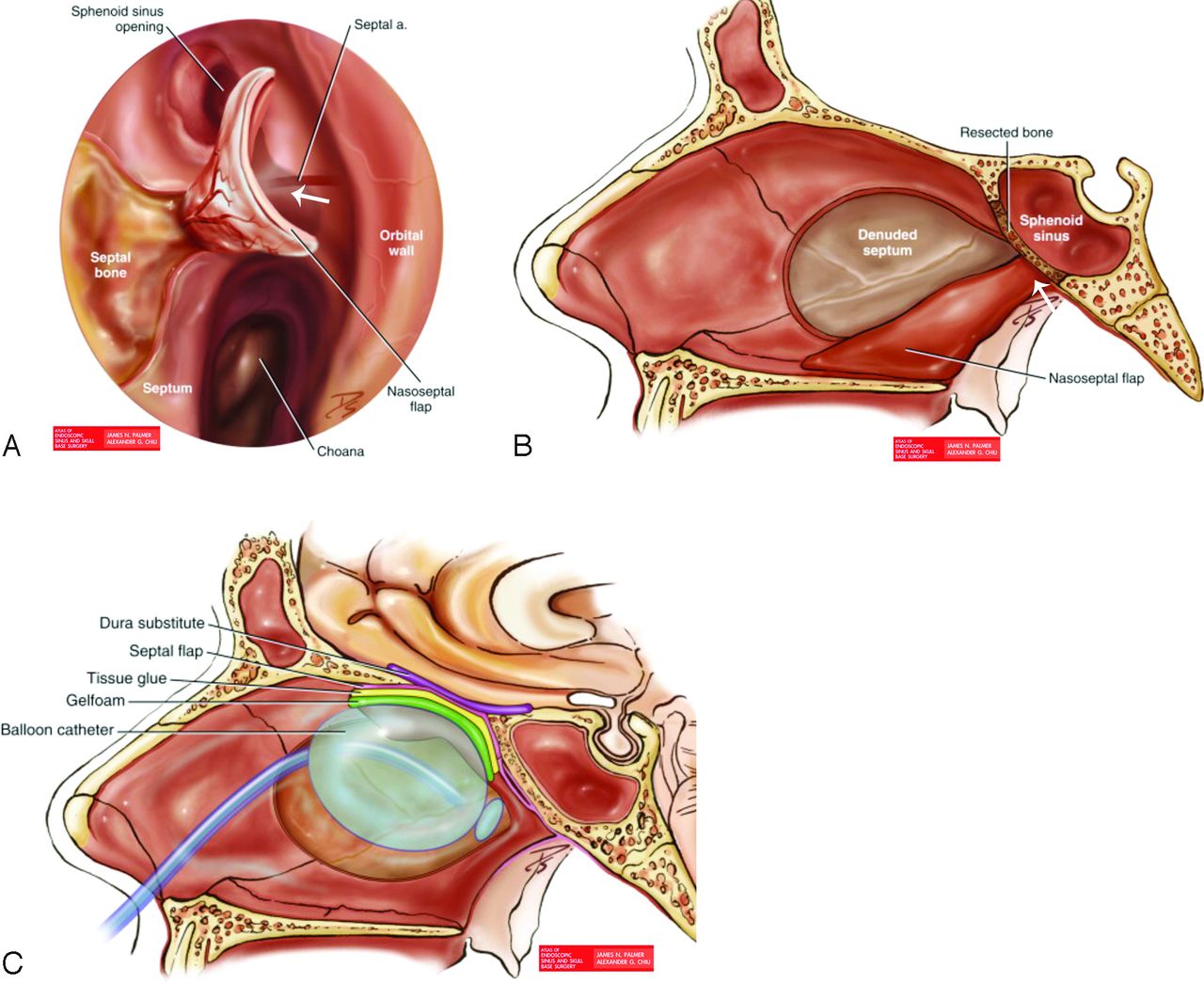
- Fig 1.
Multilayer ESBR using NSF. A, Endoscopic coronal view of the nasal cavity illustrates harvesting of the NSF from the nasal septum with the preserved septal artery vascular pedicle (arrow) arising from the sphenopalatine artery. B, Sagittal view of the harvested NSF shows that the flap is anchored by its pedicle (arrow), leading toward the ipsilateral sphenopalatine foramen. C, Sagittal drawing of the ESBR shows inlay dura substitute (such as collagen matrix, fascia lata) and onlay mucosal closure with an NSF (labeled as a septal flap). Autologous fat graft may be placed above the dura substitute layer to fill the intracranial resection bed. The NSF is held in place by biologic tissue glue. Reconstruction is bolstered with nasal sponges and/or a balloon catheter to prevent dislodging during the immediate postoperative period. Reprinted with permission from Atlas of Endoscopic Sinus and Skull Base Surgery. Palmer JN, Chiu AG. Copyright Elsevier, 2013.12
- Fig 2.
Graft shows the percentage of follow-up MR imaging studies performed before or without adjuvant treatment (gray bar) and after adjuvant treatment (black bar) versus postoperative time intervals.
- Fig 3.
A 47-year-old man with normal evolution of the ESBR after EEA gross total resection and adjuvant radiation of a clival chordoma. A, Preoperative sagittal enhanced T1WI shows tumor (T) eroding the upper clivus and compressing the ventral pons (arrow). B, Immediate postoperative sagittal enhanced fat-saturated T1WI shows an enhancing C-shaped NSF covering the clival defect (arrow), abutting the nonenhancing fascia lata (arrowhead) and clivectomy fat packing (F). Nonenhancing Gelfoam (Phadia, Uppsala, Sweden) and blood (G), enhancing pituitary (P). C, Five-month follow-up sagittal enhanced fat-saturated T1WI shows a solidly enhancing slightly thinner NSF and retraction of the reconstruction with the enhancing fascia lata (arrowhead) inseparable from granulation tissue/resorbing fat (F). Marked nodularity along the anterior and inferior portions of the NSF relates to retraction and incorporation of the flap into the newly enhancing free grafts and granulation tissues.
- Fig 4.
A 58-year-old woman status post transcribriform resection and adjuvant chemoradiation for sinonasal neuroendocrine carcinoma and NSF misinterpreted as a neoplasm. A, Preoperative coronal enhanced fat-saturated T1WI shows enhancing tumor (T) with intracranial extension. B and C, Immediate postoperative coronal and axial enhanced T1WI shows fat (F) in the subfrontal bed, nonenhancing T1-hypointense fascia lata (arrowheads) at the bone defect, and mucosal closure with enhancing NSF (arrows). D, Immediate postoperative axial T2WI shows T2-hyperintense fascia lata (arrowhead) and T2-isointense NSF (arrow). E, Three-month follow-up coronal enhanced T1WI shows normal evolution of the ESBR with retraction to the defect; significant resorption of intracranial fat graft (F); and a thin enhancing fascia lata (arrowhead) above the solidly enhancing NSF (arrows), mistaken for neoplasm in the official report. F and G, Sixteen-month follow-up (3 months after completion of chemoradiation) coronal fat-saturated enhanced T1WI and T2WI show little change of the enhancing fascia lata (arrowheads) and solidly enhancing T2-isointense NSF (arrows).
- Fig 5.
A 52-year-old man following transplanum resection and chemoradiation for sinonasal undifferentiated carcinoma has abnormal evolution of the ESBR, consistent with recurrent tumor. A, Preoperative coronal fat-saturated T2WI shows tumor (T) invading the planum sphenoidale and right optic canal (arrowhead). S indicates sinus secretions. B and C, Immediate postoperative coronal and axial enhanced fat-saturated T1WIs show an enhancing NSF (arrows) at the planum-sphenoidale defect with a right-sided vascular pedicle (asterisk). The thin nonenhancing collagen matrix dural inlay above the NSF is indiscernible. The nasal cavity is packed with sponge. D and E, Three-month follow-up coronal fat-saturated T2WI and enhanced T1WI show retraction of the enhancing NSF (arrows) into the skull base defect with a stable location of the right pedicle seen on the axial image (not shown) and mildly enhancing T2-hypointense dural graft/granulation (bow arrows). Nodular tumor recurrence at the edge of the reconstruction in the left sphenoid sinus (T) and along the supraorbital dura (arrowheads) has signal intensity and mild enhancement similar to that in preoperative tumor and different from that in the adjacent reconstructive layers.




Tables
Pathologies (No. of Patients and Average Tumor Size) Skull Base Defects ESBR Tissues (No. of Patients) Length of MRI Follow-Up (mo) Adjuvant Therapy (No. of Patients) Esthesioneuroblastoma (n = 6; 2.5 cm) ASB F, FL, NSF, FM (n = 1) 9–32 Radiation (n = 4), D, NSF (n = 3) Chemoradiation (n = 2) D, NSF, FM (n = 2) Sinonasal endocrine carcinoma (n = 1; 4.0 cm) ASB F, FL, NSF, FM (n = 1) 16 Chemoradiation (n = 1) Sinonasal undifferentiated carcinoma (n = 1; 2.2 cm) ASB D, NSF (n = 1) 3 Chemoradiation (n = 1) Chondrosarcoma (n = 1; 2.5 cm) Clivus D, NSF (n = 1) 21 Radiation (n = 1) Chordoma (n = 3; 2.0 cm) Clivus NSF (n = 2) 9–21 Radiation (n = 2) F, FL, NSF (n = 1) Meningioma (n = 4; 2.2 cm) ASB D, NSF (n = 1) 3–41 Radiation (n = 1) CSB F, FL, NSF (n = 2) Clivus F, FL, NSF (n = 1) Craniopharyngioma (n = 1; 3.5 cm) CSB F, FL, NSF (n = 1) 6 Pituicytoma (n = 1; 3.1 cm) CSB F, FL, NSF (n = 1) 13 Radiation (n = 1) Pituitary macroadenoma (n = 4; 3.4 cm) CSB NSF (n = 1) 6–27 Radiation (n = 1) F, NSF (n = 1) FL, NSF (n = 1) F, FL, NSF (n = 1) Note:—ASB indicates cribriform plates, crista galli, and/or ethmoid fovealis; CSB, planum sphenoidale, tuberculum sella, sella, and/or dorsum sella; D, collagen matrix dural graft; F, intracranial fat; FL, fascia lata; FM, free mucosa.
- Table 2:
MR imaging evolution of ESBR from the immediate postoperative period to stability on follow-up
Immediate Postoperative MRI Follow-Up MRI at 2–6 Months NSF Solid enhancement, T2-isointensity to brain (mostly similar to gray matter), distinctive C shape and vascular pedicle configurations Persistent solid enhancement, persistent T2-isointensity to brain (mostly similar to gray matter), thickness reduction by 20%–30%, average thickness of 4.5 mm Less well-defined C shape and vascular pedicle configurations, unchanged flap location Fascia lata Nonenhancing, variable T2 signal intensity Mildly enhancing, increasing T2-hypointensity, thickness reduction by ≥50%, average thickness of 3.5 mm Collagen matrix dural graft Nonenhancing, nonvisible to ≤2 mm Inseparable from enhancing granulation tissue at the reconstruction site, nonvisible to ≤2 mm Fat graft Fat signal intensity fills intracranial surgical bed Fat signal intensity in retracted intracranial surgical bed, progressive resorption with volume reduction by ≥50%





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}