
Abstract
SUMMARY: Vessel wall MR imaging is a useful tool for the evaluation of intracranial atherosclerotic disease. Enhancement can be particularly instructive. This study investigated the impact of the duration between contrast administration and image acquisition. The cohort with the longest duration had the greatest increase in signal intensity change. When using vessel wall MR imaging to assess intracranial atherosclerotic disease, protocols should be designed to maximize the duration between contrast administration and image acquisition to best demonstrate enhancement.
ABBREVIATIONS:
- DANTE
- delay alternating with nutation for tailored excitation
- vwMRI
- vessel wall MR imaging
- ICAD
- intracranial atherosclerotic disease
- SPACE
- sampling perfection with application-optimized contrasts by using different flip angle evolutions
Development of vessel wall MR imaging (vwMRI) protocols has improved the evaluation of intracranial atherosclerotic disease (ICAD) by providing direct visualization of the vessel wall and the plaque itself.1⇓⇓⇓⇓–6 In the evaluation of ICAD with vwMRI, an important diagnostic finding is plaque enhancement, a characteristic widely believed to reflect inflammation.7,8 Inconsistencies in acquisition parameters and image interpretation have limited progress in the development of these promising MR imaging techniques.6,7,9⇓⇓–12
Reproducible quantitative interpretation techniques could help overcome these limitations, particularly with respect to enhancement, but standardization of acquisition parameters is also needed.6 Duration between contrast administration and image acquisition affects the degree of measured enhancement in other pathologies.13,14 This study examined the impact of time intervals on enhancement measured in ICAD plaques and reference structures.
Materials and Methods
Following an institutional review board–approved protocol, retrospective analysis was performed of patients undergoing vwMRI for the evaluation of ischemic stroke at a major academic medical center. In this protocol, vwMRI studies are performed for patients with confirmed new infarcts suspected of being due to ICAD or not attributed to another etiology. All patients in this study were evaluated with vwMRI within 14 days of the infarct.
Studies were performed with dedicated head coils on Prisma, Trio, or Verio 3T MR imaging scanners (Siemens, Erlangen, Germany). Two blinded neuroradiologists assessed the arterial tree upstream from the new infarct. The reviewers were notified about which artery to assess by the vascular neurologist, who adjudicated the stroke parent artery status according to diffusion-weighted imaging lesions within the vascular territory of a major artery with ICAD. Reviewers were blinded to clinical data and other MR imaging findings, most notably DWI. Reviewers noted the lesion that had most likely caused the downstream infarction. The culprit lesions were determined by each reviewer and confirmed between them to be the same lesion for each patient. Each reviewer was blinded to measurements made by the other reviewer. Patients in whom multiple ICAD lesions in the same vascular bed could be considered culprit were excluded to avoid bias.
After we confirmed the consensus on the culprit lesion, maximum signal intensity values were recorded on 3D T1-weighted sampling perfection with application-optimized contrasts by using different flip angle evolutions (SPACE; Siemens) with delay alternating with nutation for tailored excitation (DANTE) flow suppression pre- and postcontrast.5 Patients were given gadobenate dimeglumine (MultiHance; Bracco Diagnostics, Princeton, New Jersey) at a dose of 0.2 mL/kg (0.1 mmol/kg). Additionally, structures known to normally enhance were included, including the low infundibulum, defined as the lowest segment distinguishable from the pituitary gland on axial images; muscle, chosen within the temporalis muscle medial to its midbelly fibrous band; cavernous sinus, measuring a segment clearly representing only blood; and the choroid plexus.6,15 Three data points were measured for each site assessed, and the mean was calculated.
Times were tabulated for contrast administration and acquisition of postcontrast images. To exclude outlier data during early development of the vwMRI protocol that could introduce bias, we excluded studies with >40 minutes between contrast injection and T1 DANTE acquisition. Correlation coefficients were calculated among variables as well as P values to assess the significance of associations. For further analysis, the cohort was divided into 3 different time intervals from contrast injection to T1 DANTE: 0–20 minutes, 20–30 minutes, and 30–40 minutes. Comparison was made of the variance of pre- to postcontrast measurements across these time periods using the Levene test of the equality of variance. All analyses were performed in STATA 15.1 (StataCorp, College Station, Texas).
Results
Studies from 54 patients were evaluated. Thirty-five patients met all the inclusion criteria (10 studies in the 0- to 20-minute group, 13 at 20–30 minutes, and 12 at 30–40 minutes). Representative studies from each time group are provided in Fig 1. The mean ± SD time from contrast injection to T1 DANTE was 24.5 ± 10.4 minutes (range, 6.9–39.5 minutes). In culprit plaques, the percentage increase in signal intensity from pre- to postcontrast was 110.2% ± 54.7%, which was significantly associated with the time from contrast injection to T1 DANTE (Fig 2, P = .029). For the reference structures, there was no association between the time from contrast injection to T1 DANTE and the change in signal intensity between pre- and postcontrast (Table). Creating a ratio of percentages in increased T1 signals of plaque over the lower infundibulum demonstrates a stronger correlation with timing than plaque alone (r2 = 0.410, P = .016). If one introduces a pituitary signal increase into the model for plaque as a covariate, plaque maintains the association with time (P < .05). Additionally, there is no direct association between the plaque and infundibulum changes (r2 = −0.103, P = .561).

Representative images of vwMRI studies of symptomatic ICAD lesions (arrows) in each of the 3 timing cohorts, <20 minutes (A and B), 20–30 minutes (C and D), and 30–40 minutes (E and F). For each study, pre- (A, C, and E) and postcontrast (B, D, F) images are shown of lesions in the right V4 segment (A and B), distal left M1 segment (E and F).
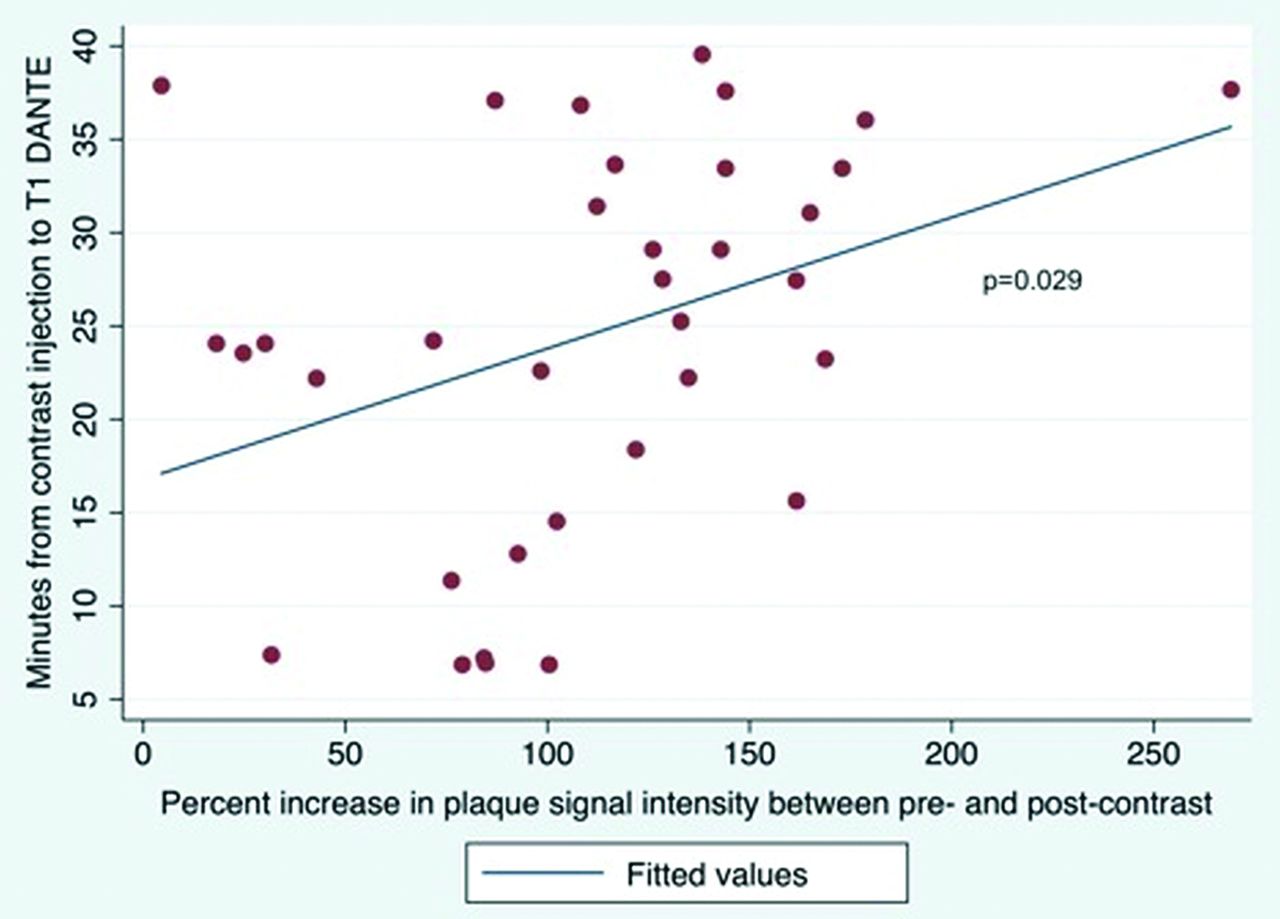
Linear regression between the minutes from contrast injection to T1 DANTE and the percentage increase in plaque signal intensity between pre- and postcontrast.
Correlation between time from contrast injection to T1 DANTE and measurements of change in signal intensity between pre- and postcontrast
Discussion
Evaluation of ICAD can be aided by vwMRI studies.1⇓–3,6,8 While these techniques have proved useful, broad clinical use is impeded by heterogeneous acquisition and interpretation methods. Standardized methodologies can mitigate such issues, particularly when quantitative analyses are used.6 Enhancement of ICAD plaques is a particularly instructive feature, and this characteristic, in particular, is prone to variability.6⇓–8 These results confirm our early clinical observation that lesion enhancement was accentuated by increased duration between contrast administration and acquisition of postcontrast DANTE images. The association between time and T1 signal changes is independent of changes in the pituitary gland. Standardizing plaque signal change to change measured in the pituitary gland is even more dependent on time from contrast administration. In response to these findings, we have standardized a vwMRI protocol that maximizes this duration within the accepted temporal confines for these studies by acquiring sequences not impacted by contrast (T2, FLAIR) after contrast administration and before postcontrast DANTE imaging.
This study has several limitations that warrant mention. Visualized enhancement may reflect variables other than timing such as differences in plaques, patient age or sex, or other factors. Additionally, elapsed time after contrast may be confounded, which cannot be determined without imaging the same person multiple times or doing a dynamic study. Such factors can be assessed in future investigations. Despite these limitations, it appears that future studies using vwMRI might benefit from defined time intervals between contrast administration and postcontrast T1 imaging.
Footnotes
This study was funded, in part, by National Institutes of Health grants NIH S10OD018482, NIH R01HL127582, NIH/NINDS K23NS105924, and the American Heart Association (19TPA34910194 and 17SDG33460420).
Disclosures: J. Scott McNally—RELATED: Grant: American Heart Association, Comments: American Heart Association Scientist Development Grant (17SDG33460420) supports a portion of my research time.* *Money paid to the institution.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received May 20, 2019.
- Accepted after revision July 17, 2019.
- © 2019 by American Journal of Neuroradiology





{kind=link}
{kind=link}