
Abstract
BACKGROUND AND PURPOSE: A basilar artery intraluminal septation is an exceedingly rarely reported, presumed congenital abnormality. In our clinical practice, we have occasionally noticed an intraluminal band within the inferior aspect of the basilar artery on CTA. Furthermore, we have noticed, at times, the presence of a punctate calcification associated with this finding. We hypothesized that what previous studies have called “basilar septations” in fact represent miniature and thus aberrant basilar fenestrations.
MATERIALS AND METHODS: We retrospectively reviewed CTA studies obtained between January 1, 2017, and August 31, 2019. Identified intraluminal basilar abnormalities were classified as either basilar septations or basilar fenestrations. Association with other posterior circulation abnormalities was documented.
RESULTS: A total of 3509 studies were examined. A basilar intraluminal abnormality was evident in 80 patients (2.3%). Of these 80 patients, 59 were classified as having a basilar fenestration (1.7%) and 21 were classified as having basilar septations (0.6%). Associated calcification was evident in 3 of the basilar fenestration cases and 13 of the basilar septation cases.
CONCLUSIONS: Basilar septations most likely represent and should be referred to as aberrant basilar fenestrations. They should be interpreted as benign congenital incidental findings and should not be misinterpreted as focal dissections or arterial webs. Important variations in the morphology of aberrant basilar fenestrations exist, including areas of thinning, varying thickness, and nodularity. Therefore, when associated with calcification or nodularity, aberrant basilar fenestrations should not be confused with focal intraluminal thrombi or calcified or noncalcified emboli.
ABBREVIATIONS:
- aBF
- aberrant basilar fenestration
- FMD
- fibromuscular dysplasia
The most common congenital finding of the basilar artery is a fenestration (prevalence range, 0.28%–5.26% in postmortem series).1⇓⇓-4 Other congenital intraluminal abnormalities of the basilar artery have been rarely reported in the literature. In particular, case reports of intraluminal basilar septations and basilar webs are exceedingly rare.5,6 Although infrequently seen, these variations can be detected on routine vascular imaging.
Arterial fenestrations are segmental duplications of the vessel lumen into 2 endothelial cell-lined ducts that share a common origin and reconnect distally.7,8,9,10,11 Fenestrations result from an incomplete fusion in the early embryonic stage, yielding a developmental abnormality that can range in length from 1 mm to a near-complete doubling of the artery.10 A large fenestration appears like a “window” perforating the vessel, whereas a very small fenestration can look like a dimple in the vessel wall.10 Prevalence varies greatly between postmortem and imaging reports, with a reported angiographic prevalence of 1.1%.13 Additionally, prevalence based on 3D reconstruction of CT and MR angiography has been reported at 13%.11,12 Although relationships between fenestration and neurovascular pathology are not well-defined, associations with aneurysms and ischemic stroke have been observed.10,12⇓-14
A basilar intraluminal septation is an exceedingly rarely reported, presumed congenital abnormality. To our knowledge, only 2 published articles describe this entity. These articles describe them as intraluminal bands within the vessel.6,15 The most frequent location for this variation is in close proximity to the junction of the vertebral arteries.6,15 The initial study describing this finding was published by Davy,15 in 1839, in which he described 17 cases in 98 postmortem examinations (17.35%). The most recent article is a single cadaveric study that found 1 septation in a sample of 150 cadavers (0.67%).6 In this case, the septation measured 3 mm long and 1.5 mm wide.6 Tubbs et al6 have suggested that these septations may represent a form fruste of basilar fenestrations and may be misinterpreted as dissections or thrombus.16 A similar finding has been described in a few imaging case reports as a presumed basilar web when associated with thrombosis and infarction.5 However, only correlational evidence was reported. Of note, these findings were not present at a branching point and did not mirror the ledge-like imaging findings of a carotid web.17,18 In fact, the imaging findings appear to be identical in location and morphology to the aforementioned basilar septations.
In our clinical practice, we have occasionally noticed an intraluminal band within the inferior aspect of the basilar artery on routine CTA. Because there is no theoretic inferior limit to the size of a basilar fenestration, we hypothesized that what previous studies have called “basilar septations” or “basilar webs” in fact represent miniature and thus aberrant basilar fenestrations (aBFs).
MATERIALS AND METHODS
In an institutional review board–approved study, we retrospectively reviewed all diagnostic-quality head and neck CTA studies performed between January 1, 2017, and August 31, 2019. Any studies with serious motion at the level of the basilar artery were excluded from the analysis. A total of 3509 diagnostic-quality head and neck CTAs were identified within the time period of analysis. Scanning was performed on 64-, 128-, and 256-section multidetector row CT scanners (VCT 64, GE Healthcare; Definition 64, Siemens; Ingenuity 128, IQon 128, and ICT 256, Philips Healthcare). The standard CTA protocol was intravenous injection of 80 mL of nonionic contrast, with arterial phase imaging performed from the aortic arch to the calvarial apex with an axial CTA source image thickness of 0.625 mm. The arterial vertebrobasilar system was inspected for the presence of any clearly defined, intraluminal abnormality on axial CTA source images. Any other CTA or MRA studies performed previously or subsequently were used to confirm the finding and assess interval changes. Any DSA studies with images of the posterior circulation were also examined.
Identified basilar intraluminal abnormalities were classified as either basilar septations or basilar fenestrations. Basilar fenestrations were defined as areas of incomplete fusion of the basilar artery with a visible extravascular lumen (ie, window) or puckering, indentation, or dimple of the vessel wall. Basilar septations were defined as an intraluminal linear hypodensity without a visible window, puckering, indentation, or dimple. In identified cases, the location within the vessel (inferior, middle, or superior one-third) was documented.
Basilar fenestrations and septations were further classified by appearance. Basilar fenestrations were classified as window-, hourglass-, or funnel-shaped. Basilar septations were classified as either linear if a smooth intraluminal band was evident or nodular if any areas of bulging or protuberance existed along the intraluminal band. Any associated morphologic findings such as calcification were also documented.
Measurements of the intraluminal finding were obtained using axial CTA. In the case of a fenestration, the measurement was obtained from the point of maximum vessel wall aperture. Alternatively, septations were measured at the point of maximum width. A measurement of ≤0.6 mm (CT scanner section thickness) was given for septations whose thickness was at the limit of study resolution.
To ascertain whether any of these findings were associated with any other posterior circulation abnormalities, we also documented the presence of an aneurysm, ischemic infarct, parenchymal hemorrhage, severe atherosclerotic stenosis or occlusion, dissection, and vascular webs. The data obtained from our retrospective review were analyzed using descriptive statistics, and 95% confidence intervals are provided for the estimated proportions of patients with abnormal anatomy. Abnormal anatomy is further divided into basilar fenestrations and basilar septations.
RESULTS
A total of 3509 patients (1727 men [49.2%] and 1782 women [50.8%]; age range, 18–102 years; mean age, 64 years) had a diagnostic-quality head and neck CTA study performed during the designated time period. A normal vertebrobasilar system was seen in 3429 of these patients (3429/3509 [97.7%], 1690 men [49.3%] and 1739 women [50.7%]; age range, 18–102 years; mean age, 64 years). A detectable basilar artery intraluminal abnormality was evident in the remaining 80 patients (80/3509 [2.3%]; 95% CI, 1.79%–2.77%; 43 men and 37 women; age range, 36–94 years; mean age, 67 years). Of these 80 cases, 59 were classified as a basilar fenestration (59/3509 [1.7%]; 95% CI, 1.26%–2.11%; 33 men [55.9%] and 26 women [44.1%]; age range, 38–94 years; mean age, 67 years) and 21 were classified as a basilar septation (21/3509 [0.6%]; 95% CI, 0.34%–0.85%; 10 men [47.6%]; 11 women [52.4%]; age range, 36–92; mean age, 68 years). No cases with >1 fenestration or septation were found.
Of the 59 cases classified as a basilar fenestration, 27 had window-shaped fenestrations, 30 had hourglass-shaped fenestrations, and 2 had funnel-shaped fenestrations (Fig 1). The mean apertures of these 3 variations were 3.9 mm (range, 1.5–15 mm), 1.2 mm (range, 0.8–2.0 mm), and 1.4 mm (range, 0.9–1.9 mm), respectively. All the small basilar fenestrations without a window were associated with visible puckering/indentation of the vessel wall. Of the patients with basilar fenestrations, 53 were located in the inferior third (53/59, 89.8%); 4 in the middle third (4/59, 6.8%); and 2 in the superior third of the vessel (2/59, 3.4%). Of the 59 basilar fenestration cases, 17 had at least 1 other CTA or MRA with the imaging findings evident and unchanged on all studies. Of these 17 cases, 3 also had DSA and VasoCT (Philips Healthcare; conebeam CT with contrast) images of the posterior circulation confirming the basilar fenestration, also well-visualized with this technique.
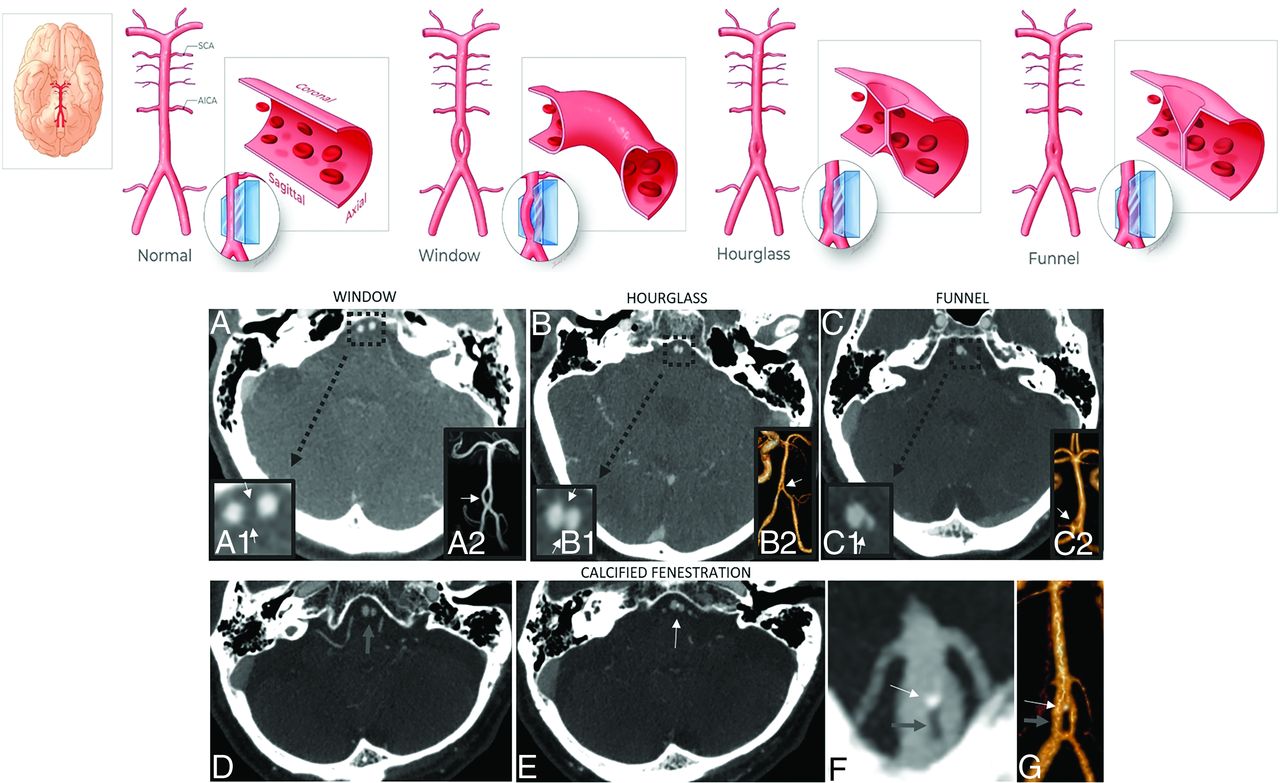
Basilar fenestrations. I) Classification. Basilar fenestrations were classified as either window-, hourglass-, or funnel-shaped (upper row illustrations: printed with permission from Insil Choi, copyright 2020). Axial CTA images (A–C) and magnified axial CTA images focusing on the basilar artery fenestration (A1, B1, C1) and coronal 3D reconstructions of the posterior circulation (A2, B2, C2) in various patients depict different morphologies of basilar fenestration apertures. II) Fenestration with calcification. Associated calcification is evident in 3 of the basilar fenestration cases (3/59; 5.1%). Sequential axial CTA images in one of these patients demonstrate a fenestration (D, wide gray arrow) with a small nodular calcification along its superior aspect (E, thin white arrow), a finding better evident on coronal MIP (F) and 3D reconstruction (G) of the basilar artery (fenestration highlighted by a thick gray arrow, and the nodular calcification, by the thin white arrow).
Of the 21 septations, 9 had at least 1 other CTA or MRA with the imaging findings evident and unchanged on all studies (Fig 2). Of these 9 cases, 3 also had DSA images of the posterior circulation, with the septations not clearly evident on angiographic images. When we compared the saliency of the septations on CTA versus MRA, the septation was more evident on CTA than on MRA in 1 patient, equally evident on CTA and MRA in 2 patients, and better evident on MRA than CTA in 2 patients. Of note, the saliency of the findings appeared primarily related to the quality of the imaging study, including motion, artifacts, and bolus timing rather than superiority of one technique over the other. Of the 21 cases classified as basilar septations, 12 were linear (Fig 2) and 9 were nodular (Fig 3). The mean width of these 2 variations was 0.63 mm (range, ≤0.6–0.7 mm) and 0.98 mm (range, 0.7–1.4 mm), respectively. None of the patients with basilar septations were seen to have puckering/indentation of the vessel wall. Of the patients with basilar septations, 14 septations were located in the inferior third (14/21, 66.7%); 5, in the middle third (5/21, 23.8%); and 2, in the superior third (2/21, 9.5%) of the vessel.

Basilar septations. I) Lack of interval changes: a basilar septation (upper row illustration, printed with permission from Insil Choi, copyright 2020) is identified in 21 patients (0.6%). A typical basilar septation can be seen on sequential axial CTA images at initial presentation in case 1 (A–C). Note the clearly defined linear hypodensity without a visible window or clear evidence of puckering or indentation of the vessel wall (A–C, arrows). Sequential axial CTA images obtained 1 year later (D–F) clearly show the absence of interval changes. Of the small subset of patients with >1 CTA, there is no evidence of interval changes at any time point. II) Evident on CTA and MRA: axial CTA image in case 2 (G1) demonstrates a septation along the ventral aspect of the basilar artery (white arrow). Note that the septation is thick anteriorly but markedly thins posteriorly. This finding is corroborated on axial MRA images with the thin posterior aspect slightly more evident (G2, white arrows). Axial CTA image in a different patient (H1) demonstrates a markedly subtle septation perhaps best visualized along the central lumen of the basilar artery (H1 magnified insert, arrowheads). This finding is again corroborated and much better visualized on a high-quality axial MRA (H2, white arrowhead). Although MRA was available in only a small subset of the patients, the presence of a septation was corroborated on this technique. Of note, depending on the quality of the CTA or MRA acquisition, the septations were, at times, better defined on CTA instead.

Basilar septations with nodularity without and with calcification (upper row illustrations, printed with permission from Insil Choi, copyright 2020). I) Several basilar septation cases exhibited areas of nodularity. Three representative cases are shown above. Axial CTA in the first case (A) demonstrates subtle nodularity along the midpoint of the basilar septation (A magnified insert, white arrow). Axial CTA image in a different patient (B) shows calcification associated with central nodularity (B magnified insert, white arrow). Axial CTA in a third patient (C2) demonstrates a prominent but only partially calcified nodular septation. The calcification is clearly evident on an axial noncontrast CT image (C1, arrow). The partially calcified prominent nodularity associated with the septation is well-demarcated on axial CTA (C2a magnified insert, white arrow) and coronal MIP (C2b, white arrow) images. II) Calcified basilar septations: focal calcification associated with basilar septations is seen in 13 cases (13/21, 61.9%). Axial CTA images in 6 different patients (D–I) demonstrate different patterns of calcification with some exhibiting a more linear pattern (D–F, arrows) and others exhibiting a more nodular pattern of calcification (G–I, arrows). Note the prominent nodular calcification occupying a large portion of the basilar lumen in case I.
Calcification was associated with intraluminal abnormalities in 16 patients. Associated calcification was evident in 3 of the patients with a basilar fenestration and in 13 of those with the basilar septations (Figs 1 and 3). With respect to calcified basilar septations, 5 of 12 linear septations were associated with calcification, while 8 of 9 nodular septations were associated with calcification.
A total of 16 cases with incidentally detected fenestrations or septations demonstrated coincident evidence of infarction (16/80, 20%). However, 12 patients had infarction involving the anterior circulation only (12/80, 15%), while only 3 patients had evidence of posterior circulation infarction (3/80, 3.8%), and 1 patient had an embolic pattern of infarction involving both the anterior and posterior circulation (1/80, 1.3%). Of the total number of patients with evidence of infarction, only 2 had basilar septations, one involving the anterior circulation (1/21, 4.8%) and the other the posterior circulation (1/21, 4.8%).
A total of 7 cases with either a basilar fenestration or septation demonstrated coincident evidence of parenchymal hemorrhage (7/80, 8.8%). A total of 4 cases had hemorrhage involving the anterior circulation territory only (4/80, 5%), 2 cases had evidence of posterior circulation territory hemorrhage (2/80, 2.5%), and 1 case had a parenchymal hemorrhage involving both the anterior and posterior circulation territories (1/80, 1.3%). Only 2 cases with basilar septations demonstrated coincident evidence of parenchymal hemorrhage, and both involved the anterior circulation territory (2/21, 9.5%).
No cases of intracranial arterial dissection were identified. Basilar fenestrations or septations with coincident dissection of the extracranial neck circulation were seen in 6 cases (6/80,7.5%). A total of 3 patients had dissection involving the extracranial vertebral arteries (3/80, 3.8%), and the other 3 had dissection involving the extracranial internal carotid arteries (3/80, 3.8%). Extracranial vertebral artery dissection was recognized in 2 of the basilar fenestration cases (2/59, 3.4%) and 1 of the basilar septation cases (1/21, 4.8%). Extracranial internal carotid artery dissection was recognized in 2 of the basilar fenestration cases (2/59, 3.4%) and 1 of the basilar septation cases (1/21, 4.8%).
Aneurysms of the cerebral circulation were recognized in 19 cases (19/80, 23.8%). However, almost all aneurysms were present in the anterior circulation, with only a single basilar tip aneurysm noted (1/80, 1.3%) with an associated basilar septation.
No cases fitting the description of an arterial web were found within the basilar artery. An extracranial internal carotid artery carotid web was discovered in 1 patient with an associated basilar fenestration. No arterial webs were evident in cases of basilar septation. Fibromuscular dysplasia (FMD) was recognized in 5 cases (5/80; 6.3%), with an associated basilar fenestration. No cases of FMD associated with basilar septations were noted.
No cases of moderate or severe intracranial posterior circulation atherosclerosis were identified. Severe extracranial atherosclerotic stenosis or occlusion was identified in 22 patients who also were found to have fenestrations or septations (22/80, 27.5%). A total of 15 patients had severe atherosclerosis involving the anterior circulation only (15/80, 18.8%), 4 patients had evidence of severe extracranial posterior circulation atherosclerosis (4/80, 5%), and 3 patients had severe stenosis or occlusion affecting both the anterior and posterior circulation (3/80, 3.8%). Basilar fenestration cases were associated with severe anterior cerebral circulation atherosclerosis 22% of the time (13/59), while severe posterior circulation atherosclerosis was seen in only 6.8% of cases (4/59). Basilar septation was associated with severe anterior cerebral circulation atherosclerosis 8.5% of the time (5/59), while posterior circulation severe atherosclerosis was seen in 5.1% of cases (3/59). Results are summarized in the Table.
Summary of imaging findingsa
DISCUSSION
A basilar intraluminal abnormality was detectable in 2.3% of patients on CTA. Of these, 1.7% had a basilar fenestration. To our knowledge, no previous study has documented morphologic differences in the aperture of basilar fenestrations. Our results reveal there are clear variations in the spectrum of size, morphology, and appearance of basilar fenestrations with less than half of our cases conforming to a typical window-shaped appearance, a little more than half of the cases exhibiting an hourglass shape, and only a few cases exhibiting funnel morphology depicted in our illustrations. Hourglass and funnel morphologies had smaller-but-measurable apertures in the vessel wall compared with window-type fenestrations. Furthermore, to our knowledge, no previous study has documented a congenital nonatherosclerotic pattern of calcification associated with basilar fenestrations, evident in 3 cases.
No previous imaging study has focused on the prevalence of basilar septations based on CTA. Our results reveal that findings fitting the description of a basilar septation are visible on arterial imaging and exhibit a morphology best described as an intraluminal linear hypodensity without a visible arterial vessel wall aperture, wall puckering, or indentation. Basilar septations comprised 0.6% of our cases. Our results show that septations mirror the location and distribution of basilar fenestrations, with most present in the inferior third of the vessel. Because there is no theoretic inferior limit to the size of a basilar fenestration, we propose that a basilar septation is likely best conceptualized as a miniature fenestration and best referred to as an aberrant basilar fenestration. We will, therefore, refer to basilar septations in the remainder of this discussion as aBFs.
Our findings show that calcification is clearly associated with both basilar fenestrations and aBFs, further supporting the notion that they represent variations in the size of the same entity. As noted above, a nonatherosclerotic pattern of focal calcification was evident in 5.1% of basilar fenestration cases while calcification was seen in 61.9% of aBF cases. Although calcification is associated with fenestrations of any size, for reasons yet unknown, it is more common in fenestrations of smaller caliber.
Conceptualizing aBFs as tiny fenestrations has important implications. They should be interpreted as benign congenital findings. They should not be confused with dissections or intraluminal webs. Furthermore, we demonstrate important variations in the morphology of aBFs, including areas of thinning, varying thickness, and nodularity. Therefore, when associated with calcification or nodularity, aBFs should not be confused with intraluminal thrombi or emboli with or without calcification. Furthermore, our results demonstrate that there is no notable correlation between aBFs and arterial dissection, thrombosis, or emboli. This benign history contrasts with the poor prognosis of the known ischemic and hemorrhagic complications of isolated basilar dissections,18,19,20 as well as the association of arterial webs with ischemic stroke.21,22
None of our aBFs fit the morphologic description of a web or a dissection. None of the basilar septations we found were present at or near an arterial branching point and none displayed the ledge-like imaging findings of a carotid web. In addition, only one of our aBFs was associated with a posterior circulation stroke (4.8%; 1/21), and none were associated with posterior circulation hemorrhage, extracranial arterial web, or FMD. Our single case of an ICA origin web and our 5 cases of FMD were associated with classic appearing basilar fenestrations instead. Therefore, we do not find evidence to support the theory that aBFs represent either webs or a focal dissection. Of note, the presence of extracranial arterial dissection as well as anterior circulation stroke in several of our cases is thought to represent a reflection of the sample because many of our CTAs were performed for acute neurologic symptoms. Only 1 case of a basilar tip aneurysm was identified, with no posterior circulation aneurysms found at the site of basilar fenestrations or aBFs. We, therefore, believe that the concomitant basilar intraluminal findings are purely incidental, without a causal association.
We believe the detection of aBFs has important implications in the era of endovascular procedures, especially in a posterior stroke work-up. Further studies are needed to ascertain their consequences, if any, in cases of basilar catheterization or stent placement or endovascular stroke treatment. Currently, it is unclear whether they are simply displaced against the vessel wall or whether vascular damage is possible. Therefore, we believe that neurointerventionalists should likely be aware of their presence before basilar catheterization.
Our study is limited due to its retrospective nature and the lack of pathologic correlation. Nonetheless, we believe that the 2 previously published pathologic studies relating to basilar septations6,15 lend strong support to our findings. Furthermore, our study was conducted in a North American population; therefore, the possibility that racial variations exist cannot be excluded. In addition, because the size of aBFs is near the limit of imaging resolution, certain questions remain that can only be answered by careful microscopic pathologic analysis. These questions include whether areas of vanishing thickness represent thinning or partial absence, whether a microscopic arterial wall aperture remains at the vessel wall or whether it is obliterated, and whether a collapsed lumen exists within the walls of an aBF or whether the walls are fused and the extraluminal channel has been congenitally obliterated. Last, our study was conducted in an adult population without patients younger than 18 years of age. Further research is necessary to ascertain the presence of the morphologic findings as well as associated calcification in a pediatric population.
CONCLUSIONS
Basilar septations are evident on 0.6% of CTAs and most likely represent and should be referred to as aberrant basilar fenestrations. They should not be misinterpreted as focal dissections, arterial webs, intraluminal thrombi, or emboli with or without calcification. We believe that the detection of aBFs has important theoretic implications in the era of endovascular procedures, and further studies are needed to ascertain their consequences in cases of planned basilar catheterization or stent placement.
Key Results
Variations in the size and appearance of basilar fenestrations exist with window-, hourglass-, and funnel-shaped morphologies.
Basilar septations are evident on 0.6% of CTAs and likely represent miniature aBFs. A nonatherosclerotic pattern of focal calcification was evident in 5.1% of basilar fenestrations and 61.9% of aBFs.
aBFs should be interpreted as benign, congenital findings. They should not be confused with dissections, webs, thrombi, or emboli with or without calcification.
Basilar septations are evident on 0.6% of CTAs, most likely represent aBFs, and should be interpreted as incidental, benign, congenital findings.
Acknowledgments
We wish to acknowledge and thank Insil Choi for her expert medical illustrations helping to depict our findings.
Footnotes
Disclosures: Ajay K. Wakhloo—UNRELATED: Consultancy: Stryker Neurovascular, Cerenovus Johnson & Johnson, Philips Healthcare, NovaSignal, ThrombX, InNeuroCo; Grants/Grants Pending: Medtronic, Philips Healthcare, Deinde Medical*; Patents (Planned, Pending or Issued): Patents with Medi-Solve and Cordis Neurovascular; Stock/Stock Options: Penumbra, BSC Group, InNeuroCo, ThrombX, Nova Digital, Deinde Medical, Analytic 4 Life. *Money paid to the institution.
References
- Received September 17, 2020.
- Accepted after revision November 5, 2020.
- © 2021 by American Journal of Neuroradiology





{kind=link}
{kind=link}
{kind=link}