
Abstract
SUMMARY: 3D rotational angiography provides remarkable spatial resolution for cerebrovascular disorders; however, it cannot be integrated directly into gamma knife planning due to the discrepancy of DICOM “tag” information, and most physicians still cannot benefit from 3D rotational angiography. Here, we describe a simple and easy technique to enable the integration of 3D rotational angiography.
ABBREVIATIONS:
- GKRS
- gamma knife stereotactic radiosurgery
- 3DRA
- 3D rotational angiography
Gamma knife stereotactic radiosurgery (GKRS) is an image-guided radiation therapy characterized by its high geometric accuracy; thus, no treatment margin is usually required when circumscribing the target. This feature, in conjunction with its sharp dose fall-off, enables high-dose irradiation in a single session; however, successful radiosurgery is highly dependent on the quality of radiographic images used.
GKRS has been accepted as one of the standard therapeutic modalities for small-to-medium arteriovenous malformations.1⇓⇓⇓⇓⇓⇓⇓–9 Currently, biplanar DSA and CT angiography or MR imaging or both are commonly used in most institutions.10⇓⇓⇓⇓–15 Recently, advances in modern endovascular suites and newer generation flat panel detectors with C-arm systems have enabled acquisition of 3D rotational angiography (3DRA), providing remarkable spatial resolution for cerebrovascular disorders. Indeed, 3DRA is beginning to be used in the treatment planning of other modalities of stereotactic radiation therapy, including CyberKnife (Accuray, Sunnyvale, California), XKnife (Integra LifeSciences, Plainsboro, New Jersey), and Trilogy (Varian Medical Systems, Palo Alto, California), contributing to improved accuracy of the treatment planning.16⇓–18 One remaining issue is that 3DRA cannot be integrated directly into GKRS planning because the planning software (Leksell GammaPlan; Elekta Instruments, Stockholm, Sweden) does not accept 3DRA. Moreover, very few studies have described the effectiveness of 3DRA on GKRS planning, though they do not state a detailed integration method.19⇓–21 Thus, most physicians still cannot benefit from 3DRA. Here, we show a very simple method to integrate 3DRA into GKRS planning.
Techniques
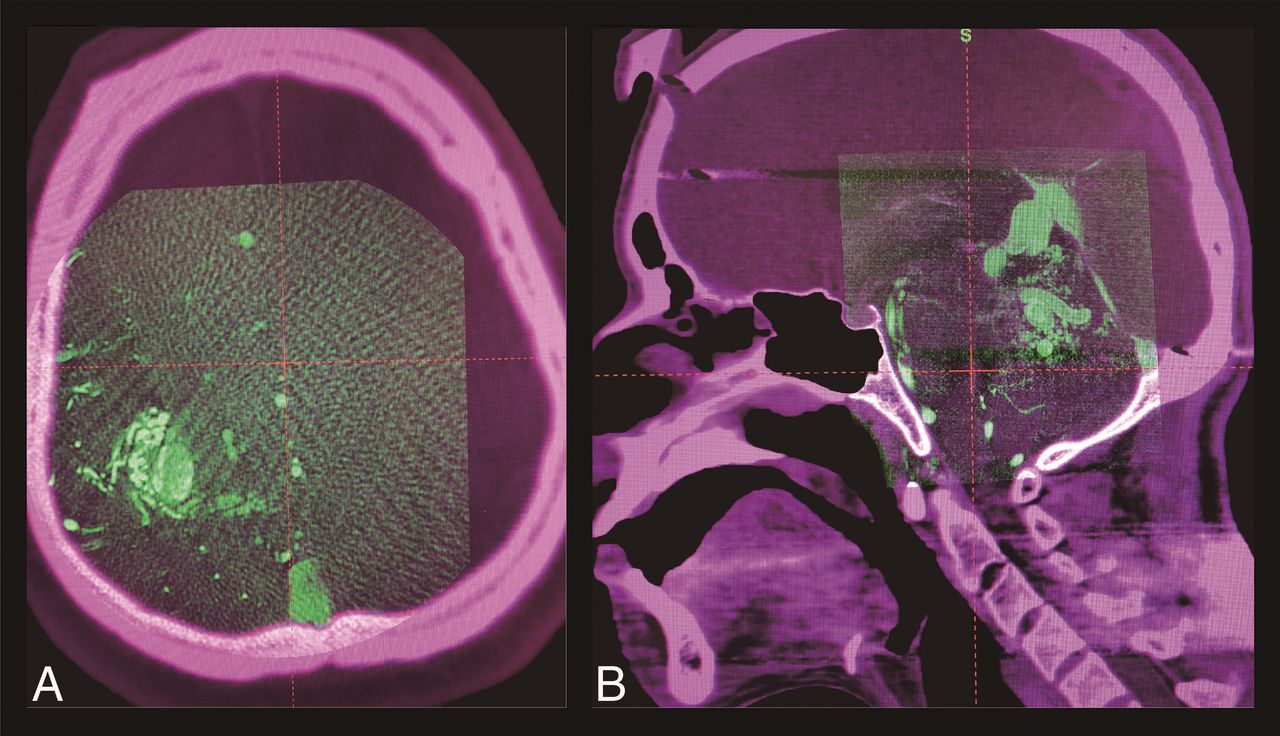
Before the day of treatment, we usually perform MR imaging (mainly time-of-flight MR angiography, supplemented by T2 and gadolinium-enhanced T1 images) for preplanning. As in the usual preparations for GKRS, the Leksell frame (Elekta Instruments) is set on the patient's head with the patient under sedation with local anesthesia. Then, the patient is transferred to the angiographic suite (Allura Xper FD20/10; Philips Healthcare, Best, Netherlands). Along with conventional DSA, 3DRA is acquired using the programmed acquisition protocol (3DRA mode). The amount of contrast medium used and preinjection delay are individually determined by neuroendovascular surgeons; briefly, 1–3 mL/s of contrast medium is continuously injected with a 1.5- to 2.0-second preinjection delay during the rotation of the C-arm. Because 3DRA could be easily coregistered to stereotactic CT if 3DRA contained enough bony tissue, a large-sized detector is generally preferred for precise image coregistration (Fig 1A). On the contrary, the smallest 8-inch detector could be used when the nidus is located near the skull base (basal ganglia, posterior fossa, and so forth) because acquired images spontaneously contain a large portion of bony tissues (Fig 1B). The obtained volume dataset is automatically transferred to the preinstalled workstation (XtraVision; Philips Healthcare), with which further reconstruction is performed with a 2563- or 5123-resolution voxel matrix in a planned cube-shaped FOV with preset side lengths of 34.96, 52.18, 69.92, or 104.36 mm. We mostly use a 69.92-mm side-length cube with a 2563-resolution voxel matrix to maintain the balance between spatial resolution and contrast resolution; thus, spatial resolution is roughly calculated as 0.27 mm. Then, the DICOM “tag” technique is corrected from XA into CT in our software so that the GammaPlan can recognize the 3DRA properly as a CT-like image. Once the 3DRA is installed in the GammaPlan, image coregistration to stereotactic CT will be automated using the preinstalled coregistration function. A step-by-step instruction manual to integrate 3DRA is shown in On-line Figure. Detailed case illustrations are shown in Fig 2.
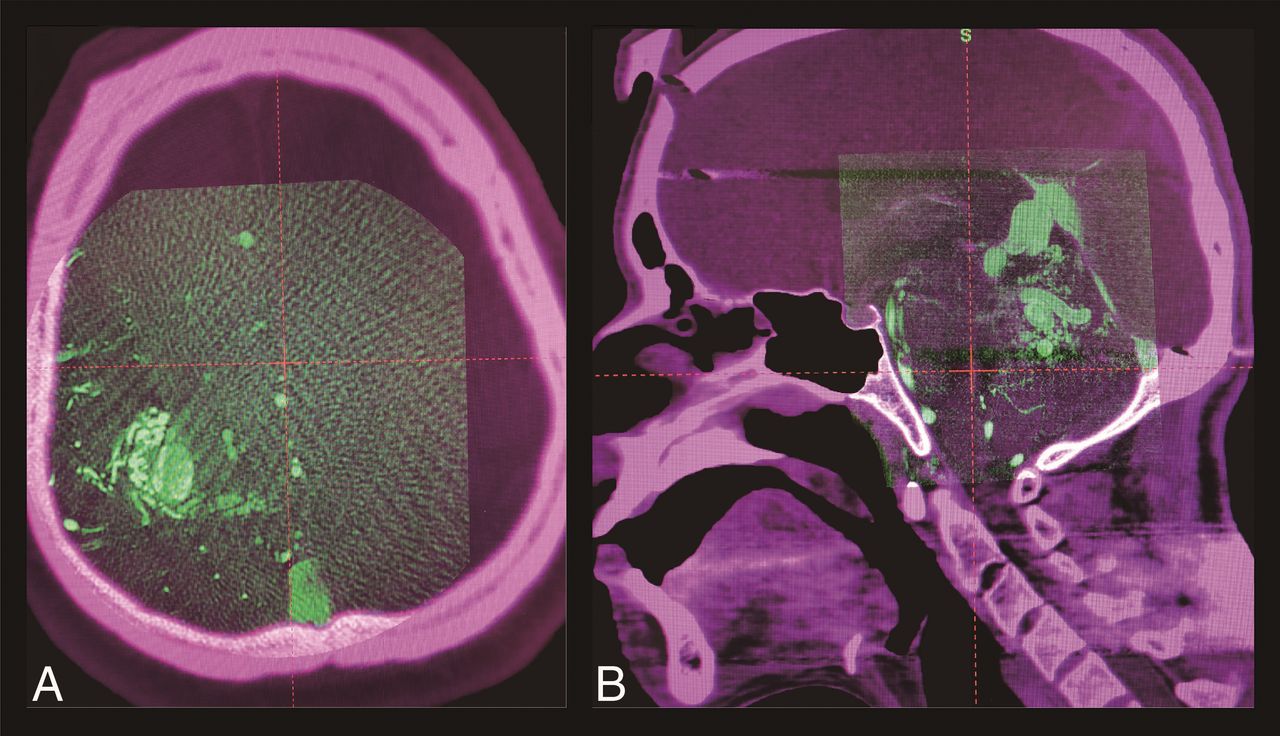
3D rotational angiography images obtained with a large (A) and an 8-inch detector (B) are coregistered to each stereotactic CT image on treatment-planning software (GammaPlan).

A 34-year-old woman with an unruptured, small, left medial frontal arteriovenous malformation, once treated with gamma knife (A). The small remnant nidus persisted at 3.5 years from the initial radiosurgery (B, a red arrowhead shows the remnant nidus). The actual treatment planning of the secondary treatment (C) shows that 3D rotational angiography (left column) successfully depicts the faint remnant, while both time-of-flight (middle column) and gadolinium-enhanced T1 images (right column) fail to depict it. The nidus was finally obliterated (D) at 1.5 years from the secondary treatment. Yellow lines show the prescription isodose lines.
Discussion
With the above-described simple contrivance, 3DRA can readily be used for GKRS planning. The strength of this technique is its accessibility. GammaPlan cannot directly accept 3DRA because of the discrepancy of DICOM tag information; accordingly, we must address this issue. No changes are required in the geometric or patient information; thus, the image quality itself is intact. Because 3DRA is a CT-like image, being characteristic of the finest spatial resolution for high-contrast objects with poor contrast resolution and thus having many features common to CT,22,23 stereotactic CT would be the best reference image for the coregistration.18 By means of high-definition images, physicians can not only reduce unwanted waste radiation to the surrounding brain tissues but also enable a safe prescription of high radiosurgical doses, enough to obliterate the nidus, which might theoretically lead to improvement in the obliteration rate as well as a decrease in radiation-induced adverse events. However, this article is only a technical report, and the actual clinical outcomes should be further examined.
Although 3DRA mode is preferred in our institution, contrast-enhanced conebeam CT with a small targeted FOV (high-resolution XperCT mode; Philips Healthcare) is also available in our angiographic suite. This acquisition mode provides superior spatial resolution with a long acquisition time (20 seconds), using a slow C-arm rotation and an 8-inch detector, which might be better for very small arteriovenous malformations. However, use of the high-resolution XperCT mode might raise a concern about coregistration. Notably, images containing a large portion of the cranium as well as skull base bone are important for precise coregistration; the use of a smaller detector contributes to further increased spatial resolution but also loses images of the surrounding cranium and skull base, leading to difficulty in coregistration. We usually perform stereotactic CT after finishing angiography so that the contrast medium remaining in the blood vessels can provide additional information of vascular anatomies, which may enhance the quality of image coregistration. Further research is desirable to examine the coregistration accuracy to ensure the quality of the prescription of the therapeutic radiation dose.
Moreover, when a nidus receives blood flow from >2 vessels, the precise nidus contour is shown as the summation of parts of the nidus obtained by cannulation in each vessel. Thus, it is quite important to perform 3- or 4-vessel angiography and judge the involvement to avoid underestimation of the whole nidus angioarchitecture.
Although 3DRA provides superior resolution for angioarchitectures of vascular lesions, we recommend creating radiosurgical plans by meticulously comparing all the available imaging modalities. Particularly, MR imaging exhibits excellent contrast resolution and provides a better understanding of the surrounding functional brain anatomies, and DSA enables surgeons to instinctively recognize a spatial expanse of the nidus. Notably, surgeons should manipulate the DICOM header at their own risk because carelessly manipulating DICOM could spoil the quality of the images. Meticulous care must be taken not to change important information in the DICOM header other than technique because it could alter spatial relationships. Given the above reasons, 3DRA should not be used as a main technique but as reference information during radiosurgical planning.
Conclusions
We describe a simple, easy-to-access technique to enable integration of 3DRA into GKRS planning, which could provide the highest resolution for angioarchitectures of vascular lesions. The present method remains preliminary; thus, the created treatment plans should be validated in comparison with the conventional planning method. Further research is desirable to assess the effect of this technique on the actual radiosurgical outcomes.
Footnotes
Disclosures: Hirotaka Hasegawa—RELATED: Grant: JSPS KAKENHI, Comments: grant No. JP17K16628.
This study was supported by Japan Society for the Promotion of Science (JSPS) KAKENHI grant (No. JP17K16628).
Indicates open access to non-subscribers at www.ajnr.org
References
- Received April 4, 2018.
- Accepted after revision June 12, 2018.
- © 2018 by American Journal of Neuroradiology





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.